Background: Hospital malnutrition is a global complex, multi-factorial problem, mainly due to lack of appropriate awareness. Hospital malnutrition negatively impacts patient's recovery and increases hospitalization cost. Materials and methods: We assessed hospitalized patients during the first 24-48 hours. Nutritional risk screening (NRS 2002) was applied; anthropometric and dietary parameters were evaluated. Objective: 1) To assess nutritional status and risk of malnutrition in patients admitted to a Mexican public hospital. 2) To determine the frequency of patients who did not meet their energy and protein needs. Results: We evaluated a total of 568 patients. Risk of malnutrition was present in 3.6% of patients at admission while 84% of them were at risk of malnutrition after prolonged hospitalization. A BMI<20 Kg/m2 was observed in 7.4% of the patients, whereas 49.5% were classified and obese or overweight. Weight loss >10% was seen in 32.9% of the patients. Food intake showed that in average hospital patients consumed 50% of their caloric requirements and 39% of protein requirements; only 42% of the patients had a food intake between 70-100%. Conclusions: Hospital malnutrition is a complex issue with both personal and institutional etiological factors. Healthcare institutions must improve awareness and training of personnel and the quality of hospital nutrition/food service to improve the addressing of hospital malnutrition.
Hospital malnutrition results in a deterioration of multiple organ systems. This cumulative nutritional deficit is usually underestimated 1. Initial symptoms of hospital malnutrition manifest themselves clinically as anorexia, dysphagia, and an inability to digest and absorb nutrients. Nutritional deficiency is directly related to loss of nutrients, increase in nutritional requirements, lack of consumption to meet such requirements, medications, prescription of restrictive diets, prolonged fasting, inability to eat without assistance and badly organized hospital food services. 2, 3 Additionally, studies show that patients exhibit a higher risk of worsening or developing malnutrition during hospital stay than at the time of admission 1, 4, 5, 6.
Hospital malnutrition affects patients adversely in terms of effectiveness of treatment and increases the possibility of complications, especially infections. 7 It increases morbidity and mortality. 1, Hospital malnutrition also leads to loss of muscle mass and an alteration in the healing process therefore compromising the quality of life. 8, 9 Hence there is an urgent need to address hospital malnutrition, in order to optimize clinical outcomes and for cost effectiveness of health care 1, 5, 6.
Medical institutions hospital malnutrition prevalence is an indicator of inadequate quality assurance. Previous studies have shown that hospital malnutrition affects patients and medical institutions costs 6, 7, 8.
Several studies reported malnutrition however this diagnosis depends of their criteria classification. In 2003, the ELAN (Latin American Malnutrition Study) study, aimed to assess nutritional status in 13 Latin countries with Subjetive global assessment (SGA) and concluded that 30-50% of patients admitted to the hospital were malnourished 9. This year Correia and Waitzberg, reported high mortality rates in patients with undernourished compared with those well-nourished, which resulted in 12.4% and 4.7%, respectively 7. However in 2008 Fuchs V et al. in Mexico reported malnutrition in 21% of patients evaluated with BMI, and 69% with % of weight loss 10. Burgos et al. in 2011, point out that hospital stay among undernourished patients is 5 days longer, than that for those in healthy conditions 11.
Hospital nutrition services tend to offer an unappealing menu, consisting of low quality ingredients, which are poorly adapted to specific requirements 3. Lack of nutritional assessment is detrimental to high quality hospital nutrition service. This may be attributed to the lack of adequate number and availability of dietitians 12.
During admission, protocols and screening tools are required to identify patients at a higher risk of malnutrition to prioritize interventions. Other patients may be evaluated on a weekly basis 9. These screening tools include a dietary survey, physical examination, and evaluation of anthropometric variables supported by biochemical parameters when indicated 11, 12, 13, 14.
Commonly used screening tools are: Subjective Global Assessment (SGA) 15, Mini Nutritional Assessment (MNA) 16, Malnutrition Universal Screening Tool (MUST) 17 and Nutritional Risk Screening (NRS-2002) 18. Nutritional Risk Screening (NRS-2002) was developed by Kondrup et al., has been validated in Europe and Asia. It presents a specificity and sensibility of >80% among different pathologies and ages 18. The NRS-2002 consists of 2 scores:
1. Assessment of nutritional status: weight loss in the last six months, decrease in food intake, and a BMI of less than 20.5 kg/m2.
2. Assessment of the patients’ present condition/disease.
Both scores are added, and 1 point is included if the patient is ≥70 years old. If the result is 3 or more, an immediate nutritional intervention is required 19.
This study aims to assess a random number of patients at the Hospital General de México, using the NRS 2002 tool and compare their nutritional requirements with their consumption during hospital stay. If nutritional requirements were not met, the reasons for the same were recorded.
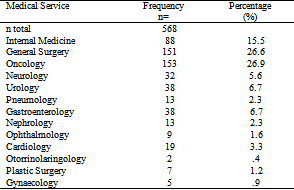
Hospital General de Mexico is a tertiary public hospital with over 1500 beds. A cross sectional study was designed to evaluate hospitalized patients. Patients were randomly selected from 13 different wards of the Hospital General de Mexico that included: Internal Medicine, General Surgery, Oncology, Neurology, Urology, Pneumology, Gastroenterology, Nephrology, Ophthalmology, Cardiology, Otorrinolaringology, Plastic Surgery, Gynaecology. This study was approved by the ethical and research committee of Hospital General de Mexico with the number DI/13}7113/3/56.
Hospitalized patients of both genders with a minimum stay of 24 hours, which were ≥18 years old, conscious and without language barriers were eligible participants. Patients were verbally informed of the purpose of the study and participation was voluntary.
Exclusion criteria included: <18 years of age, intensive care unit (ICU) patients, pediatric and psychiatry admissions, patients unable to give their consent (e.g. language barrier, unconscious, or mentally impaired) and those who had enteral or parenteral nutrition.
From the hospital records, demographic variables like age and gender, clinical details including hospital ward, length of stay and diagnosis were obtained. Diet related variables like oral diet, fasting, oral nutrition, anthropometric variables such as size, actual weight, usual weight, weight loss (in the last six months, as reported by the patient), weight loss percentage and ideal weight (calculated using the Hamwi formula) 20. If the observed food intake was <100%, patients were further questioned to ascertain the reasons (food service deficiencies or clinical condition).
Nutritional risk was assessed through the Nutritional Risk Screening (NRS-2002) taking into account the diagnosis, weight loss, body mass index and energy intake. SPSS (Statistical Product and Service Solution) version 22.0 (IBM Innovation Centers®, IL, USA) 21, was used for statistical analysis. Data were collected and organized through Microsoft Office Excel in a database.
Variables were evaluated considering their characteristics and distribution Continuous variables were reported in a descriptive analysis using medium, range and standard deviation (SD). For non-continuous variables such as using body mass index (BMI) classification, weight loss's percentage, ideal weight percentage and NRS-2002 frequencies were used.
A total of 600 surveys were done out of which 32 were discarded as they did not meet the criteria and/or had data capture errors. The analysis was developed with 568 patients, 41.2% was males and 58.8% was female. The average age of the studied population was 46.9 ± 16 years. Table 1 details the analyzed sample size of 568 hospitalized patients. Oncology ward (26.9%), general surgery (26.6%) and internal medicine (15.5%) represented the 69% of the patients. The duration of hospitalization of hospitalization was 7.39 ± 9.04 days. Table 2 shows a descriptive analysis of the anthropometric variables. The average of weight loss in hospitalized patients was 6.8 ± 11 % of usual weight.
An average of fasting was 1.7 days. In regard of daily calories and protein intake in hospitalized patients was quantified a 765.2 kcal and 31.76 g of protein of oral intake, which allowed 50% of their requirements (Table 3). On the other hand, patients with oral diet (OD) were 22.5% of total patients (due to scheduled diagnostic studies, and/or clinical procedures). Patients consumed 42% of patients had a food consumption between 70-100% of the diet provided by the Hospital Nutrition Service, while only 34.6% of patients had a food consumption less than 60% of hospital diet.
Nutritional status by BMI in Table 4 present a 7.4% of prevalence of malnutrition, 43% of normal weight and 49.5 of higher BMI either overweight or obesity. Nutritional risk screening at the time of admission showed that 13.6% of the patients were at risk of malnutrition but 86.4% of the patients were at risk when hospitalized for a long time.
Hospital malnutrition continues to be a challenge although a lot of research studies and literature has been published on the subject. Our study concluded that 13.6% of patients were at risk of malnutrition upon admission and one week after hospitalization the risk increased to 86.4%. Literature reports risk of malnutrition in between 30-50%of the patients 10, 22, 23, 24. Euro OOPS study is a multicenter research conducted in 26 countries using NRS-2002 as screening tool. This study reported a prevalence of hospital malnutrition in 32.6% of patients 22. PREDyCES study in spain report in 2012 a prevalence of 23.7%, however in Mexico studies reported report 21-69% 10 that result a variable prevalence depending of tool used and the population assessed, due there is a pathologies more vulnerable like cancer that report 40.5% of nutritional risk 23.
Both personal and organizational factors cause hospital malnutrition. Age, state of mind, disease, lack of autonomy to feed oneself or chew, and dietetic restrictions are personal risk factors. Cancer, neurological pathologies, hematological diseases, cardiovascular diseases and lifestyle conditions like diabetes are closely related to the development of malnutrition. 24 Lack of skill to diagnose and treat malnutrition by the hospital staff, lack of reports on patients food intake and weight loss, and the lack of communication among the different hospital services and nutrition departments, failure to come up with specially adapted diets to meet the patient's requirements and diet restrictions are the organizational factors responsible for hospital malnutrition.
Hospital malnutrition affects patients clinically and economically. It increases the length of the hospital stay and/or increases the rate of mortality and morbidity. Also prolonged hospitalization implies greater treatment costs. 25, 26 Studies have shown that under-nourished patients have longer hospital stays, reported differences between 6.9 ±7.3 days, versus 4.6 ±5.6 for non malnourished patients. 27, 28 In addition, malnutrition increases hospitalization costs from 24 to 70%. 29
Due to the absence of a gold standard, the prevalence of hospital malnutrition may vary depending on the population and the tools used to evaluate it. Therefore, several investigations have studied and developed methods to assess a patients’ nutritional status, with the intention of creating an appropriate diagnostic tool. Such tools have been internationally validated, thanks to their high specificity and speed in its application within a clinical environment. 30
The results of our study show that there is a high incidence of hospital malnutrition. BMI alone is an indicator that proves insufficient to diagnose malnutrition, and the high incidence of obese and overweight patients make it even more difficult.5, 31 Our study allows us to confirm the existence of malnutrition in overweight or obese patients, who are at a higher risk of malnutrition due to the increase in nutrient needs because of altered nutrition equilibrium and other disease process. It is important that complications are detected on time. 32
Several studies of nutrition assessment conducted in hospitals like our own, and found a reported prevalence of malnutrition of 63-71%, within an average hospital stay of 9 days. The prevalence of hospital malnutrition is similar in several hospitals within the Mexico City area. Although there is difference in the reported results, this may be due to the lack of a gold standard in malnutrition assessment methods. 33, 34
Another important finding of our study is that a significantly higher percentage of patients are at risk of malnutrition after prolonged stay at hospital. Lack of malnutrition risk detection at admission stage and lack of quality in hospital food services caused cumulative nutritional deficits, increasing the risk of malnutrition progression in hospitalized patients.
In our study, a wide proportion of the sample was not eating the required macronutrients. In addition, about 84.4% were malnourished even after eating 70-100% of the food provided by the hospital. Only 50% of their energy and 40% of their protein requirements were covered. This implies the need of close supervision of the Hospital Nutrition Services. Johansen et al, have also published similar results, reflecting adequacy percentages less than 90% in most of the hospital populations, thus complementary nutrition supplementation is needed to be able to meet their needs. 35
The main limitation of this study is that the analyzed variables depended on patient’s own diet recall. Hence this was subjective and prone to biases. A standardized system should be established to document the quantity of food provided and the amount unconsumed. 36
The present study verifies the existence of a high prevalence of malnutrition in hospitalized patients, based on a number of different criteria, using anthropometric and dietetic variables as well as the NRS-2002 screening tool. Energy and protein intake did not always meet the patient’s requirements. The solution to this problem lies within the Hospital Institution’s procedures. Changes in menus to adapt to individual nutritional need of patients are necessary.
Though hospital malnutrition is widely reported and investigated, the prevalence of malnutrition is reaching alarming levels. Hence awareness development is crucial. Training health professionals to diagnose and treat hospital malnutrition is of utmost importance. Hospitals and healthcare institutions need an accurate, responsible and established system for improving the quality of Hospital Nutrition service.
Authors declare that there are no conflicts of interest or competing interests in this research paper.
The authors are grateful to the Hospital General de Mexico for its contribution in the development of this study.
We also want to thank Krishnan Sriram, MD and Mangala Bhavani, RD for their help with the manuscript.
| [1] | S. Montoya-Montoya, N. Múnera-García. Efecto de la intervención nutricional temprana en el resultado clínico de pacientes con riesgo nutricional. Nutr Hosp 2014; 29: 427-436. | ||
| In article | PubMed | ||
| [2] | White JV, Guenter P, Jensen G, Malone A, Schofield M. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J Parenter Enteral Nutr 2012; 36: 275-83. | ||
| In article | View Article PubMed | ||
| [3] | Garcia de Lorenzo A, Alvarez J, Planas M, Burgos R, Araujo K. Multidisciplinary consensus on the approach to hospital malnutrition in Spain. Nutr Hosp. 2011; 26(4): 701-710. | ||
| In article | PubMed | ||
| [4] | Gout SB, Barker AL, Crowe CT. Malnutrition identification, diagnosis and dietetic referrals: Are we doing a good enough job? Nutr Diet 2009; 66: 206-211. | ||
| In article | View Article | ||
| [5] | Vesga A, Gamboa E. Riesgo de malnutricion asociado a baja ingesta alimentaria, estancia hospitalaria prolongada y reingreso en un hospital de alto nivel de complejidad en Colombia. Nutr Hosp. 2015; 32(3): 1308-1314. | ||
| In article | View Article | ||
| [6] | Rodriguez BJ, Laquaniti N, Merkel MC, Villagra A. Política nutricional activa en la implementación del soporte nutricional hospitalario; resultados de un estudio obervacional. Nutr Hosp. 2014; 30(2):452-447. | ||
| In article | |||
| [7] | Correia ML, Waitzberg DL. The impact of malnutrition on morbidity, mortality, lenght of stay and costs evaluated through a multivariate model analysis. Clin Nutr 2003; 22(3): 235-239. | ||
| In article | View Article | ||
| [8] | G. Mercadal-Orfila, J. Lluch-Taltavull, C. Campillo-Artero, M. Torrent-Quetglas. Association between nutritional risk based on the NRS-2002 test and hospital morbidity and mortality. Nutr Hosp 2012; 27(4):1248-1254). | ||
| In article | PubMed | ||
| [9] | Correia Ml, Campos AC. Prevalence of hospital malnutrition in Latin America: the multicenter ELAN study. Nutrition. 2003; 19(10): 823-825. | ||
| In article | View Article | ||
| [10] | V. Fuchs., D. Mostkoff, G.Gutiérrez Salméan, O. Amancio. Estado nutricio en pacientes hospitalizados en un hospital público de la cuidad de México. Nutr Hosp 2008;23(3): 294-303. | ||
| In article | PubMed | ||
| [11] | Burgos R, et al. Prevalence of malnutrition and its etiological factors in hospitals. Nutr Hosp 2012; 27(2): 469-476. | ||
| In article | PubMed | ||
| [12] | P. Llopis-Salvia, P.Luna-Catayud, J. A. Avellana-Zaragoza, R.Bou-Monterde. Organización y funcionamiento de la atención nutricional hospitalaria: el modelo implantado en el Hospital Universitario de la Ribera. Nutr Hosp 2012; 27: 529-536. | ||
| In article | PubMed | ||
| [13] | Curtis Morris R. Malnutrition in hospitalized patients: diagnosis and treatment. Western J Med 1986; 144(1): 63-7. | ||
| In article | View Article | ||
| [14] | Seidener DL. Nutritional issues in the surgical patients. Cleveland Clin J Med 2006; 63(Supl. 1): S77-81. | ||
| In article | View Article | ||
| [15] | Detsky A S, McLaughlin J R, Baker J P et al. What is subjective global assessment of nutritional status? J Parenter Enteral Nutr 1987; 11: 8-13. | ||
| In article | View Article PubMed | ||
| [16] | Guigoz Y, Vellas B, Garry PJ. Assessing the nutritional status of the elderly: the Mini Nutritional Assessment as part of the geriatric evaluation. Nutr Rev 1996; 54: S59. | ||
| In article | View Article PubMed | ||
| [17] | King CL, Elia M, Stroud MA, Stratton R. The predictive validity of the malnutrition screening tool ('MUST') with regard to morality and length of stay in elderly patients. Clinical Nutrition 2003; 22: S4. | ||
| In article | View Article | ||
| [18] | Kondrup J, Rasmussen HH, Hamberg O, Stanga Z. Nutritional Risk Screening (NRS-2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003; 22(3): 321-336. | ||
| In article | View Article | ||
| [19] | Carney E, Meguid M. Current concepts in nutritional assessment. Arch Surg. 2002; 137(1): 42-45. | ||
| In article | View Article PubMed | ||
| [20] | Korfalii G, Gündogdu H, Aydintg S, Bahar M, Besler T, MoralAR, Oguz M, Sakarya M, Uyar M, Kilçturgay S. Nutritnal riskof hospitalized patients in Turkey. Clin Nutr 2009; 28:533-537. | ||
| In article | View Article PubMed | ||
| [21] | SPSS Statistics Desktop Version 22.0 available packages. License added by on line for payment in: https://www-01.ibm.com/marketing/iwm/iwmdocs/tnd/data/web/en_US/trialprograms/W110742E06714B29.html | ||
| In article | View Article | ||
| [22] | Sorensen J, Kondrup J, Prokopowicz J, Schiesser M, Krahen- biihl L, Meier R, et al. Eu-roOOPS: An international, multicentre study to implement nutritional risk screening and evaluate clinical outcome. Clin Nutr 2008; 27: 340-9. | ||
| In article | View Article PubMed | ||
| [23] | Alvarez K, Delgadillo T, Garcia A, Alatriste G, Fuchs-Tarlovsky Vanessa. Prevalencia de riesgo de desnutrición hospitalaria evaluada en NRS-2002 en población oncológica mexicana. Nutr Hosp. 2014; 30(1): 173-178. | ||
| In article | View Article | ||
| [24] | Álvarez-Hernández J, Planas Vila M, León-Sanz M, García de Lorenzo A, Celaya-Pérez S, García-Lorda P et al. Prevalence and costs of malnutrition in hospitalized patients; the PREDyCES Study. Nutr Hosp. 2012 Jul-Aug; 27(4): 1049-59. | ||
| In article | PubMed | ||
| [25] | Hurtado-Torres G. Incidencia, impacto clínico-económico y clasificación de la desnutrición hospitalaria. Med Int Mex 2003; 29: 290-298. | ||
| In article | View Article | ||
| [26] | Iizaka S, Okuwa M, Sugama J, Sanada H. The impact of malnutrition and nutrition-related factors on the development and severity of pressure ulcers in older patients receiving home care. Clin Nutr 2010; 29: 47-53. | ||
| In article | View Article PubMed | ||
| [27] | Penié J, Cuban Group for the Study of Hospital Malnutrition. State of malnutrition in Cuban hospitals. Nutrition 2005; 21: 487-97. | ||
| In article | View Article PubMed | ||
| [28] | Norman K, Pichard C, Lochs H, Pirlich M. Prognosticimpact ofdisease-related malnutrition. Clin Nutr 2008; 27: 5-15. | ||
| In article | View Article PubMed | ||
| [29] | Elia M. The economics of malnutrition. Nestle Nutr Workshop Ser Clin Perform Programme 2009; 12: 29-40. | ||
| In article | View Article PubMed | ||
| [30] | Baker L, Gout B, Crowe T. Hospital Malnutrition; prevalence, identification and impact on patients and the healthcare system. Int J Environ Res Public Health 2011; 8: 514-527. | ||
| In article | View Article PubMed | ||
| [31] | White J, et al. ASPEN / AND characteristics recommended for the identification and documentation of adult malnutrition. JAcad Nutr Diet. 2012; 11(5): 2012. | ||
| In article | |||
| [32] | Santana S. State of malnutrition in Cuban hospitals; a needed update. Nutr Hosp 2015; 31/5): 1900-1909. | ||
| In article | View Article | ||
| [33] | Perez CE, Ruiz VS. Desnutrición hospitalaria: prevalencia en el Hospital Juárez de México. Rev Hosp Jua Mex 2010; 774(4): 234-238. | ||
| In article | View Article | ||
| [34] | Baca MG, Peña CM. Prevalencia de sub-alimentación de pacientes con soporte enteral en el Centro Médico Lic. Adolfo López Mateos. Nutr Hosp. 2015; 31(4): 1597-1602. | ||
| In article | View Article | ||
| [35] | Loser C. Malnutrition in hospital: the clinical and economic implications. Dtsch Arztebl Int 2010; 107: 911-7. | ||
| In article | PubMed PubMed | ||
| [36] | Johansen N. Effect of nutritional support on clinical outcome in patients at nutritional risk. Clin Nutr 2004; 23: 539-50. | ||
| In article | View Article PubMed | ||
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | S. Montoya-Montoya, N. Múnera-García. Efecto de la intervención nutricional temprana en el resultado clínico de pacientes con riesgo nutricional. Nutr Hosp 2014; 29: 427-436. | ||
| In article | PubMed | ||
| [2] | White JV, Guenter P, Jensen G, Malone A, Schofield M. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J Parenter Enteral Nutr 2012; 36: 275-83. | ||
| In article | View Article PubMed | ||
| [3] | Garcia de Lorenzo A, Alvarez J, Planas M, Burgos R, Araujo K. Multidisciplinary consensus on the approach to hospital malnutrition in Spain. Nutr Hosp. 2011; 26(4): 701-710. | ||
| In article | PubMed | ||
| [4] | Gout SB, Barker AL, Crowe CT. Malnutrition identification, diagnosis and dietetic referrals: Are we doing a good enough job? Nutr Diet 2009; 66: 206-211. | ||
| In article | View Article | ||
| [5] | Vesga A, Gamboa E. Riesgo de malnutricion asociado a baja ingesta alimentaria, estancia hospitalaria prolongada y reingreso en un hospital de alto nivel de complejidad en Colombia. Nutr Hosp. 2015; 32(3): 1308-1314. | ||
| In article | View Article | ||
| [6] | Rodriguez BJ, Laquaniti N, Merkel MC, Villagra A. Política nutricional activa en la implementación del soporte nutricional hospitalario; resultados de un estudio obervacional. Nutr Hosp. 2014; 30(2):452-447. | ||
| In article | |||
| [7] | Correia ML, Waitzberg DL. The impact of malnutrition on morbidity, mortality, lenght of stay and costs evaluated through a multivariate model analysis. Clin Nutr 2003; 22(3): 235-239. | ||
| In article | View Article | ||
| [8] | G. Mercadal-Orfila, J. Lluch-Taltavull, C. Campillo-Artero, M. Torrent-Quetglas. Association between nutritional risk based on the NRS-2002 test and hospital morbidity and mortality. Nutr Hosp 2012; 27(4):1248-1254). | ||
| In article | PubMed | ||
| [9] | Correia Ml, Campos AC. Prevalence of hospital malnutrition in Latin America: the multicenter ELAN study. Nutrition. 2003; 19(10): 823-825. | ||
| In article | View Article | ||
| [10] | V. Fuchs., D. Mostkoff, G.Gutiérrez Salméan, O. Amancio. Estado nutricio en pacientes hospitalizados en un hospital público de la cuidad de México. Nutr Hosp 2008;23(3): 294-303. | ||
| In article | PubMed | ||
| [11] | Burgos R, et al. Prevalence of malnutrition and its etiological factors in hospitals. Nutr Hosp 2012; 27(2): 469-476. | ||
| In article | PubMed | ||
| [12] | P. Llopis-Salvia, P.Luna-Catayud, J. A. Avellana-Zaragoza, R.Bou-Monterde. Organización y funcionamiento de la atención nutricional hospitalaria: el modelo implantado en el Hospital Universitario de la Ribera. Nutr Hosp 2012; 27: 529-536. | ||
| In article | PubMed | ||
| [13] | Curtis Morris R. Malnutrition in hospitalized patients: diagnosis and treatment. Western J Med 1986; 144(1): 63-7. | ||
| In article | View Article | ||
| [14] | Seidener DL. Nutritional issues in the surgical patients. Cleveland Clin J Med 2006; 63(Supl. 1): S77-81. | ||
| In article | View Article | ||
| [15] | Detsky A S, McLaughlin J R, Baker J P et al. What is subjective global assessment of nutritional status? J Parenter Enteral Nutr 1987; 11: 8-13. | ||
| In article | View Article PubMed | ||
| [16] | Guigoz Y, Vellas B, Garry PJ. Assessing the nutritional status of the elderly: the Mini Nutritional Assessment as part of the geriatric evaluation. Nutr Rev 1996; 54: S59. | ||
| In article | View Article PubMed | ||
| [17] | King CL, Elia M, Stroud MA, Stratton R. The predictive validity of the malnutrition screening tool ('MUST') with regard to morality and length of stay in elderly patients. Clinical Nutrition 2003; 22: S4. | ||
| In article | View Article | ||
| [18] | Kondrup J, Rasmussen HH, Hamberg O, Stanga Z. Nutritional Risk Screening (NRS-2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003; 22(3): 321-336. | ||
| In article | View Article | ||
| [19] | Carney E, Meguid M. Current concepts in nutritional assessment. Arch Surg. 2002; 137(1): 42-45. | ||
| In article | View Article PubMed | ||
| [20] | Korfalii G, Gündogdu H, Aydintg S, Bahar M, Besler T, MoralAR, Oguz M, Sakarya M, Uyar M, Kilçturgay S. Nutritnal riskof hospitalized patients in Turkey. Clin Nutr 2009; 28:533-537. | ||
| In article | View Article PubMed | ||
| [21] | SPSS Statistics Desktop Version 22.0 available packages. License added by on line for payment in: https://www-01.ibm.com/marketing/iwm/iwmdocs/tnd/data/web/en_US/trialprograms/W110742E06714B29.html | ||
| In article | View Article | ||
| [22] | Sorensen J, Kondrup J, Prokopowicz J, Schiesser M, Krahen- biihl L, Meier R, et al. Eu-roOOPS: An international, multicentre study to implement nutritional risk screening and evaluate clinical outcome. Clin Nutr 2008; 27: 340-9. | ||
| In article | View Article PubMed | ||
| [23] | Alvarez K, Delgadillo T, Garcia A, Alatriste G, Fuchs-Tarlovsky Vanessa. Prevalencia de riesgo de desnutrición hospitalaria evaluada en NRS-2002 en población oncológica mexicana. Nutr Hosp. 2014; 30(1): 173-178. | ||
| In article | View Article | ||
| [24] | Álvarez-Hernández J, Planas Vila M, León-Sanz M, García de Lorenzo A, Celaya-Pérez S, García-Lorda P et al. Prevalence and costs of malnutrition in hospitalized patients; the PREDyCES Study. Nutr Hosp. 2012 Jul-Aug; 27(4): 1049-59. | ||
| In article | PubMed | ||
| [25] | Hurtado-Torres G. Incidencia, impacto clínico-económico y clasificación de la desnutrición hospitalaria. Med Int Mex 2003; 29: 290-298. | ||
| In article | View Article | ||
| [26] | Iizaka S, Okuwa M, Sugama J, Sanada H. The impact of malnutrition and nutrition-related factors on the development and severity of pressure ulcers in older patients receiving home care. Clin Nutr 2010; 29: 47-53. | ||
| In article | View Article PubMed | ||
| [27] | Penié J, Cuban Group for the Study of Hospital Malnutrition. State of malnutrition in Cuban hospitals. Nutrition 2005; 21: 487-97. | ||
| In article | View Article PubMed | ||
| [28] | Norman K, Pichard C, Lochs H, Pirlich M. Prognosticimpact ofdisease-related malnutrition. Clin Nutr 2008; 27: 5-15. | ||
| In article | View Article PubMed | ||
| [29] | Elia M. The economics of malnutrition. Nestle Nutr Workshop Ser Clin Perform Programme 2009; 12: 29-40. | ||
| In article | View Article PubMed | ||
| [30] | Baker L, Gout B, Crowe T. Hospital Malnutrition; prevalence, identification and impact on patients and the healthcare system. Int J Environ Res Public Health 2011; 8: 514-527. | ||
| In article | View Article PubMed | ||
| [31] | White J, et al. ASPEN / AND characteristics recommended for the identification and documentation of adult malnutrition. JAcad Nutr Diet. 2012; 11(5): 2012. | ||
| In article | |||
| [32] | Santana S. State of malnutrition in Cuban hospitals; a needed update. Nutr Hosp 2015; 31/5): 1900-1909. | ||
| In article | View Article | ||
| [33] | Perez CE, Ruiz VS. Desnutrición hospitalaria: prevalencia en el Hospital Juárez de México. Rev Hosp Jua Mex 2010; 774(4): 234-238. | ||
| In article | View Article | ||
| [34] | Baca MG, Peña CM. Prevalencia de sub-alimentación de pacientes con soporte enteral en el Centro Médico Lic. Adolfo López Mateos. Nutr Hosp. 2015; 31(4): 1597-1602. | ||
| In article | View Article | ||
| [35] | Loser C. Malnutrition in hospital: the clinical and economic implications. Dtsch Arztebl Int 2010; 107: 911-7. | ||
| In article | PubMed PubMed | ||
| [36] | Johansen N. Effect of nutritional support on clinical outcome in patients at nutritional risk. Clin Nutr 2004; 23: 539-50. | ||
| In article | View Article PubMed | ||







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}