Lactate dehydrogenase (LDH) is an unspecific marker predominantly for hemolysis, thrombotic, infectious, and malignant diseases. On rare occasions, it can also be idiosyncratically elevated. We present a case of a 30-year-old otherwise healthy female patient who is referred to outpatient internal medicine with a persistent LDH elevation for years. Extensive laboratory and radiological diagnostics are performed without any indications of disease. Macro-LDH is suspected, and serum immunocomplex precipitation with polyethylene glycol is performed. Laboratory results make the presence of macro-LDH likely. Therefore, it is suggested that macroenzymes be considered early in the diagnostic journeys of patients with elevated serum enzyme activities unsuitable to the corresponding clinical context to spare them unnecessary procedures and provide them with a diagnosis of this probable benign condition.
Lactate Dehydrogenase (LDH) serves as an unspecific marker of cell death in vitro 1, 2 and human disease in vivo 3. Serum LDH is commonly elevated in oncological patients 4, 5, in hemolysis and associated disease 6, 7, during infections and thrombosis 8 as well as in rheumatic conditions like rheumatoid arthritis 9. In rare cases, this enzyme forms a complex with another protein, primarily immunoglobin, resulting in macro-LDH and elevated enzyme activity in laboratory assays due to increased serum half-life 10.
We present the case of a young female patient who underwent extensive diagnostic evaluation for asymptomatic elevation of serum LDH.
A 30-year-old woman is referred to internal medicine by her general practitioner for evaluation of persistent elevation of LDH. Recent laboratory work shows an LDH concentration of 382 U/l (reference: 70-240 U/l). Complete blood count (CBC), liver function parameters, TSH (thyroid-stimulating hormone), and creatinine are unremarkable. The patient complains of no current or recent health problems. In further detail, she denies weight loss, fever (not continuous nor cyclical), night sweats, or staying abroad before detection of LDH elevation. She does not take any regular medications or drugs, has never had any medical condition, and is a mother of two healthy children. According to her, LDH enzyme activity has been elevated “for years”, but she has never undergone extensive diagnostics, which she now wishes to be performed. Physical examination, electrocardiogram, and abdominal sonography show no abnormal findings, except for asymptomatic cholecystolithiasis. Blood work is repeated by atraumatic venipuncture, without a tourniquet, using a large bore needle. The hemolysis parameters haptoglobin and bilirubin are within the normal range, the CBC including reticulocyte count is unremarkable. Direct and indirect Coombs tests are negative. Coagulation studies, infection serology, autoantibody studies, muscle parameters, serum electrophoresis, immunophenotyping, immunoglobulin concentrations, electrolyte concentrations (sodium, potassium, calcium, chloride), liver and renal parameters (including urine status) do not show abnormalities. LDH is elevated (511 U/l, reference range: 125 - 220 U/l) and folic acid is mildly reduced (6,8 nmol/l, reference range: 7,9 – 46,4) without evidence of macrocytic anemia, the blood sedimentation rate is 80 mm after one hour and 100 mm after two hours. Pneumological evaluation for sarcoidosis and latent tuberculosis, as well as a computed tomography scan of the thorax and abdomen, remain without significant findings. Table 1 shows an overview of the full patient evaluation. Folic acid 5 mg once a day for one month is prescribed for possible subclinical ineffective hematopoiesis. Elevation of serum enzyme activity is suspected in the context of macro-LDH.
PEG precipitation is performed using a modified method based on the procedure proposed by Davidson et al. 11. 25 w/v % polyethylene glycol 6000 (Merck Millipore, Article # 817007) is prepared in 0,9 % sterile sodium chloride solution (Fresenius Kabi, free-flex infusion bag). 2 ml of patient serum is carefully mixed with 2 ml of 25 % PEG and incubated for 5 minutes at room temperature (verum sample). For the control specimen, 2 ml of patient serum is mixed with 2 ml of a 0,9 % sterile NaCl solution and incubated for 5 minutes at room temperature, resulting in a dilution of 1:1. The control and verum samples are centrifuged in Vacuette tubes with serum separator gel (Greiner Bio-One, Article # 455071) at a relative centrifugal force (RCF) of 1 521 for 8 minutes (Hettich Rotofix 32 A). The supernatant is transferred to a new Vacuette tube and sent for laboratory analysis. A third tube containing naïve blood serves as a reference and for the determination of folic acid concentration. The PEG precipitation process is displayed in the following flowchart.
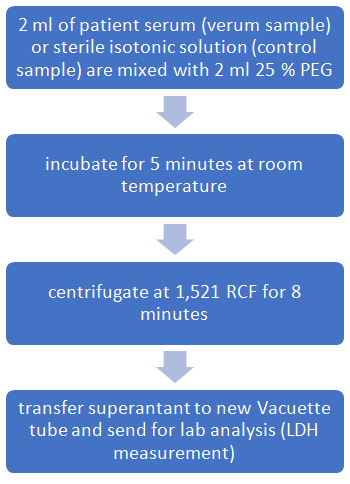
PEG is used due to its ability to precipitate immunoglobins and their corresponding complexes, largely sparing uncomplexed serum enzymes 12.
Bürki et al. and Dedeene et al. 13, 14 recently tried to establish reference values in healthy patients for PEG precipitation activities (PPA), a measurement for the serum enzyme activity after PEG precipitation. However, it should be noted that reference values vary significantly in the literature and appear to depend on analysis assays, lab machine used (Roche versus Abbott), precipitation protocol, and initial serum enzyme activity.
Laboratory results are shown in the following table. Cholesterol and immunoglobin G (IgG) concentrations were assessed as control markers for successful PEG precipitation.
Serum gamma globulins in the naïve sample were in the normal range, as increased serum globulins may generate false-positive results 15.
IgG was not detectable in the verum sample and cholesterol was reduced by 75 % comparing control and verum; therefore, success of the PEG precipitation reaction is likely. The folic acid concentration was now normal with still elevated LDH, excluding the hypothesis of subclinical ineffective hematopoiesis due to folic acid deficiency.
The PEG precipitation activity (PPA) can be calculated using the following equation, indicating how much LDH is not complexed to another protein and therefore does not precipitate during PEG exposure 11, 13:
 |
The reference values for the lower limits of LDH PPA vary in the literature ranging from 45 % (99. percentile upper limit of normal) to 65 % 13, 14. Davidson et al. 11 propose a 12 – 70 % reference spectrum for PPA in patients without macro-LDH.
The PPA in the patient sample is 73,6 % and therefore above the upper normal limits for PPA, suggesting the presence of macro-LDH.
LDH-isoenzyme electrophoresis is performed and confirms the presence of macro-LDH using a second test method for verification.
Macroenzymes develop when serum enzymes form complexes with serum proteins, especially immunoglobins. These complexes with higher molecular mass than uncomplexed enzymes lead to an elevated enzyme activity in laboratory assays due to increased serum half-life 10, 16.
As a result macroenzymes can lead to misinterpretation of laboratory values, prompting rigorous patient evaluation for a possible benign condition 17.
Historically macroenzymes have been described as causative factors for elevated serum enzyme activities of amylase 18 and successively for AST, lipase, CK, and LDH 10, 16. LDH macroenzymes were first found in lupoid liver cirrhosis and leukemia in 1967 19, 20. Cases of LDH elevation due to complex formation have also been described in patients with ulcerative colitis and myocarditis, in a post-burn patient, after interferon-alpha therapy for hepatitis C, after streptokinase therapy and after myocardial infarction. Hence they are usually associated with some kind of disease 19, 20, 21, 22, 23, 24, 25.
Nevertheless, there is also evidence, that macro-LDH formation is possible in totally healthy people: Perry et al. 8 presented a case of a healthy woman with a highly elevated serum LDH concentration of 4 457 U/l (normal range: 297 – 618 U/l), where LDH has formed a complex with immunoglobulin G to produce IgG-LDH. In 2011 Fillee et al. 26 described another case of a clinically healthy patient with an LDH concentration greater than two times the upper limit of normal, who had undergone splenectomy for assumed lymphomatous splenic lesions, only later to be diagnosed with LDH-macroenzyme condition presumably without clinical relevance.
Precipitation of macroenzyme complexes with polyethylene glycol 6000 and comparison of enzyme activity in the supernatant after centrifugation to an unprecipitated sample have been proposed as an easy-to-perform method in suspected cases of macroenzymes 11.
This method showed practical applicability and has already been used, for example, in a clinical case to prove the presence of AST-macroenzyme in a patient serum 27.
To our knowledge, this is the first case in which macro-LDH was suspected in a completely healthy young individual, and the PEG precipitation method was used first line in an outpatient setting for detection of an LDH enzyme complex.
In the case presented, extensive laboratory and radiological diagnostics had been performed before the possibility of macro-LDH was considered. After reviewing the literature, a procedure easy to perform in an outpatient setting and without laboratory equipment was found and performed, which demonstrated the existence of macro-LDH in the patient’s serum.
In general, macroenzyme conditions are characterized by persisting increased serum enzyme activities. It is therefore suggested that the possibility of macroenzyme existence should be considered early in patients in whom elevated serum enzyme values do not match the clinical context. As the prevalence of macroenzymes remains without an exact figure, it is unclear whether withholding or delaying extensive diagnostic testing for other conditions (possibly including radiation exposure and not insignificant cost for patients or health systems) in otherwise healthy patients is reasonable. Further research is necessary to establish validated PPA reference values to enable a broad adaption of the PEG precipitation method in the low-threshold detection of most likely benign macroenzyme conditions.
No funding was received for conducting this research.
Patrik Wintersberger: Ongoing employment with MSD Animal Health, reimbursement of expenses by Recordati.
Jürgen Harauer: Nothing to declare.
Informed consent from the patient for publication was obtained.
| [1] | Chan FKM, Moriwaki K, De Rosa MJ. Detection of Necrosis by Release of Lactate Dehydrogenase Activity. In: Snow AL, Lenardo MJ, editors. Immune Homeostasis [Internet]. Totowa, NJ: Humana Press; 2013 [cited 2023 Oct 29]. p. 65–70. (Methods in Molecular Biology; vol. 979). Available from: https://link.springer.com/10.1007/978-1-62703-290-2_7. | ||
| In article | View Article PubMed | ||
| [2] | Kumar P, Nagarajan A, Uchil PD. Analysis of Cell Viability by the Lactate Dehydrogenase Assay. Cold Spring Harb Protoc. 2018 Jun; 2018(6): pdb.prot095497. | ||
| In article | View Article PubMed | ||
| [3] | Wu Y, Lu C, Pan N, Zhang M, An Y, Xu M, et al. Serum lactate dehydrogenase activities as systems biomarkers for 48 types of human diseases. Sci Rep. 2021 Jun 21; 11(1): 12997. | ||
| In article | View Article PubMed | ||
| [4] | Forkasiewicz A, Dorociak M, Stach K, Szelachowski P, Tabola R, Augoff K. The usefulness of lactate dehydrogenase measurements in current oncological practice. Cell Mol Biol Lett. 2020 Dec; 25(1): 35. | ||
| In article | View Article PubMed | ||
| [5] | Jurisic V, Radenkovic S, Konjevic G. The Actual Role of LDH as Tumor Marker, Biochemical and Clinical Aspects. In: Scatena R, editor. Advances in Cancer Biomarkers [Internet]. Dordrecht: Springer Netherlands; 2015 [cited 2023 Oct 29]. p. 115–24. (Advances in Experimental Medicine and Biology; vol. 867). Available from: https://link.springer.com/10.1007/978-94-017-7215-0_8. | ||
| In article | View Article PubMed | ||
| [6] | Barcellini W, Fattizzo B. Clinical Applications of Hemolytic Markers in the Differential Diagnosis and Management of Hemolytic Anemia. Dis Markers. 2015; 2015: 1–7. | ||
| In article | View Article PubMed | ||
| [7] | Kato GJ, McGowan V, Machado RF, Little JA, Taylor J, Morris CR, et al. Lactate Dehydrogenase as a Biomarker of Hemolysis-Associated Nitric Oxide Resistance, Priapism, Leg Ulceration, Pulmonary Hypertension and Death in Patients with Sickle Cell Disease. Blood. 2005 Nov 16; 106(11): 3188–3188. | ||
| In article | View Article | ||
| [8] | Perry C, Peretz H, Ben-Tal O, Eldor A. Highly elevated lactate dehydrogenase level in a healthy individual: A case of macro-LDH. Am J Hematol. 1997 May; 55(1): 39–40. | ||
| In article | View Article | ||
| [9] | Cohen AS. Lactic dehydrogenase (LDH) and transaminase (GOT) activity of synovial fluid and serum in rheumatic disease states, with a note on synovial fluid LDH isozymes. Arthritis Rheum. 1964 Oct; 7(5): 490–501. | ||
| In article | View Article PubMed | ||
| [10] | Briani C, Zaninotto M, Forni M, Burra P. Macroenzymes: too often overlooked. J Hepatol. 2003 Jan; 38(1): 119. | ||
| In article | View Article PubMed | ||
| [11] | Davidson DF, Watson DJ. Macroenzyme detection by polyethylene glycol precipitation. Ann Clin Biochem Int J Lab Med. 2003 Sep 1; 40(5): 514–20. | ||
| In article | View Article PubMed | ||
| [12] | Fahie-Wilson M, Halsall D. Polyethylene glycol precipitation: proceed with care. Ann Clin Biochem Int J Lab Med. 2008 May; 45(3): 233–5. | ||
| In article | View Article PubMed | ||
| [13] | Bürki C, Volleberg M, Blomgren L, Froese S, Hersberger M. Reference ranges for the polyethylene glycol (PEG) precipitation activity (%PPA) of eight routine enzyme activities. Pract Lab Med. 2023 Jan; 33: e00304. | ||
| In article | View Article PubMed | ||
| [14] | Vermeersch P, Frans G, Dedeene L, Stockman M, Steels S. Detection of macroenzymes: establishing upper reference limits for eight enzymes after polyethylene glycol precipitation. Biochem Medica [Internet]. 2023 Feb 15 [cited 2023 Dec 8]; 33(1). Available from: https://www.biochemia-medica.com/en/journal/33/1/10.11613/BM.2023.010705. | ||
| In article | View Article PubMed | ||
| [15] | Ram S, Harris B, Fernando JJR, Gama R, Fahie-Wilson M. False-positive polyethylene glycol precipitation tests for macroprolactin due to increased serum globulins. Ann Clin Biochem Int J Lab Med. 2008 May; 45(3): 256–9. | ||
| In article | View Article PubMed | ||
| [16] | Galasso PJ, Litin SC, O’Brien JF. The Macroenzymes: A Clinical Review. Mayo Clin Proc. 1993 Apr; 68(4): 349–54. | ||
| In article | View Article PubMed | ||
| [17] | Turecky L. Macroenzymes and their clinical significande. Bratisl Lek Listy. 2005; 105(7-8): 260–3. | ||
| In article | |||
| [18] | Wilding P. Globulin-bound Amylase: A Cause of Persistently Elevated Levels in Serum. Ann Intern Med. 1964 Jun 1; 60(6): 1053. | ||
| In article | View Article | ||
| [19] | Ganrot PO. Lupoid cirrhosis with serum lactic acid dehydrogenase linked to an γA immunoglobulin. Experientia. 1967 Jul; 23(7): 593–593. | ||
| In article | View Article PubMed | ||
| [20] | Lundh B. A macromolecular serum lactate dehydrogenase activity in a case of leukemia. Clin Chim Acta. 1967 May; 16(2): 305–9. | ||
| In article | View Article PubMed | ||
| [21] | Delanghe J, De Buyzere M, De Scheerder I, Vanderborght J, Wieme R. Macro-lactate dehydrogenase in serum after acute myocardial infarction. Clin Chem. 1987 Jun 1; 33(6): 1103–4. | ||
| In article | View Article PubMed | ||
| [22] | Liu ZJ, Zhang Y. Macro Lactate Dehydrogenase in a Patient with Myocarditis. cclm. 2000 Apr 30; 38(4): 307–8. | ||
| In article | View Article PubMed | ||
| [23] | Liu ZJ, Zhang Y, Zhang XB, Yang X. Observation and identification of lactate dehydrogenase anomaly in a postburn patient. Postgrad Med J. 2004 Aug 5; 80(946): 481–3. | ||
| In article | View Article PubMed | ||
| [24] | Nabeshima S, Hayashi J, Hirata M, Nakashima K, Noguchi A, Kashiwagi S. Increased Lactic Dehydrogenase (LDH)-Linked Immunoglobulin Associated with Interferon-.ALPHA. Therapy in a Case of Chronic Hepatitis C. Intern Med. 1994; 33(7): 446–9. | ||
| In article | View Article PubMed | ||
| [25] | Pascarella F, Caropreso M, Miele E, Fortunato G, Vajro P, Staiano A. Macro-creatine kinase and macro-lactate dehydrogenase in a girl with ulcerative colitis. Dig Liver Dis. 2007 Aug; 39(8): 780–1. | ||
| In article | View Article PubMed | ||
| [26] | Fillee C, Van hoof V, Lambert M. INCREASE OF SERUM LACTATE DEHYDROGENASE CAUSED BY A MACROENZYME. A CASE REPORT. Acta Clin Belg. 2011 Feb 1; 66(1): 63–5. | ||
| In article | View Article PubMed | ||
| [27] | Rohani P, Imanzadeh F, Sayyari A, Kazemi Aghdam M, Shiari R. Persistent elevation of aspartate aminotransferase in a child after incomplete Kawasaki disease: a case report and literature review. BMC Pediatr. 2020 Dec; 20(1): 73. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2024 Patrik Wintersberger and Jürgen Harauer
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Chan FKM, Moriwaki K, De Rosa MJ. Detection of Necrosis by Release of Lactate Dehydrogenase Activity. In: Snow AL, Lenardo MJ, editors. Immune Homeostasis [Internet]. Totowa, NJ: Humana Press; 2013 [cited 2023 Oct 29]. p. 65–70. (Methods in Molecular Biology; vol. 979). Available from: https://link.springer.com/10.1007/978-1-62703-290-2_7. | ||
| In article | View Article PubMed | ||
| [2] | Kumar P, Nagarajan A, Uchil PD. Analysis of Cell Viability by the Lactate Dehydrogenase Assay. Cold Spring Harb Protoc. 2018 Jun; 2018(6): pdb.prot095497. | ||
| In article | View Article PubMed | ||
| [3] | Wu Y, Lu C, Pan N, Zhang M, An Y, Xu M, et al. Serum lactate dehydrogenase activities as systems biomarkers for 48 types of human diseases. Sci Rep. 2021 Jun 21; 11(1): 12997. | ||
| In article | View Article PubMed | ||
| [4] | Forkasiewicz A, Dorociak M, Stach K, Szelachowski P, Tabola R, Augoff K. The usefulness of lactate dehydrogenase measurements in current oncological practice. Cell Mol Biol Lett. 2020 Dec; 25(1): 35. | ||
| In article | View Article PubMed | ||
| [5] | Jurisic V, Radenkovic S, Konjevic G. The Actual Role of LDH as Tumor Marker, Biochemical and Clinical Aspects. In: Scatena R, editor. Advances in Cancer Biomarkers [Internet]. Dordrecht: Springer Netherlands; 2015 [cited 2023 Oct 29]. p. 115–24. (Advances in Experimental Medicine and Biology; vol. 867). Available from: https://link.springer.com/10.1007/978-94-017-7215-0_8. | ||
| In article | View Article PubMed | ||
| [6] | Barcellini W, Fattizzo B. Clinical Applications of Hemolytic Markers in the Differential Diagnosis and Management of Hemolytic Anemia. Dis Markers. 2015; 2015: 1–7. | ||
| In article | View Article PubMed | ||
| [7] | Kato GJ, McGowan V, Machado RF, Little JA, Taylor J, Morris CR, et al. Lactate Dehydrogenase as a Biomarker of Hemolysis-Associated Nitric Oxide Resistance, Priapism, Leg Ulceration, Pulmonary Hypertension and Death in Patients with Sickle Cell Disease. Blood. 2005 Nov 16; 106(11): 3188–3188. | ||
| In article | View Article | ||
| [8] | Perry C, Peretz H, Ben-Tal O, Eldor A. Highly elevated lactate dehydrogenase level in a healthy individual: A case of macro-LDH. Am J Hematol. 1997 May; 55(1): 39–40. | ||
| In article | View Article | ||
| [9] | Cohen AS. Lactic dehydrogenase (LDH) and transaminase (GOT) activity of synovial fluid and serum in rheumatic disease states, with a note on synovial fluid LDH isozymes. Arthritis Rheum. 1964 Oct; 7(5): 490–501. | ||
| In article | View Article PubMed | ||
| [10] | Briani C, Zaninotto M, Forni M, Burra P. Macroenzymes: too often overlooked. J Hepatol. 2003 Jan; 38(1): 119. | ||
| In article | View Article PubMed | ||
| [11] | Davidson DF, Watson DJ. Macroenzyme detection by polyethylene glycol precipitation. Ann Clin Biochem Int J Lab Med. 2003 Sep 1; 40(5): 514–20. | ||
| In article | View Article PubMed | ||
| [12] | Fahie-Wilson M, Halsall D. Polyethylene glycol precipitation: proceed with care. Ann Clin Biochem Int J Lab Med. 2008 May; 45(3): 233–5. | ||
| In article | View Article PubMed | ||
| [13] | Bürki C, Volleberg M, Blomgren L, Froese S, Hersberger M. Reference ranges for the polyethylene glycol (PEG) precipitation activity (%PPA) of eight routine enzyme activities. Pract Lab Med. 2023 Jan; 33: e00304. | ||
| In article | View Article PubMed | ||
| [14] | Vermeersch P, Frans G, Dedeene L, Stockman M, Steels S. Detection of macroenzymes: establishing upper reference limits for eight enzymes after polyethylene glycol precipitation. Biochem Medica [Internet]. 2023 Feb 15 [cited 2023 Dec 8]; 33(1). Available from: https://www.biochemia-medica.com/en/journal/33/1/10.11613/BM.2023.010705. | ||
| In article | View Article PubMed | ||
| [15] | Ram S, Harris B, Fernando JJR, Gama R, Fahie-Wilson M. False-positive polyethylene glycol precipitation tests for macroprolactin due to increased serum globulins. Ann Clin Biochem Int J Lab Med. 2008 May; 45(3): 256–9. | ||
| In article | View Article PubMed | ||
| [16] | Galasso PJ, Litin SC, O’Brien JF. The Macroenzymes: A Clinical Review. Mayo Clin Proc. 1993 Apr; 68(4): 349–54. | ||
| In article | View Article PubMed | ||
| [17] | Turecky L. Macroenzymes and their clinical significande. Bratisl Lek Listy. 2005; 105(7-8): 260–3. | ||
| In article | |||
| [18] | Wilding P. Globulin-bound Amylase: A Cause of Persistently Elevated Levels in Serum. Ann Intern Med. 1964 Jun 1; 60(6): 1053. | ||
| In article | View Article | ||
| [19] | Ganrot PO. Lupoid cirrhosis with serum lactic acid dehydrogenase linked to an γA immunoglobulin. Experientia. 1967 Jul; 23(7): 593–593. | ||
| In article | View Article PubMed | ||
| [20] | Lundh B. A macromolecular serum lactate dehydrogenase activity in a case of leukemia. Clin Chim Acta. 1967 May; 16(2): 305–9. | ||
| In article | View Article PubMed | ||
| [21] | Delanghe J, De Buyzere M, De Scheerder I, Vanderborght J, Wieme R. Macro-lactate dehydrogenase in serum after acute myocardial infarction. Clin Chem. 1987 Jun 1; 33(6): 1103–4. | ||
| In article | View Article PubMed | ||
| [22] | Liu ZJ, Zhang Y. Macro Lactate Dehydrogenase in a Patient with Myocarditis. cclm. 2000 Apr 30; 38(4): 307–8. | ||
| In article | View Article PubMed | ||
| [23] | Liu ZJ, Zhang Y, Zhang XB, Yang X. Observation and identification of lactate dehydrogenase anomaly in a postburn patient. Postgrad Med J. 2004 Aug 5; 80(946): 481–3. | ||
| In article | View Article PubMed | ||
| [24] | Nabeshima S, Hayashi J, Hirata M, Nakashima K, Noguchi A, Kashiwagi S. Increased Lactic Dehydrogenase (LDH)-Linked Immunoglobulin Associated with Interferon-.ALPHA. Therapy in a Case of Chronic Hepatitis C. Intern Med. 1994; 33(7): 446–9. | ||
| In article | View Article PubMed | ||
| [25] | Pascarella F, Caropreso M, Miele E, Fortunato G, Vajro P, Staiano A. Macro-creatine kinase and macro-lactate dehydrogenase in a girl with ulcerative colitis. Dig Liver Dis. 2007 Aug; 39(8): 780–1. | ||
| In article | View Article PubMed | ||
| [26] | Fillee C, Van hoof V, Lambert M. INCREASE OF SERUM LACTATE DEHYDROGENASE CAUSED BY A MACROENZYME. A CASE REPORT. Acta Clin Belg. 2011 Feb 1; 66(1): 63–5. | ||
| In article | View Article PubMed | ||
| [27] | Rohani P, Imanzadeh F, Sayyari A, Kazemi Aghdam M, Shiari R. Persistent elevation of aspartate aminotransferase in a child after incomplete Kawasaki disease: a case report and literature review. BMC Pediatr. 2020 Dec; 20(1): 73. | ||
| In article | View Article PubMed | ||





{kind=link}