Neurovascular disorders, such as strokes and aneurysms, present significant global health and economic challenges. Robotic systems in neurovascular interventions offer promising improvements in procedural precision, safety, and clinical outcomes; however, their high acquisition and operational costs require rigorous financial justification. This study developed a service line-focused cost-benefit model to evaluate the financial viability and strategic value of robotic-assisted neurovascular systems. Using a mixed-methods approach, the study integrated a five-year deterministic financial model with qualitative interviews involving clinicians, hospital administrators, and strategic planners. Data were derived from vendor pricing, peer-reviewed literature, hospital budget reports, and expert insights. The model incorporated capital, operational, and clinical parameters and included sensitivity analyses to assess key variables such as procedural volume, reimbursement rates, and complication-related savings. Results indicated a projected net benefit of $21.4 million over five years under baseline assumptions, with procedural volume being the most influential factor in financial outcomes. Break-even analysis revealed that a minimum of 150 procedures per year is required for viability. Qualitative findings emphasized non-financial advantages, including improved physician recruitment, institutional prestige, and tele-robotic capabilities. These findings offer hospital decision-makers a comprehensive framework for evaluating robotic investments in neurovascular care.
Neurovascular disorders such as ischemic strokes, intracranial aneurysms, and arteriovenous malformations represent a significant source of global morbidity and mortality 1. Stroke alone accounts for over 12 million cases globally each year and is the second leading cause of death worldwide 2. With aging populations and the rising prevalence of cardiovascular risk factors such as hypertension, diabetes, and obesity, the demand for advanced neurovascular care continues to escalate 3. These demographic trends place considerable clinical and financial strain on healthcare systems, challenging institutions to deliver efficient, high-quality care.
Neuro-interventional procedures have evolved considerably over the past two decades with the advancement of minimally invasive endovascular techniques 4. Mechanical thrombectomy for acute ischemic stroke, coiling and stenting for aneurysms, and embolization procedures for arteriovenous malformations have revolutionized care delivery, reducing the need for open surgery. Nevertheless, these procedures remain technically demanding, highly operator-dependent, and susceptible to variability based on physician experience 5. Navigation within fragile cerebral vasculature leaves little margin for error, as even minor deviations can result in catastrophic complications such as hemorrhage or infarction 6.
Furthermore, prolonged exposure to ionizing radiation remains a significant occupational hazard for interventionalists and their support teams 7. The physical toll of wearing heavy lead aprons for extended periods compounds the occupational risks 4. These factors underscore the urgent need for technologies that enhance procedural precision, standardize outcomes, and improve provider safety.
Robotic-assisted systems have emerged as a promising solution to address these challenges. Leveraging advanced electromechanical controls, robotics offer improved precision, stability, and reproducibility during complex neurovascular procedures 8. Remote operation capabilities allow interventionalists to control procedures outside the radiation field, reducing occupational exposure. Moreover, emerging telerobotic applications suggest the potential to extend specialized neurovascular expertise to underserved regions lacking on-site interventionalists 9.
Despite these clinical promises, the financial realities of adopting robotic systems remain complex. Capital costs often exceed several million dollars, while ongoing maintenance, training, and consumable expenses compound long-term financial commitments 10. From a hospital administrator's perspective, particularly at the service line level where technology adoption decisions are often made—evaluating high-stakes investments requires a nuanced understanding of direct and indirect financial implications.
Traditional cost-effectiveness analyses often focus on broad system-level evaluations or payer-centric perspectives 11. However, hospital service lines operate under unique financial pressures, balancing procedural volume, payer mix, regional competition, staffing, and long-term institutional strategy. Few studies have developed cost-benefit models targeting service line decision-makers in the neurovascular domain.
This study aims to fill this gap by developing a comprehensive cost-benefit model evaluating the financial viability of robotic-assisted neurovascular systems from a service line perspective. By modeling direct costs, clinical benefits, market dynamics, and operational considerations, we seek to provide hospital administrators with an actionable framework to inform investment decisions.
Healthcare organizations face immense pressure to justify high-cost technology acquisitions. Cost-effectiveness analyses (CEAs) and budget impact analyses (BIAs) have been widely used to evaluate surgical robotics, particularly in high-volume specialties like prostatectomy and hysterectomy 10. These studies demonstrate that while robotic platforms entail substantial upfront costs, long-term financial viability depends heavily on utilization rates, complication reduction, and institutional efficiency 8.
For neurovascular robotics, however, the economic literature remains sparse. 9 emphasize that direct procedural cost savings may emerge from reduced complications, shorter lengths of stay, and improved rehabilitation outcomes following robotic-assisted interventions. However, these indirect savings are difficult to quantify ex-ante and are often excluded from basic ROI models.
Furthermore, many existing CEAs adopt a payer-centric perspective, focusing on system-level cost savings rather than service line-level financial realities 11. From a hospital administrator's perspective, additional variables such as payer mix, referral patterns, and regional competition significantly influence ROI calculations 5. While early feasibility data supports the technical capabilities of robotic neurovascular systems, significant gaps remain. There is limited real-world data on long-term clinical outcomes specific to neurovascular robotics. Additionally, existing literature offers sparse service line-level financial models that reflect hospital operational realities. Furthermore, there has been an inadequate exploration of strategic non-financial benefits, such as market differentiation, provider recruitment, and the potential for telerobotic expansion. This study addresses these gaps by constructing a detailed service line-focused cost-benefit model incorporating financial and strategic factors relevant to hospital decision-makers.
2.1. Research Questions1.What are the direct and indirect financial implications of adopting robotic-assisted systems for neurovascular care from a service line perspective?
2.How do clinical outcomes and procedural volume interact to influence the financial viability of robotic neurovascular systems?
This study adopted a mixed-methods design, combining qualitative inquiry with quantitative financial modeling to evaluate the economic and strategic considerations associated with robotic neurovascular intervention systems. The qualitative component involved semi-structured interviews with key stakeholders directly engaged in clinical practice, financial management, and strategic planning within neurovascular service lines. Concurrently, a deterministic cost-benefit analysis model was developed to simulate financial outcomes over a five-year horizon, incorporating data derived from published literature, vendor reports, and hypothetical hospital budget scenarios. The integrated approach allowed for both contextual exploration of decision-making factors and rigorous projection of financial implications.
3.2. ParticipantsA purposive sampling strategy was employed to select ten subject matter experts representing both clinical and administrative domains relevant to neurovascular robotics. The participant cohort comprised three neurointerventional radiologists, two stroke neurologists, three hospital financial administrators, and two healthcare strategic planners. These individuals were affiliated with large academic medical centers and regional referral hospitals across diverse U.S. healthcare markets. Institutional affiliations and specific geographic identifiers were anonymized to protect confidentiality. The composition of the sample was designed to capture multi-dimensional perspectives on clinical efficacy, financial feasibility, and organizational strategy pertaining to robotic adoption.
3.3. Data Collection InstrumentsTwo primary data collection instruments were utilized. First, semi-structured interview guides were developed, focusing on four core domains: clinical performance and efficacy of robotic systems, financial perceptions including capital investment and return expectations, strategic organizational objectives, and perceived adoption barriers. Second, a structured financial modeling tool was created using Microsoft Excel to facilitate quantitative analysis. Model inputs were populated using data synthesized from peer-reviewed literature, industry reports (particularly vendor documentation related to the CorPath GRX neurovascular robotic system) 13, and hypothetical hospital procurement documents constructed to reflect standard tertiary care acquisition and operational costs.
3.4. ProcedureInterviews were conducted remotely via secure, HIPAA-compliant video conferencing platforms. Each interview lasted approximately 45 to 60 minutes, was audio-recorded with informed consent, and subsequently transcribed verbatim. The qualitative data were analyzed using thematic analysis facilitated by NVivo software 12, employing an inductive coding approach to identify recurrent themes across clinical, financial, and strategic domains. The financial model was developed in parallel, with input values triangulated from multiple data sources: vendor pricing brochures, existing cost-effectiveness studies (notably 9, 10, and constructed procurement scenarios reflective of prevailing U.S. tertiary healthcare practices. Model assumptions were validated through expert feedback to enhance ecological validity.
3.5. Financial Model StructureThe financial model applied a deterministic cost-benefit framework, calculating total costs, total benefits, and net benefit over a five-year period. The following equations structured the model:
• Total Cost (TC): TC = C_init + C_train + (T × (C_maint + N × C_oper))
• Total Benefit (TB): TB = T × (N × (R + B_clinical) + B_volume)
• Net Benefit (NB): NB = TB − TC
Baseline parameter values (See Table 1) were derived from literature, vendor data, and hypothetical procurement assumptions, as outlined below:
To evaluate model robustness under varying operational conditions, a comprehensive sensitivity analysis was performed. Key model parameters—including procedural volume (N), reimbursement rates (R), clinical savings (B_clinical), capital investment (C_init), and operating costs (C_oper)—were systematically varied by ±25%. This sensitivity range was chosen to reflect both conservative and optimistic adoption scenarios, thereby allowing assessment of financial performance across a plausible spectrum of real-world implementation conditions.
The financial model applied a deterministic cost-benefit framework, calculating total costs, total benefits, and net benefit over a five-year period. The following equations structured the model:
TC = C_init + C_train + T × (C_maint + N × C_oper)
Substituting the parameter values yielded:
TC = 2,500,000 + 100,000 + 5 × (150,000 + 300 × 1,000) = 4,850,000 USD.
The total benefits over the same period were calculated as:
TB = T × [N × (R + B_clinical) + B_volume]
which resulted in:
TB = 5 × [300 × (15,000 + 1,500) + 300,000] = 26,250,000 USD.
The resulting net financial benefit (NB) was:
NB = TB − TC = 26,250,000 − 4,850,000 = 21,400,000 USD.
Thus, under baseline conditions, the model projects a positive net financial gain of $21.4 million over a five-year implementation horizon.
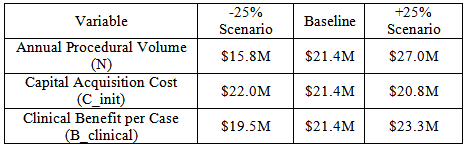
4.2. Sensitivity AnalysisSensitivity analyses were conducted to assess the impact of variation in key model parameters on projected financial outcomes (See Table 2). Three critical variables—annual procedural volume (N), capital acquisition cost (C_init), and clinical benefit per procedure (B_clinical)—were systematically varied by ±25% to simulate both conservative and optimistic adoption scenarios.
Annual procedural volume exhibited the highest sensitivity, with a $11.2 million spread in projected net benefit between the low and high utilization scenarios. Variations in capital cost and clinical benefit per procedure had relatively smaller effects on overall net benefit. This suggests that achieving and sustaining sufficient procedural volume is the primary financial determinant of successful adoption.
4.3. Break-Even ThresholdThe break-even threshold analysis identified that a minimum procedural volume of approximately 150 robot-assisted neurovascular interventions per year is required to achieve financial viability over the five-year evaluation period. Below this utilization threshold, cumulative costs exceed projected benefits unless supplemented by substantial strategic, reputational, or clinical advantages. Institutions unable to achieve this volume may need to consider broader strategic justifications—including research prominence, recruitment competitiveness, and future tele-robotic capabilities—to support investment decisions.
4.4. Thematic Analysis of Expert InterviewsQualitative thematic analysis of expert interviews yielded several recurring themes that complement the financial findings, offering additional context for adoption considerations.
Neurointerventional physicians consistently expressed optimism regarding the potential clinical advantages of robotic systems. Anticipated benefits included enhanced precision in navigating complex cerebral vasculature, improved stability of microcatheters during delicate maneuvers, and potential reductions in complication rates. Several participants also emphasized operator ergonomic benefits, particularly reduced physical strain and diminished cumulative radiation exposure during lengthy fluoroscopy-guided procedures.
From an administrative perspective, the adoption of neurovascular robotics was viewed as a strategic opportunity for market differentiation. Hospital executives and strategic planners cited potential advantages in marketing cutting-edge capabilities to attract referring physicians, patients, and highly specialized clinical staff. In several interviews, participants highlighted the emerging possibility of tele-robotic stroke interventions, which could enable high-volume centers to extend specialty care access into rural and underserved markets—a consideration aligned with broader institutional population health goals.
Financial administrators uniformly identified the magnitude of the initial capital acquisition cost as the most significant barrier to adoption. Competing capital priorities within constrained institutional budgets were frequently cited, along with uncertainty regarding whether sustained procedural volume could be reliably achieved to justify the initial investment. While downstream revenue projections appeared favorable in the model, participants emphasized that such projections would be scrutinized during internal budget justification processes.
Several participants highlighted operational barriers that may complicate implementation. These included steep learning curves for technical staff, requirements for dedicated training programs, early inefficiencies in procedural scheduling and room turnover, and ambiguity surrounding insurance reimbursement for robot-assisted neurovascular interventions. Participants emphasized that addressing these operational barriers proactively would be essential to support smooth clinical integration.
The financial analysis in this study demonstrates that robotic neurovascular intervention platforms hold the potential for strong economic viability when implemented under conditions of sufficient procedural demand and operational readiness. The projected net benefit of $21.4 million over a five-year evaluation period underscores that, when fully utilized, robotic systems can generate both significant direct procedural revenue and substantial downstream savings. Importantly, these financial benefits are not purely a function of capital investment, but rather reflect the dynamic interplay between volume, clinical outcomes, and strategic market positioning.
The dominant influence of procedural volume on financial returns aligns with well-established principles from broader robotic surgery literature 10. In neurovascular care specifically, where case complexity and precision are paramount, robotic systems may provide incremental safety and efficiency gains that compound financial performance. The model's sensitivity analysis clearly illustrates that while capital acquisition costs and clinical benefit assumptions are meaningful, sustained procedural throughput is the primary lever determining long-term financial success. Institutions capable of concentrating sufficient case volume—either through regional referral aggregation, tele-robotic expansion, or comprehensive service line integration—are therefore optimally positioned to realize the full economic potential of robotic neurovascular platforms.
Beyond financial projections, the qualitative data enriches interpretation by highlighting a convergence of clinical, operational, and strategic perspectives that extend the value proposition of robotic adoption. Physicians emphasized improved procedural control in navigating tortuous cerebral vasculature, where millimeter-level precision can critically influence outcomes in thrombectomy or aneurysm coiling procedures. These clinical refinements, while often challenging to quantify in purely economic terms, may yield meaningful reductions in peri-procedural complications, improved recanalization rates, and downstream recovery advantages that ultimately reduce hospital resource utilization and improve long-term patient quality of life.
Additionally, the interviews reveal how robotic neurovascular adoption may operate as a strategic growth catalyst. Administrators framed robotics as an opportunity to enhance institutional prestige, attract top-tier clinician talent, and potentially restructure regional referral networks through emerging tele-robotic capabilities. This strategic dimension introduces a multiplier effect: not only does robotics directly generate procedural revenue, but it may also drive organizational growth by capturing market share, strengthening payer negotiations, and positioning institutions at the forefront of neurovascular innovation.
Furthermore, the operational complexities identified by stakeholders reflect a realistic understanding of adoption challenges. Training demands, early learning curves, and scheduling inefficiencies are consistent with prior robotic adoption experiences in other specialties. However, these obstacles, while non-trivial, are typically front-loaded and tend to diminish as institutional expertise matures. Over time, as familiarity with robotic workflows increases and scheduling protocols adapt, the operational friction often stabilizes, allowing clinical and financial benefits to fully materialize.
Taken together, these findings suggest that while robotic neurovascular adoption requires careful planning, institutional commitment, and clear procedural volume strategies, the long-term return on investment can be substantial—both financially and strategically. The value proposition is not solely transactional but rather embedded within broader organizational trajectories that include clinical excellence, workforce development, and regional leadership in advanced cerebrovascular care.
The results of this study reinforce prior findings from broader surgical robotics literature, where high-volume centers are consistently shown to realize the greatest financial returns from robotic investments 8. This study contributes novel insights specific to neurovascular care by incorporating emerging strategic dimensions unique to this subspecialty. Notably, interview participants highlighted the distinct potential for tele-robotic expansion, allowing tertiary centers to remotely extend neurovascular intervention capabilities into rural or underserved markets. Early feasibility demonstrations of tele-robotic stroke interventions suggest this model could profoundly alter institutional referral patterns, allowing regional centers of excellence to capture larger catchment areas 15. This emerging capacity represents a potential multiplier effect on procedural volume, which may further reinforce the favorable economics demonstrated in the financial model.
Furthermore, while prior cost-effectiveness analyses have primarily focused on robotic applications in urology, gynecology, and general surgery, this study expands the conversation into a rapidly developing neurovascular domain where early technological feasibility has been demonstrated but economic assessments remain sparse. As neurovascular robotics matures, this study provides an initial framework for evaluating both the financial and strategic considerations that will shape adoption trajectories.
5.2. Strategic Non-Financial ImplicationsBeyond direct financial considerations, several strategic non-financial benefits emerged from expert interviews that may provide additional justification for institutional investment. First, advanced robotic capabilities may enhance recruitment of highly specialized neurointerventional physicians who seek access to cutting-edge technology platforms 6.The presence of robotic systems may also serve to reduce occupational injuries and physical strain associated with prolonged exposure to radiation and operator fatigue 4, potentially extending the career longevity of specialized physicians—a factor of increasing relevance as workforce shortages intensify in advanced interventional specialties.
Moreover, early adoption of robotic neurovascular capabilities may confer brand differentiation advantages in competitive healthcare markets, positioning institutions as leaders in advanced stroke and cerebrovascular care. Institutions establishing first-mover status in tele-robotic expansion may also gain early operational experience and technological integration expertise, potentially shaping future referral pathways and payer contracting opportunities as tele-robotic interventions mature.
Collectively, these non-financial considerations suggest that robotic adoption may offer strategic institutional value that extends beyond direct revenue projections, particularly for academic medical centers seeking leadership positioning in evolving neurovascular care models.
5.3. LimitationsSeveral limitations of this study warrant consideration. First, the financial model relied on hypothetical parameter estimates extrapolated from published literature, vendor reports, and constructed procurement scenarios due to the current scarcity of comprehensive real-world neurovascular robotics data. While parameter values were triangulated and validated through expert consultation, they remain subject to inherent uncertainty. Second, the financial model adopted a provider-institution perspective, excluding broader societal costs such as patient quality-adjusted life years (QALYs) or societal productivity gains, which may underestimate total value generation from improved neurovascular outcomes. Third, the rapid pace of technological evolution in robotic systems may alter capital cost structures and operational performance characteristics over time, potentially impacting future cost-benefit dynamics. Finally, the qualitative component of this study utilized a relatively small, purposive sample of experts, limiting the generalizability of thematic findings across broader institutional contexts.
5.4. Future Research DirectionsGiven these limitations and the emerging nature of robotic neurovascular systems, several important areas warrant further investigation. Longitudinal outcome studies following real-world neurovascular robotics programs are needed to validate clinical efficacy, complication reduction rates, and long-term cost savings. Comparative studies evaluating clinical and economic outcomes between centers adopting robotics versus those maintaining conventional manual interventions would provide valuable evidence to inform best-practice adoption models. As tele-robotic capabilities continue to develop, expanded feasibility trials testing remote intervention networks across geographically dispersed, rural healthcare systems are needed to assess clinical safety, logistical feasibility, and broader access-to-care implications. Finally, integration of value-based reimbursement models into financial assessments—accounting for both quality improvement and cost containment—may offer a more comprehensive framework for evaluating robotic neurovascular investments in evolving healthcare payment landscapes.
Robotic-assisted neurovascular systems represent a promising technological advancement capable of enhancing procedural precision, improving safety, and expanding access to complex interventions. From a service line perspective, this study demonstrates that while upfront capital and training costs are substantial, long-term financial returns can be significant when procedural volume is optimized and modest clinical improvements are realized.
Our model suggests breakeven thresholds are achievable even at moderate case volumes typical of regional referral centers. Furthermore, strategic advantages such as market differentiation, physician recruitment, and future tele-robotic capabilities strengthen the case for adoption beyond purely financial considerations.
Successful integration, however, requires deliberate preparation, including robust training programs, multidisciplinary team coordination, and continuous clinical governance. As robotic platforms mature and outcome data accumulate, ongoing evaluation will remain critical to ensuring that adoption decisions are both clinically sound and economically sustainable.
| [1] | World Health Organization, "World Stroke Day 2022," WHO Sri Lanka, Oct. 29, 2022. [Online]. Available: https:// www.who.int/ srilanka/news/detail/29-10-2022-world-stroke-day-2022. | ||
| In article | |||
| [2] | V. L. Feigin et al., "Global burden of stroke and risk factors in 204 countries and territories," Lancet Neurol., vol. 20, no. 10, pp. 795–820, 2021. | ||
| In article | |||
| [3] | J. F. Meschia et al., "Guidelines for the primary prevention of stroke: A statement for healthcare professionals from the American Heart Association/American Stroke Association," Stroke, vol. 45, no. 12, pp. 3754–3832, 2014. | ||
| In article | View Article PubMed | ||
| [4] | C. S. Weyland et al., "Occupational radiation exposure of neurointerventionalists during endovascular stroke treatment," Eur. J. Radiol., vol. 164, p. 110882, 2023. | ||
| In article | View Article PubMed | ||
| [5] | W. G. Kunz et al., "Cost-Effectiveness of Endovascular Stroke Therapy: A Patient Subgroup Analysis From a US Healthcare Perspective," Stroke, vol. 47, no. 11, pp. 2797–2804, 2016. | ||
| In article | View Article PubMed | ||
| [6] | J. D. Morrison et al., "Feasibility of robotic neuroendovascular surgery," Interv. Neuroradiol., vol. 30, no. 5, pp. 611–618, 2024. | ||
| In article | View Article PubMed | ||
| [7] | D. L. Miller et al., "Occupational radiation protection in interventional radiology: A joint guideline of the Cardiovascular and Interventional Radiology Society of Europe and the Society of Interventional Radiology," J. Vasc. Interv. Radiol., vol. 21, no. 5, pp. 607–615, 2010. | ||
| In article | View Article PubMed | ||
| [8] | K. H. Narsinh et al., "Robotics for neuroendovascular intervention: Background and primer," Neuroradiol. J., vol. 35, no. 1, pp. 25–35, 2022. | ||
| In article | View Article PubMed | ||
| [9] | H.-J. Mijderwijk et al., "External validation of the ARISE prediction models for aneurysmal rebleeding after aneurysmal subarachnoid hemorrhage," Neurosurgery, vol. 97, no. 1, pp. 120–129, 2025. | ||
| In article | View Article PubMed | ||
| [10] | H. M. Hollandsworth et al., "Multiquadrant surgery in the robotic era: A technical description and outcomes for da Vinci Xi robotic subtotal colectomy and total proctocolectomy," Surg. Endosc., vol. 34, pp. 5153–5159, 2020. | ||
| In article | View Article PubMed | ||
| [11] | D. B. Mark and M. A. Hlatky, "Medical economics and the assessment of value in cardiovascular medicine: Part I," Circulation, vol. 106, no. 4, pp. 516–520, 2002. | ||
| In article | View Article PubMed | ||
| [12] | NVivo, NVivo (Version 12) [Computer software], QSR International Pty Ltd., 2020. [Online]. Available: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home. | ||
| In article | |||
| [13] | Corindus, a Siemens Healthineers Company, "CorPath GRX neurovascular system demonstrates safety and effectiveness in robotic-assisted aneurysm embolization," Endovascular Today, Sep. 12, 2022. [Online]. Available: https:// evtoday.com/ news/ corindus-corpath-grx-neurovascular-system-demonstrates-safety-and-effectiveness-in-robotic-assisted-aneurysm-embolization. | ||
| In article | |||
| [14] | C. B. Beaman, N. Kaneko, P. M. Meyers, and S. Tateshima, "A Review of Robotic Interventional Neuroradiology," AJNR Am. J. Neuroradiol., vol. 42, no. 5, pp. 808–814, 2021. | ||
| In article | View Article PubMed | ||
| [15] | G. Charbonnier et al., "Telestroke network to robotic telestroke network: How to upgrade regional stroke care to include remote robotics?," Digit. Health, vol. 10, 2024. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2025 Oluwadamilola Adeleke
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | World Health Organization, "World Stroke Day 2022," WHO Sri Lanka, Oct. 29, 2022. [Online]. Available: https:// www.who.int/ srilanka/news/detail/29-10-2022-world-stroke-day-2022. | ||
| In article | |||
| [2] | V. L. Feigin et al., "Global burden of stroke and risk factors in 204 countries and territories," Lancet Neurol., vol. 20, no. 10, pp. 795–820, 2021. | ||
| In article | |||
| [3] | J. F. Meschia et al., "Guidelines for the primary prevention of stroke: A statement for healthcare professionals from the American Heart Association/American Stroke Association," Stroke, vol. 45, no. 12, pp. 3754–3832, 2014. | ||
| In article | View Article PubMed | ||
| [4] | C. S. Weyland et al., "Occupational radiation exposure of neurointerventionalists during endovascular stroke treatment," Eur. J. Radiol., vol. 164, p. 110882, 2023. | ||
| In article | View Article PubMed | ||
| [5] | W. G. Kunz et al., "Cost-Effectiveness of Endovascular Stroke Therapy: A Patient Subgroup Analysis From a US Healthcare Perspective," Stroke, vol. 47, no. 11, pp. 2797–2804, 2016. | ||
| In article | View Article PubMed | ||
| [6] | J. D. Morrison et al., "Feasibility of robotic neuroendovascular surgery," Interv. Neuroradiol., vol. 30, no. 5, pp. 611–618, 2024. | ||
| In article | View Article PubMed | ||
| [7] | D. L. Miller et al., "Occupational radiation protection in interventional radiology: A joint guideline of the Cardiovascular and Interventional Radiology Society of Europe and the Society of Interventional Radiology," J. Vasc. Interv. Radiol., vol. 21, no. 5, pp. 607–615, 2010. | ||
| In article | View Article PubMed | ||
| [8] | K. H. Narsinh et al., "Robotics for neuroendovascular intervention: Background and primer," Neuroradiol. J., vol. 35, no. 1, pp. 25–35, 2022. | ||
| In article | View Article PubMed | ||
| [9] | H.-J. Mijderwijk et al., "External validation of the ARISE prediction models for aneurysmal rebleeding after aneurysmal subarachnoid hemorrhage," Neurosurgery, vol. 97, no. 1, pp. 120–129, 2025. | ||
| In article | View Article PubMed | ||
| [10] | H. M. Hollandsworth et al., "Multiquadrant surgery in the robotic era: A technical description and outcomes for da Vinci Xi robotic subtotal colectomy and total proctocolectomy," Surg. Endosc., vol. 34, pp. 5153–5159, 2020. | ||
| In article | View Article PubMed | ||
| [11] | D. B. Mark and M. A. Hlatky, "Medical economics and the assessment of value in cardiovascular medicine: Part I," Circulation, vol. 106, no. 4, pp. 516–520, 2002. | ||
| In article | View Article PubMed | ||
| [12] | NVivo, NVivo (Version 12) [Computer software], QSR International Pty Ltd., 2020. [Online]. Available: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home. | ||
| In article | |||
| [13] | Corindus, a Siemens Healthineers Company, "CorPath GRX neurovascular system demonstrates safety and effectiveness in robotic-assisted aneurysm embolization," Endovascular Today, Sep. 12, 2022. [Online]. Available: https:// evtoday.com/ news/ corindus-corpath-grx-neurovascular-system-demonstrates-safety-and-effectiveness-in-robotic-assisted-aneurysm-embolization. | ||
| In article | |||
| [14] | C. B. Beaman, N. Kaneko, P. M. Meyers, and S. Tateshima, "A Review of Robotic Interventional Neuroradiology," AJNR Am. J. Neuroradiol., vol. 42, no. 5, pp. 808–814, 2021. | ||
| In article | View Article PubMed | ||
| [15] | G. Charbonnier et al., "Telestroke network to robotic telestroke network: How to upgrade regional stroke care to include remote robotics?," Digit. Health, vol. 10, 2024. | ||
| In article | View Article PubMed | ||