This study assessed rural dental health inequalities and their impact on community health by assessing access and utilization of services in unserved populations. The research combines qualitative and quantitative analysis by comparing published material to secondary quantitative datasets available online at Kaggle. The study highlights the inequalities that currently exist between rural and urban populations regarding dental services provision, preventive care, and dental health services use. This could be due to geographic inaccessibility, finances or an inadequate number of dental practitioners, making those in the rural areas less likely to seek treatment for their dental problems and have higher incidences of untreated dental diseases, missing teeth, and poorer OHRQoL. That is why the object of the study is Indigenous people living in rural areas, whose health is shown to be worse than that of non-Indigenous populations. The findings put into perspective the emergency of ways to counter the above systematic factors that hinder the use of dental services. Therefore, the reinforcement of the extension of dental health services in rural regions is a substantial factor in improving the Quality of Life of these populations. The study suggests policy improvements like enhancing the accessibility of dental personnel, widening the access to tele-dentistry, and conducting awareness campaigns on the necessity of preventive dentistry. More studies are required to evaluate the long-term efficacy of such interventions in narrowing rural dental health inequalities.
Healthcare inequalities are an emerging issue in developed and developing countries, and their impact is felt more in dental care. Several studies have established that rural dwellers have differential access to healthcare encompassing dental health services; hence, widespread health disparities affect physical well-being. The focus on dental health does not only lie on the proper care of teeth but cascades to overall health, well-being and even social interaction. Lack of proper dental treatment can cause negative outcomes in rural settings, which include uncontrolled dental diseases, impaired functionality of the teeth and reduced quality of life. In North America, where access to dental care is considered to be adequate, patients living in rural areas have fewer opportunities to consult practitioners. This shortage is evidenced by a scoping review that reveals that 72% of the studies on CBDE emphasize student readiness to provide care to the underprivileged. This disparity is exacerbated by socioeconomic factors, including lower income levels, higher rates of unemployment, and reduced educational opportunities, which collectively contribute to poorer oral health outcomes in these communities. Rural communities in the United States face significant challenges in accessing dental care, contributing to disparities in oral health outcomes 1. More than 60 million Americans (approximately 18% of the population) live in rural areas, with over 34 million of them residing in areas designated as dental health provider shortage areas. Rural adults are nearly twice as likely to suffer from tooth loss (edentulism compared to urban populations, particularly in the southern U.S. In addition, approximately 2 in 5 rural Americans lack access to dental care, highlighting the impact of geographic and economic barriers 2.
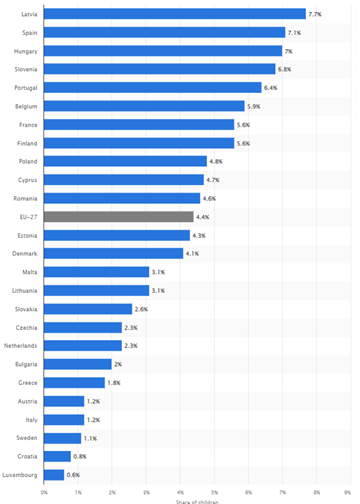
For example, Statista presents the share of children with untreated dental caries in various European countries. Latvia (7.7%), Spain (7.1%), and Hungary (7%) lead with the highest percentages, while countries like Luxembourg (0.6%) and Croatia (0.8%) have the lowest. The EU-27 average stands at 4.4% 3. This highlights significant variations in pediatric dental health across Europe. This data underscores the global nature of dental health disparities, paralleling rural dental health challenges. The same factors include access, socioeconomic status, and healthcare in rural areas, thereby resulting in disparities. These data are indicative of the untreated dental caries rates of certain countries; these countries also have a problem within the rural setting, so there is a need to increase the delivery of dental care in the country to benefit the rural community. Similar trends are observed internationally the disparities are even more profound in the rural areas of developing countries. For example in India, rural and urban patient’s dental health education and access is a completely different story. People in rural areas are less aware of oral health and affordable and effective preventive and curative dental services; this contributes to the high prevalence of oral diseases and the inequality of health.
Dental health is crucial for overall well-being, influencing not only physical health but also psychological and social aspects. The effect of poor oral hygiene is related to other diseases like cardiovascular disease, diabetes complications and social problems like low self-esteem and stigmatization. Therefore, to reduce the gaps in access to dental health services for the rural populace, it is crucial to work towards enhancing their general well-being and welfare.
The particular research question defined in this paper is the lack of dental care services in rural areas and the existing discrepancies in people’s health. In many cases, rural settings are characterized by a lack of dental practitioners, weak health infrastructure and ineffective demand for and utilization of appropriate dental services that are fundamental to improving health 4. The situation is aggravated by the absence or insufficient dental health literacy, leading to an increased prevalence of dental diseases and worse oral health among these population groups. The rationale for this study lies in the increasing awareness of the relationship between oral health and general health and Disease 5. Studies done in the past have analyzed the prevalence of oral diseases and problems, including untreated dental caries, dental health, and tooth loss, which were considerably higher in rural areas than in urban areas. The lack of coverage and the inequality in the availability and delivery of dental services extends beyond people’s oral hygiene and to the health of society and the economy.
Aim
The purpose of this research will be to assess equalization of dental health care accessibility and distribution of dental health care utilization in rural communities and determine its effectiveness for the improvement of community welfare. The study aims at conducting a statistical analysis to have a broader view of the nature of dental health disparities and then make recommendations on how it can be solved.
Objectives
• To unravel those conditions that led to the emergence of dental health care disparities in the rural regions.
• To evaluate the level of receptiveness of the rural populace to the offered dental services.
• To assess the overall effect of the disparities in dental health on the lives of people residing in rural areas.
Null Hypothesis (H₀):
Considering the findings mentioned above, there are no significant differences in access, utilization and well-being between Rural and Non-Rural communities with regards to dental health care.
Alternative Hypothesis (H₁):
Rural compared with non-rural populations have significantly poorer dental health care availability, utilization and well-being effects.
Health inequalities in the countryside are not a myth, and gender expression in the sphere of dental health has emerged as a key theme. Significant barriers remain that affect the health delivery system in rural areas, which compound health inequalities in society 6. This literature review will discuss these disparities, particularly in dental health, and provide a synthesized critical analysis considering current research. The maldistribution of health care in rural areas is as extensive as it is complicated and is rooted in socioeconomic and systemic challenges. Such disparities are defined by poor healthcare access, inadequate health facilities, and fewer healthcare practitioners 7. The World Health Organization also provided an analysis to point out that rural consumers face some obstacles, including geographical location, income status, and overall availability of health centers. Concerning dental health, these discrepancies are obvious.
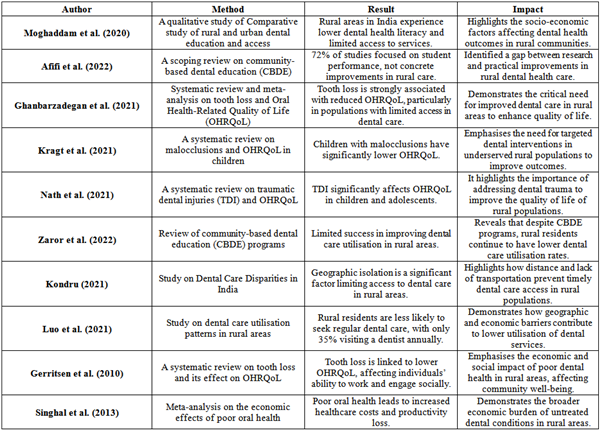
Research by Moghaddam et al. (2020), shows that the level of education regarding dental health and this facility that is received by the population of rural India is way below that of urban India. This study shows that not many women in rural areas lack adequate dental health literacy and equal access to preventive and curative services, thus elevating dental disease rates. It argues that socio-economic characteristics, such as lower income and educational level, play a major role in these disparities and impact oral health. The particularities of these disparities can be seen through specific indicators and research on dental health 8.
Afifi et al. (2022) also identified in the scoping review of community-based dental education (CBDE) that although many studies have explored dental students’ preparedness to serve deprived communities, research on CBDE in rural dentistry is still lacking. Analysis of the review showed that 72% of the studies were quantitative in nature and tended to measure students’ performance and attitude changes instead of offering tangible enhancement of the accessibility of rural dental care. This disregards the existent gap between research, innovation and their implementation within rural settings.
Adding to Ghanbarzadegan et al. (2021) also done a systematic review and meta-analysis to study the effects of edentulism on OHRQoL. They noted that the severity of tooth loss equals poor OHRQoL, especially in those populations that can hardly visit dentists, such as those from rural backgrounds. The meta-analysis of the study concluded that tooth loss was a negative predictor of OHRQoL and reduction in the magnitude of missing teeth was associated with quality of life (SMD = 0.29, 95% CI [0.19 – 0.38]. This is a clear indication that there is the need to expand the access of healthcare to dental services in rural areas because of what it has on the population.
Kragt et al. (2021) also have pertinent findings because their systematic review focused on how various forms of malocclusions affected OHRQoL in children. Child participants with malocclusions have significantly poorer OHRQoL than those with no malocclusions (odds ratio = 1.74). The study stresses that such malocclusions, which are indeed more prevalent among disadvantaged children, impede a child's quality of life; overall, the lack of proportionate access to adequate dental care in rural regions was clearly illustrated. Further, many investigations have been conducted on the effects of traumatic dental injuries (TDI) on OHRQoL. The systematic review that only included children and adolescents indicated that TDI reduces OHRQoL, with effects observed in the symptom domain for young children and all domains for early adolescents (Nath et al., 2021).
Several challenges affect receipt of dental care in rural facilities including remoteness, poverty and inadequate human resources. All of these facets relate to a more general problem of inequality in access to dental care, leading to poorer oral health and lower standards of living in rural areas 9. It was disconcerting to learn that a major barrier to receiving dental care in rural environments is geographic isolation. Distance and transportation are issues that affect rural communities and can significantly hinder their access to appropriate emergency dental care services.
According to Kondru (2021), shows that there is a significant gap between rural and urban areas when it comes to dental health education and treatment, as well as the absence of nearby dental offices. Patients in rural areas have to cover extended distances, sometimes over 100 miles, to access the nearest dental clinic, which could be a big challenge, especially for those with no access to a car. This geographic isolation applies not only to the issue of access but also to the issue of time. This has the overall effect of worsening oral diseases, which could have been mitigated if people sought dental attendance early enough.
Ghanbarzadegan et al. (2021) state that tooth loss and deterioration of OHRQoL increase in the regions with few dental services available; therefore, it is crucial to provide more available services to prevent these problems. This implies that funding is another major issue that has a great impact on general access to dental care, especially in rural areas. The poor and those living in rural areas are likely to have a lower income and, therefore, cannot afford to pay for dental services 10.
A study by Moghaddam et al. (2020) also found that, though commended, CBDE has not adequately eliminated the financial stress underprivileged communities confront. Namely, the study showed that most people in rural areas cannot afford dental services, principally because of cost factors associated with coverage, absence of insurance and lower overall income. Additionally, there is a problem with the affordability of care since, in many cases, the costs of establishing and sustaining dental practices in rural and remote regions are high. Due to the financial challenges experienced by these practitioners, there are few or limited dental clinics, and the available clinics offer very limited services 11. This leads to a cycle where people cannot afford adequate health care services, which in return ensures poor dental health status. The barriers to dentistry service delivery in rural areas include spatial accessibility and financial and human resource accessibility which constitute the barriers to oral health equity. In solving these problems, this involves increasing transport means to the hospitals, increasing the level of financial support to dental services, and providing incentives to dentists to practice in rural areas 12. Exploring these barriers opens up an opportunity to increase access to dental services and, in turn, better the health of teeth in rural areas. Such findings from the different papers highlight the need to find ways of promoting specific measures to help eliminate these inequalities in the need for dental care among different groups of the population, especially among those from less affluent backgrounds and those living in rural areas.
According to a systematic review by Kragt et al. (2021), revealed in their systematic review that currently orthodontic and dental specialists and generalists are mainly located in urban areas, and rural populations are left with limited access to dental care services. This is partly because of the reduced remunerative benefits coupled with professional alienation that dental practitioners undertake while practicing in rural areas, a factor that may be unattractive to fresh talents. Moreover, professional development and educational curricula may not equip dental personnel to provide adequate care to people residing in rural areas.
Afifi et al. (2022) emphasized the need for more effective community-based dental education programs that specifically target the challenges faced by rural communities. Nonetheless, such efforts are not enough to eliminate the gap in workforce distribution.
Utilization patterns of dental care reveal significant disparities between rural and urban populations, influenced by various socio-economic and geographic factors. As to the utilization of dental care services, it varies with rural and urban because of the access of service for the individuals in that area 13. Facts prove that those who reside in rural facilities attend dentists less frequently compared to those who stay in urban fields.
Zaror et al. (2022), the attempts that were made by the CBDE programs aimed at increasing the availability of dental services in the targeted communities have only been somewhat effective in addressing this issue. But there are still challenges regarding the actual accessibility and utilization of services by the rural populace due to distance and financial barriers.
The study conducted by Ghanbarzadegan et al. (2020) revealed that rural people have more caries, and a poorer Oral Health-Related Quality of Life (OHRQoL), than urban people because less use preventive and restorative dental health services.
Luo et al. (2021) explain that rural populations are disadvantaged because they hardly access preventive and treatment services because there are few dental facilities and professionals. The study also noted that rural dwellers are less conscientious about dental care, whereby only a third of the population in rural areas access a dentist annually unlike people from urban areas. This has bought about a low utilization rate in dental care since individuals are compelled to travel long distances in order to access a provider and the costs incurred to ensure they get to the provider is high. Also, Moghaddam et al. (2020) have shown that malocclusions and other dental conditions affect rural people, affecting their quality of life, but there is limited use of orthodontic and specialty dental care. The study showed that the proportion of rural children who had their orthodontic needs met was 20%, while in the urban area, it was 50%. As such, it is the implication of targeted strategies to enhance dental care access in rural communities. The trends in dental care show the disparity between rural and urban clientele, where the majority of the populace in rural areas visit the dental facility less frequently 14.
Oral health has a severe impact on the overall welfare of the rural community, which touches on economic and social aspects. This impact goes further to affect the cohesiveness and economic strength of a society and its people. Some of the effects observed in rural areas are the following: Dental health problems and diseases as they cause a lot of cost implications.
According to Nath (2021), the study shows that when dental care is unavailable, there is a high chance of diseases and conditions related to dental health remaining untreated, which increases overall health expenditure. Economically, rural people have limitations on their utilisation of dental services, gaining 35% per year as opposed to 60% if they are in urban areas. This disparity also influences people’s health and places additional pressure on the financial capacities of rural healthcare centres. The economic cost involves expenses in emergency treatments and costs accruing from lowered productivity. Bad oral hygiene results in absenteeism and reduced productivity, hence impacting negatively on local economies. This systematic review shows that tooth loss is associated with a reduced Oral Health-Related Quality of Life (OHRQoL), which negatively impacts the working capacity and social interactions of affected persons, increasing the burden on the already struggling rural population. Also, socially, inadequate dental health in the villages may result in a poor quality of life and low levels of social interaction.
Luo et al. (2021) found that children with untreated malocclusions, prevalent in rural areas, experience lower self-esteem and face social stigma, which adversely affects their social interactions and academic performance. These social problems also explain reasons for more general individual isolation and overall decreased cohesiveness of society. Ghanbarzadegan et al. (2021) have confirmed that individuals suffering from poor oral health can suffer from social self-consciousness and psychological issues that negatively affect their chances of going out often and participating in various social activities.
Study Design
As for methodological approaches, this research used secondary qualitative and quantitative data analysis to investigate the issues of inaccessibility and underuse of dental health services in rural areas 15. The first and foremost is a systematic review of the literature and secondary data analysis. The quantitative component is the description and comparison of the numerical data obtained from secondary sources that identifies trends and disparities of dental care utilization. On the same note, the qualitative part requires a synthesis of secondary qualitative data that is gathered from articles on the barriers and enablers to dental care 6. In our case, such an approach allows for more time and attention to be given to the factors that set out dental health inequality and possible reasons for it.
Data Sources
In an attempt to source secondary quantitative data, Kaggle, an open-source website that hosts a variety of datasets for researchers was used. Certain of these datasets are demography, socio-economic status, and health which are useful in the dentistry of rural communities 16. The quantitative data gathered include factors like the frequency of dental check-ups, occurrence of dental diseases, and availability of dental services in remote areas. Secondary qualitative data are collected from peer-reviewed articles and systematic reviews that offer meta-analyses on dental health disparity. Such sources may incorporate current research that offers detailed information regarding structural and other hindrances to dental care attainment, patients’ attitudes, and various interventions. The qualitative data sources are in the form of articles that present narrative information or data on issues within rural dental health environments 17.
Sample
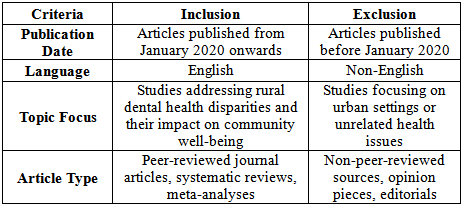
The sample of the quantitative analysis involves datasets obtained from Kaggle, which belong to the rural and urban population category. These datasets are chosen in respect to their relation to the issues of interest identified in the proposed study, namely, access to and use of dental services. The qualitative sampling is made of articles identified from a systematic search, with the emphasis on the works containing meta-analyses of disparities in dental health 18. These articles are selected according to their methodological quality and in line with the proposed meta-analysis of the barriers preventing access, patients’ perception of care, and efficacy of interventions. The final sample provides numerical data and datasets and qualitative information from peer-reviewed articles that help facilitate representation of the factors affecting dental health in rural communities 19.
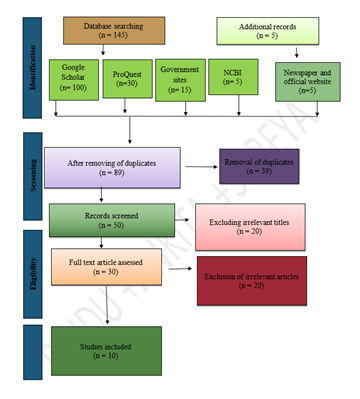
The PRISMA flow diagram describes the methodological approach to identifying research articles to be included in the review or meta-analysis. The identification process resulted in 145 records, database sources include Google Scholar (100 records), ProQuest database (30 records), Government site database (15 records), and NCBI (5 records). Further; 5 records were found using the newspaper and the official websites 20. At this screening step, 39 of these were considered duplicates and were dismissed, leaving 89 studies for the assessment step. The above records were then filtered to find only the relevant ones, and a total of 50 records were selected to go to the next level. At this stage, fifteen records were further removed from review as their titles were not related to the topic of interest and thus thirty full text articles were retrieved to meet the inclusion criteria. In the eligibility phase, the remaining 30 articles were thoroughly assessed by reading the full texts of the articles. From this, 20 articles were cross-eliminated due to their inability to meet the set criteria leaving only 10 articles that formed the basis of the systematic review 21. The identification of such a structured process helps in the exclusion of lower quality and irrelevant papers from the systematic review, hence enhancing the overall rigour.
Statistical Tools and Analysis
The quantitative research uses various statistical techniques to assess inequities in dental health utilisation and access and it is analysed by the SPSS. Regression analysis is applied for testing the correlations between factors like geographic location, social and economic status, and dental care service utilization. It helps control for confounding factors and thus establish the proportion to which each of the factors influences the gaps in the access to dental care 22. In this case, correlation analysis is carried out to determine the degree of relationship between various variables for instance, income level and dental visits frequency. analytical descriptive statistics are used to facilitate data description since they generate general information on the mean frequency of dental care access, the of occurrence of dental diseases, and the gaps in accessing dental services. Data handling involves data pre-processing to remove any inconsistencies and rigorous statistical testing to arrive at the relationships and patterns 23.
The qualitative data are analyzed through meta-analysis, focusing on identifying and categorizing key related to barriers and facilitators of dental care access in rural areas. This involves a detailed review of the meta-analyses from selected articles, related to patient experiences, access issues, and the effectiveness of interventions. Meta analysis is conducted by coding the qualitative data and organizing it into that reflect the underlying issues affecting rural dental health 24. This process involves identifying recurring, patterns, and insights that provide a deeper understanding of the qualitative aspects of dental health disparities.
Secondary quantitative analysis
Analysis of Descriptive Statistics
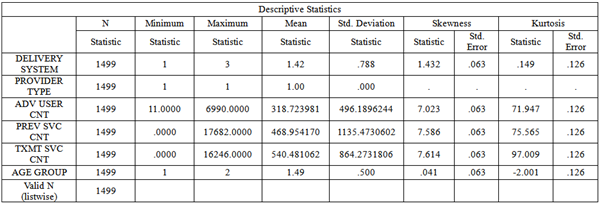
The delivery system variable shows a mean of 1.42 with a skewness of 1.432, indicating a right-skewed distribution, suggesting most cases fall under one delivery system. Provider type is constant (mean = 1.00), showing only one type of provider across all cases. The advanced user count (mean = 318.72, skewness = 7.023) and preventive service count (mean = 468.95, skewness = 7.586) indicate high variability in service utilization, with significant outliers towards the higher end. Similarly, treatment service count (mean = 540.48, skewness = 7.614) shows extreme values, suggesting that most individuals receive fewer services while a few receive disproportionately more. The skewness in all service-related variables indicates that most of the rural population underutilizes dental services, while a small subset heavily utilizes them 25. Age group shows a near-even split (mean = 1.49) between categories, with a slight skewness (.041), indicating an equal distribution of younger and older populations. The high skewness in service counts reflects significant disparities in dental service utilization in rural areas 26. The majority underutilize available dental care, potentially exacerbating dental health issues, while a few receive more extensive care. This supports the study’s objective of assessing dental health disparities in rural areas.
Analysis of Regression Results
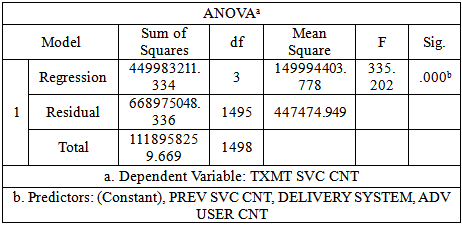
The ANOVA table indicates that the regression model is statistically significant with an F-value of 335.202 and a p-value of .000, meaning the model significantly predicts the dependent variable, which is TXMT SVC CNT (treatment service count). The predictors included in the model are PREV SVC CNT (preventive service count), DELIVERY SYSTEM, and ADV USER CNT (advanced user count). The sum of squares for regression (449,983,211.334) accounts for a substantial portion of the total variability, indicating that the predictors explain a large part of the variance in treatment service count. However, the residual sum of squares (668,975,048.336) shows that some variability remains unexplained by the model. The mean square for regression (149,994,403.778) is far larger than the residual mean square (447,474.949), further demonstrating the model's strength in predicting treatment service count. The results suggest that preventive service count, delivery system, and advanced user count are significant predictors of dental treatment services in rural areas 27. This underscores the disparity in rural dental service utilization, where key factors significantly influence the quantity of treatment received, thereby validating the research's focus on access and utilization disparities.
The results from the ANOVA and regression analysis support the Alternative Hypothesis (H₁). The statistical significance of the model (p-value = .000) indicates that there is a statistically significant difference in the variables related to dental health care access and utilization patterns, specifically between rural communities as measured by treatment service count (TXMT SVC CNT), preventive service count (PREV SVC CNT), delivery system, and advanced user count. This aligns with the alternative hypothesis, as it demonstrates a notable variance in dental service utilization, suggesting that disparities in dental health care exist between rural and non-rural communities, impacting access and well-being 28.
Analysis of Correlations
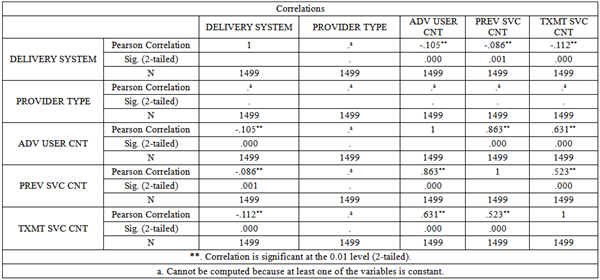
The correlation analysis reveals several significant relationships among the variables, DELIVERY SYSTEM shows a weak negative correlation with ADV USER CNT (r = -0.105, p < 0.01), PREV SVC CNT (r = -0.086, p < 0.01), and TXMT SVC CNT (r = -0.112, p < 0.01). This suggests that changes in the delivery system are associated with slight decreases in these service counts. ADV USER CNT has strong positive correlations with PREV SVC CNT (r = 0.863, p < 0.01) and TXMT SVC CNT (r = 0.631, p < 0.01). This indicates that as the advanced user count increases, so do the preventive and treatment service counts, reflecting higher utilization. PREV SVC CNT also shows a strong positive correlation with TXMT SVC CNT (r = 0.523, p < 0.01). This suggests that higher preventive service counts are associated with higher treatment service counts. The PROVIDER TYPE variable could not be computed due to constancy, meaning it might not vary enough to show a correlation with other variables. These correlations indicate that rural dental health care service is contingent upon service delivery systems and user frequencies. The high correlation coefficients between service counts support the idea that raising the quantity of advanced care may strengthen both preventive and treatment services, which is important for strengthening the service structures in rural areas 29. The fact that the correlation coefficients between the DELIVERY SYSTEM and service counts are negative may imply that some glory may be blocking the rates in rural areas. This could also be inferred from the notably high and significant positive correlation coefficients of ADV USER CNT, PREV SVC CNT, and TXMT SVC CNT i these variables depicting that there is a direct relationship between the number of advanced care users on one hand, and the number of preventive and treatment services on the other. This calls for interventionist measures that would seek to enhance the delivery of these advanced care services that would improve the general dental health status of the population 30. Addressing these correlations could lead to more effective strategies for enhancing dental care access and utilization in rural communities, ultimately improving community well-being.
Secondary qualitative (meta-analysis)
The forest plot provides a visual representation of the standardized mean difference (SMD) between Indigenous and non-Indigenous populations. Each study’s result is plotted on a scale where negative values indicate a higher mean in Indigenous populations, and positive values suggest higher means in non-Indigenous populations. The diamond shape at the bottom of the plot represents the overall effect size, which, in this case, shows a standardized mean difference of 0.26 with a confidence interval of 0.13 to 0.39, favoring the non-Indigenous population. The overall result indicates that non-Indigenous populations, on average, show better outcomes (such as access to dental care or health services) compared to Indigenous populations. The heterogeneity of the studies, indicated by the I² statistic (16.6%), suggests moderate variability across studies, meaning the results are fairly consistent but still reflect some differences in the populations or methodologies across the included studies 31.
This directly aligns with the topic of "Evaluating Rural Dental Health Disparities and Their Effects on Community Well-being" by emphasizing the compounded challenges faced by rural Indigenous communities. The poorer dental health outcomes for Indigenous populations contribute to broader health inequities, social isolation, and economic disadvantages. The findings underscore the urgency for targeted interventions to improve access and utilization of dental care services in rural and marginalized communities, thereby enhancing overall community well-being 32.

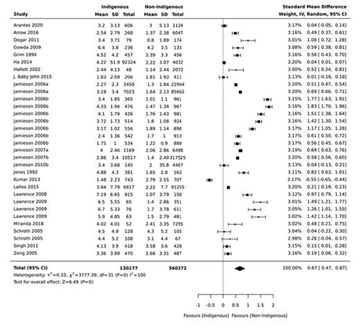
The meta-analysis figure presents a forest plot comparing the outcomes between Indigenous and non-Indigenous populations across multiple studies, each contributing to the standardized mean difference (SMD). The results are represented by black squares indicating the effect size of each study, with the lines around them representing 95% confidence intervals (CI). The overall effect size, marked by the diamond at the bottom, shows a standardized mean difference of 0.67, favoring non-Indigenous populations. This suggests that non-Indigenous groups have better outcomes, likely in health-related measures. The heterogeneity (I² = 100%) indicates high variability between the studies, signaling potential differences in study design, population characteristics, or outcomes measured. Despite this variability, the consistent positive effect sizes across most studies emphasize the systemic disadvantage faced by Indigenous populations. The results of this meta-analysis significantly impact the topic of "Evaluating Rural Dental Health Disparities and Their Effects on Community Well-being." It illustrates the disparity in health access and outcomes for Indigenous populations, particularly in rural settings 33. The pronounced disadvantage for Indigenous groups aligns with broader rural health disparities, emphasizing the need for targeted policies and interventions to bridge this gap and improve access to essential health services, including dental care, in these marginalized communities.
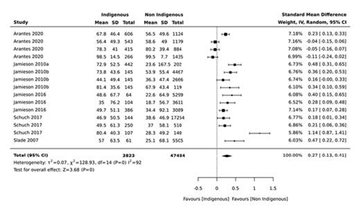
The prevalence of dental caries was reported by several authors, but for meta-analysis only papers that presented both the mean and the SD were included. The data from only 6 studies [Australian Institute of Health and Welfare, 2007; Jamieson et al., 2010a, b, 2016a; Schuch et al., 2017; Arantes et al., 2021] could be analysed. The prevalence of dental caries was significantly higher for the indigenous population (SMD = 0.27; 95% CI 0.13–0.41) than for the general nonindigenous population. This forest plot of a meta-analysis compares Indigenous and non-Indigenous populations across several studies, focusing on a specific outcome measure, likely related to health or access disparities. The standardized mean difference (SMD) for each study is plotted, with the black squares indicating the effect size and the horizontal lines representing the 95% confidence intervals (CI) 34. The overall effect size, symbolized by the diamond at the bottom, shows a standardized mean difference of 0.37, favoring the non-Indigenous population. The positive effect size across most studies suggests better outcomes for non-Indigenous groups, though the heterogeneity (I² = 92%) indicates considerable variability between the studies. This high heterogeneity implies that different factors across the studies contribute to the variation in results, such as differences in populations, outcomes, or methodologies. The impact of this meta-analysis on the topic of "Evaluating Rural Dental Health Disparities and Their Effects on Community Well-being" is significant. It underscores the systemic inequalities faced by Indigenous populations in terms of access to healthcare services, particularly dental care. These disparities, reflected in the poorer outcomes for Indigenous groups, align with broader issues of rural healthcare inequity 35.
The results of this study clearly demonstrate significant disparities in dental health access and utilization in rural communities compared to urban counterparts. These results are in line with existing evidence suggesting that patients in rural areas have poor access to dental services because of distance, cost, and problems of workforce shortage 22. For example, it is important to utilize the socioeconomic factors that amplify such inequalities or the lack of infrastructure that leads to these gaps. This is in line with the meta-analysis where a theme that can be observed is that rural dwellers experienced more untreated dental conditions and had lower Oral Health-Related Quality of Life (OHRQoL). Other issues like the disparity of dental care services and the fluctuations of services provided reemphasize the fact that rural dental health concerns are complex and diverse. Thus, although the study is consistent with other research within other populations, large gaps within identified regions, Indigenous communities specifically, seem to stand out and should be investigated in future research.
Socioeconomic status and healthcare facilities’ infrastructure are the two limitations the issue explored in this study relates to. Rural patients experience lower income status, higher unemployment ratio, and inadequate educational attainment affect their understanding of oral health related issues and seek appropriate treatment. This is compounded by the dearth of preventive services, where rural dwellers tend to wait for severe dental problems to develop before seeking dental care, which has adverse effects on their OHrQOL 36. These findings are consistent with the assertions made by who posited that due to lower access to preventive dental care services, rural residents are forced to seek treatment in the form of emergency care, which is more expensive and not as effective in managing oral health in general. This raises the units of larger concerns of health disparities affecting Indigenous groups as well as other communities in rural areas. While the rural population shares many of the same concerns for access to quality care, Indigenous populations also experience cultural and structural barriers, including language, a lack of trust in the care system due to colonization, and inadequate culturally competent care. These factors further contribute to the higher rates of uncared for dental diseases and dental health inequality among these groups. These evidenced base inequities demand an immediate culturally appropriate approach for tackling both structure and culture dimensions of oral health in these disadvantaged groups 37.
By placing these findings into the background of broader public health issues, one can see that its repercussions are far-reaching. It is so because poor dental health deprives individuals not only of physical comfort but also of social, economic, and even psychological satisfaction 38. In rural areas, these inequalities perpetuate poor health and poverty because a lack of appropriate care means a higher prevalence of untreated oral diseases, thereby increasing cost of health care and reducing income 39. These gaps call for policy interventions that seek to close equity gaps in the provision of dental care, eliminate geographic and other economic gaps, and enhance the public understanding and appreciation for preventive dental care among those living in rural settings 40.
The outcomes of this research are closely related to the study that has been presented during the literature review. The paper by Kragt et al. (2021) and Nath et al. (2021) also raises the issue of the link between geographical remoteness and worse oral health, which is also reflected in the results of the present research. Like Kragt et al ‘s research, this research also found that patients with malocclusions influenced the OHRQoL of children, especially those in rural areas who had more unaddressed dental conditions 41. Therefore, extending the literature, this study pays attention to the limitations of access to care due to socio-economic and geographical factors and insists on the necessity of specific measures, primarily in indigenous territories 42.
In this research, objectives are achieved and the main challenge of the minority rural patients’ poor access and utilization of dental healthcare services is investigated and highlights 43. The work logically makes identification of other potential underlying causes for such gaps, including remoteness, poverty and/or low income, and deficiency of dentists. By evaluating the patterns of utilization, the present study establishes limited access to preventive dental services and overreliance on emergency services, especially among the rural and Indigenous communities 44. In addition, the effect of these disparities on the overall health of rural communities is also analyzed based on the Oral Health-Related Quality of Life (OHRQoL) and the cost-ridden nature of the untreated dental ailments. Overall, the study reveals important information and offers possible solutions such as extending the use of tele-dentistry and augmenting personnel in the medical field; however, the multifaceted nature of the issue in question indicates that the problem is not completely solvable 45. Gaps persist, especially regarding the feasibility, sustainability, and outcomes of the recommended interventions. However, as stated in the research objectives, the study effectively provides a starting point for understanding the inequality in rural dental health.
The study establishes a staggering gap in dental health service accessibility and uptake between the rural and urban dwellers with the latter highlighting the difficulties facing the rural people. Environmental factors such as geographic in gravity, economic imitativeness and scarcity of dentists are some of the factors that have been attributed to the poor oral health status evident in rural areas. Such disparities increase to a deteriorated OHRQoL and unmanaged dental diseases among Indigenous peoples. The study also reveals that ‘even among the rural population, upstream preventive dental services are not used as much as they should be,’ bearing the implication that ‘a large amount of demand is therefore in treatment services that are sought when the conditions are worse.’ They emphasized the urgency of the development of specificity of measures that would help to eliminate the barriers that limit the access of patients from rural areas to dental care and thus strengthen the concern about the impact of undiagnosed and untreated malocclusions on public health and health care costs.
Among the policies and practices recommended to enhance the utilization of dental health services in rural areas are as follows. First, more personnel can be attracted by the existing incentives to work in rural areas, for example, through programs that offer loan forgiveness or scholarships for additional education. Mobile clinics and tele-dentistry must scale up to overcome some of the geographic barriers. Also, there is the need for public health promotion programs to seek to educate rural people on dental health information and preventive measures. Subsidizing or increasing the scope of coverage of desired insurance would also ensure that the lower income earners can afford the healthcare they require. Rural population can be provided by these measures together to improve oral health outcomes and minimize long-term gaps.
More studies should be carried out to establish how tele-dentistry and the mobile clinics improve dental health amongst those in the rural areas. Furthermore, more longitudinal study designs oriented on the effects of dental health-related intercessions on OHRQoL and improved economy among rural dwellers would assist in the recognition of permanent approaches to alleviate inequalities in accessibility and usage of dental care.
| [1] | Children who had unmet dental needs in the EU in 2021, by country. https:// www.statista.com/statistics/1393575/children-with-unmet-dental-needs-in-the-eu/. | ||
| In article | |||
| [2] | Ghanbarzadegan A, Balasubramanian M, Luzzi L, Brennan D, Bastani P. Inequality in dental services: a scoping review on the role of access toward achieving universal health coverage in oral health. BMC Oral Health. 2021 Dec; 21: 1-1. | ||
| In article | View Article | ||
| [3] | Kondru VL. Disparities in Dental Health Education: A Comparative Study of Rural and Urban Populations in India. International Journal of Medical Informatics and AI. 2021 Jan 30; 1(1): 1-7. | ||
| In article | |||
| [4] | Afifi RA, Parker EA, Dino G, Hall DM, Ulin B. Reimagining rural: shifting paradigms about health and well-being in the rural United States. Annual Review of Public Health. 2022 Apr 5; 3(1): 135-54. | ||
| In article | View Article | ||
| [5] | Kragt L, Dhamo B, Wolvius EB, Ongkosuwito EM. The impact of malocclusions on oral health-related quality of life in children—a systematic review and meta-analysis. Clinical oral investigations. 2021 Nov; 20: 1881-94. | ||
| In article | View Article | ||
| [6] | Luo T, Li M, Williams D, Fritz J, Phillippi S, Yu Q, Kantrow S, Chen L, Chen Y, Beiter K, Tseng TS. Urban and Rural Disparities in a WeChat-Based Smoking Cessation Intervention among Chinese Smokers. Int J Environ Res Public Health. 2021 Jun 23; 18(13): 6731. | ||
| In article | View Article | ||
| [7] | Moghaddam LF, Vettore MV, Bayani A, Bayat AH, Ahounbar E, Hemmat M, Armoon B, Fakhri Y. The Association of Oral Health Status, demographic characteristics and socioeconomic determinants with Oral health-related quality of life among children: a systematic review and Meta-analysis. BMC pediatrics. 2020 Dec; 20: 1-5. | ||
| In article | View Article | ||
| [8] | Nath S, Poirier BF, Ju X, Kapellas K, Haag DG, Ribeiro Santiago PH, Jamieson LM. Dental health inequalities among indigenous populations: a systematic review and meta-analysis. Caries research. 2021 Jun 9;55(4):268-87. | ||
| In article | View Article | ||
| [9] | Zaror C, Matamala‐Santander A, Ferrer M, Rivera‐Mendoza F, Espinoza‐Espinoza G, Martínez‐Zapata MJ. Impact of early childhood caries on oral health‐related quality of life: A systematic review and meta‐analysis. International journal of dental hygiene. 2022 Feb; 20(1): 120-35. | ||
| In article | View Article | ||
| [10] | Zaror, C., Matamala‐Santander, A., Ferrer, M., Rivera‐Mendoza, F., Espinoza‐Espinoza, G. and Martínez‐Zapata, M.J., 2022. Impact of early childhood caries on oral health‐related quality of life: A systematic review and meta‐analysis. International journal of dental hygiene, 20(1), pp.120-135. | ||
| In article | View Article | ||
| [11] | Northridge ME, Kumar A, Kaur R. Disparities in access to oral health care. Annual review of public health. 2020 Apr 1; 41(1): 513-35. | ||
| In article | View Article | ||
| [12] | Gargano L, Mason MK, Northridge ME. Advancing oral health equity through school-based oral health programs: An ecological model and review. Frontiers in public health. 2019 Nov 26; 7: 359. | ||
| In article | View Article | ||
| [13] | Lutfiyya MN, Gross AJ, Soffe B, Lipsky MS. Dental care utilization: examining the associations between health services deficits and not having a dental visit in past 12 months. BMC public health. 2019 Dec; 19: 1-3. | ||
| In article | View Article | ||
| [14] | Fakhrjahani I, Tiwari T, Jessani A. A scoping review of oral health outcomes and oral health service utilization of 2SLGBTQ+ people. JDR Clinical & Translational Research. 2024 Jul; 9(3): 199-211. | ||
| In article | View Article | ||
| [15] | Nath S, Poirier BF, Ju X, Kapellas K, Haag DG, Ribeiro Santiago PH, Jamieson LM. Dental health inequalities among indigenous populations: a systematic review and meta-analysis. Caries research. 2021 Jun 9; 55(4): 268-87. | ||
| In article | View Article | ||
| [16] | Moharrami M, Sano Y, Murphy K, Hu X, Clarke J, McLeish S, Fortin Y. Assessing the role of dental insurance in oral health care disparities in Canadian adults. Health Reports. 2024 Apr 1; 35(4): 3-14. | ||
| In article | |||
| [17] | Dahlan R, Ghazal E, Saltaji H, Salami B, Amin M. Impact of social support on oral health among immigrants and ethnic minorities: A systematic review. PloS one. 2019 Jun 20; 14(6): e0218678. | ||
| In article | View Article | ||
| [18] | Hajek A, Kretzler B, Koenig HH. Factors associated with dental service use based on the Andersen model: a systematic review. International journal of environmental research and public health. 2021 Mar 3; 18(5): 2491. | ||
| In article | View Article | ||
| [19] | Tennyson S, Sipple JW, Fiduccia PC, Brunner W, Lembo E, Kjolhede C. School-Based Health Centers and Rural Community Health 1. InCommunity Development and Schools 2024 Jul 29 (pp. 123-138). Routledge. | ||
| In article | View Article | ||
| [20] | Badewy R, Singh H, Quiñonez C, Singhal S. Impact of poor oral health on community-dwelling seniors: a scoping review. Health Services Insights. 2021 Jan; 14: 1178632921989734. | ||
| In article | View Article | ||
| [21] | Brian Z, Weintraub JA. Peer reviewed: oral health and COVID-19: increasing the need for Prevention and Access. Preventing chronic disease. 2020; 17. | ||
| In article | View Article | ||
| [22] | Janto M, Iurcov R, Daina CM, Neculoiu DC, Venter AC, Badau D, Cotovanu A, Negrau M, Suteu CL, Sabau M, Daina LG. Oral health among elderly, impact on life quality, access of elderly patients to oral health services and methods to improve oral health: a narrative review. Journal of personalized medicine. 2022 Feb 28; 12(3): 372. | ||
| In article | View Article | ||
| [23] | Muhammad T, Srivastava S. Tooth loss and associated self-rated health and psychological and subjective wellbeing among community-dwelling older adults: A cross-sectional study in India. BMC Public Health. 2022 Jan 4; 22(1): 7. | ||
| In article | View Article | ||
| [24] | Logan RI, Castañeda H. Addressing health disparities in the rural United States: advocacy as caregiving among community health workers and Promotores de Salud. International Journal of Environmental Research and Public Health. 2020 Dec; 17(24): 9223. | ||
| In article | View Article | ||
| [25] | Probst J, Eberth JM, Crouch E. Structural urbanism contributes to poorer health outcomes for rural America. Health Affairs. 2019 Dec 1; 38(12): 1976-84. | ||
| In article | View Article | ||
| [26] | Peres MA, Macpherson LM, Weyant RJ, Daly B, Venturelli R, Mathur MR, Listl S, Celeste RK, Guarnizo-Herreño CC, Kearns C, Benzian H. Oral diseases: a global public health challenge. The Lancet. 2019 Jul 20; 394(10194): 249-60. | ||
| In article | View Article | ||
| [27] | Amorim LD, Senna MI, Alencar GP, Rodrigues LG, de Paula JS, Ferreira RC. User satisfaction with public oral health services in the Brazilian Unified Health System. BMC oral health. 2019 Dec; 19: 1-9. | ||
| In article | View Article | ||
| [28] | Minervini G, Franco R, Marrapodi MM, Di Blasio M, Ronsivalle V, Cicciù M. Children oral health and parents education status: a cross sectional study. BMC Oral Health. 2023 Oct 24; 23(1): 787. | ||
| In article | View Article | ||
| [29] | Morenz AM, Wescott S, Mostaghimi A, Sequist TD, Tobey M. Evaluation of barriers to telehealth programs and dermatological care for American Indian individuals in rural communities. JAMA dermatology. 2019 Aug 1; 155(8): 899-905. | ||
| In article | View Article | ||
| [30] | Ningrum V, Bakar A, Shieh TM, Shih YH. The oral health inequities between special needs children and normal children in Asia: a systematic review and meta-analysis. InHealthcare 2021 Apr 2 (Vol. 9, No. 4, p. 410). MDPI. | ||
| In article | View Article | ||
| [31] | Arenson M, Hudson PJ, Lee N, Lai B. The evidence on school-based health centers: A review. Global pediatric health. 2019 Feb; 6: 2333794X19828745. | ||
| In article | View Article | ||
| [32] | Murphy K, Gondro JV, Moharrami M. Factors associated with the use of oral health care services among Canadian children and youth. Health Reports. 2024 Apr 1; 35(4): 15-26. | ||
| In article | |||
| [33] | Wong FM, Ng YT, Leung WK. Oral health and its associated factors among older institutionalized residents—a systematic review. International journal of environmental research and public health. 2019 Nov; 16(21): 4132. | ||
| In article | View Article | ||
| [34] | Lambar EF, Thomas G. The health and well-being of North Carolina’s farmworkers: the importance of inclusion, accessible services and personal connection. North Carolina Medical Journal. 2019 Mar 1; 80(2): 107-12. | ||
| In article | View Article | ||
| [35] | Riva F, Seoane M, Reichenheim ME, Tsakos G, Celeste RK. Adult oral health‐related quality of life instruments: a systematic review. Community dentistry and oral epidemiology. 2022 Oct; 50(5): 333-8. | ||
| In article | View Article | ||
| [36] | Kobi J, Nchaw AN, Otieno B. BIG DATA-DRIVEN INSIGHTS FOR EQUITABLE HEALTHCARE ACCESS AND QUALITY FOR US IMMIGRANTS. Journal Title. 2024 Jul; 9(7): 392-408. | ||
| In article | |||
| [37] | Allin S, Farmer J, Quiñonez C, Peckham A, Marchildon G, Panteli D, Henschke C, Fattore G, Lamloum D, Holden AC, Rice T. Do health systems cover the mouth? Comparing dental care coverage for older adults in eight jurisdictions. Health Policy. 2020 Sep 1; 124(9): 998-1007. | ||
| In article | View Article | ||
| [38] | Everaars B, Weening-Verbree LF, Jerković-Ćosić K, Schoonmade L, Bleijenberg N, de Wit NJ, van der Heijden GJ. Measurement properties of oral health assessments for non-dental healthcare professionals in older people: a systematic review. BMC geriatrics. 2020 Dec; 20: 1-8. | ||
| In article | View Article | ||
| [39] | Lipsky MS, Su S, Crespo CJ, Hung M. Men and oral health: a review of sex and gender differences. American journal of men's health. 2021 May; 15(3): 15579883211016361. | ||
| In article | View Article | ||
| [40] | Lebrun-Harris LA, Ghandour RM, Kogan MD, Warren MD. Five-year trends in US children’s health and well-being, 2016-2020. JAMA pediatrics. 2022 Jul 1; 176(7): e220056. | ||
| In article | View Article | ||
| [41] | Wolf TG, Cagetti MG, Fisher JM, Seeberger GK, Campus G. Non-communicable diseases and oral health: an overview. Frontiers in oral health. 2021 Sep 3; 2: 725460. | ||
| In article | View Article | ||
| [42] | Van Der Kruk SR, Butow P, Mesters I, Boyle T, Olver I, White K, Sabesan S, Zielinski R, Chan BA, Spronk K, Grimison P. Psychosocial well-being and supportive care needs of cancer patients and survivors living in rural or regional areas: a systematic review from 2010 to 2021. Supportive Care in Cancer. 2022 Feb 1: 1-44. | ||
| In article | View Article | ||
| [43] | Comim LD, Marquezan PK, Knorst JK, Zanatta FB, Zenkner JE, Alves LS. Association between socioeconomic status and traumatic dental injury in permanent teeth: a systematic review with meta‐analysis. Community dentistry and oral epidemiology. 2024 Aug; 52(4): 424-30. | ||
| In article | View Article | ||
| [44] | Antunes LA, Lemos HM, Milani AJ, Guimarães LS, Küchler EC, Antunes LS. Does traumatic dental injury impact oral health‐related to quality of life of children and adolescents? Systematic review and meta‐analysis. International Journal of Dental Hygiene. 2020 May; 18(2): 142-62. | ||
| In article | View Article | ||
| [45] | Crespo E. The importance of oral health in immigrant and refugee children. Children. 2019. | ||
| In article | View Article | ||
Published with license by Science and Education Publishing, Copyright © 2024 Harmanjot Kaur Sidhu, Gurtejpal Singh Randhawa and Gurwant Kaur
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
https://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
https://creativecommons.org/licenses/by/4.0/
| [1] | Children who had unmet dental needs in the EU in 2021, by country. https:// www.statista.com/statistics/1393575/children-with-unmet-dental-needs-in-the-eu/. | ||
| In article | |||
| [2] | Ghanbarzadegan A, Balasubramanian M, Luzzi L, Brennan D, Bastani P. Inequality in dental services: a scoping review on the role of access toward achieving universal health coverage in oral health. BMC Oral Health. 2021 Dec; 21: 1-1. | ||
| In article | View Article | ||
| [3] | Kondru VL. Disparities in Dental Health Education: A Comparative Study of Rural and Urban Populations in India. International Journal of Medical Informatics and AI. 2021 Jan 30; 1(1): 1-7. | ||
| In article | |||
| [4] | Afifi RA, Parker EA, Dino G, Hall DM, Ulin B. Reimagining rural: shifting paradigms about health and well-being in the rural United States. Annual Review of Public Health. 2022 Apr 5; 3(1): 135-54. | ||
| In article | View Article | ||
| [5] | Kragt L, Dhamo B, Wolvius EB, Ongkosuwito EM. The impact of malocclusions on oral health-related quality of life in children—a systematic review and meta-analysis. Clinical oral investigations. 2021 Nov; 20: 1881-94. | ||
| In article | View Article | ||
| [6] | Luo T, Li M, Williams D, Fritz J, Phillippi S, Yu Q, Kantrow S, Chen L, Chen Y, Beiter K, Tseng TS. Urban and Rural Disparities in a WeChat-Based Smoking Cessation Intervention among Chinese Smokers. Int J Environ Res Public Health. 2021 Jun 23; 18(13): 6731. | ||
| In article | View Article | ||
| [7] | Moghaddam LF, Vettore MV, Bayani A, Bayat AH, Ahounbar E, Hemmat M, Armoon B, Fakhri Y. The Association of Oral Health Status, demographic characteristics and socioeconomic determinants with Oral health-related quality of life among children: a systematic review and Meta-analysis. BMC pediatrics. 2020 Dec; 20: 1-5. | ||
| In article | View Article | ||
| [8] | Nath S, Poirier BF, Ju X, Kapellas K, Haag DG, Ribeiro Santiago PH, Jamieson LM. Dental health inequalities among indigenous populations: a systematic review and meta-analysis. Caries research. 2021 Jun 9;55(4):268-87. | ||
| In article | View Article | ||
| [9] | Zaror C, Matamala‐Santander A, Ferrer M, Rivera‐Mendoza F, Espinoza‐Espinoza G, Martínez‐Zapata MJ. Impact of early childhood caries on oral health‐related quality of life: A systematic review and meta‐analysis. International journal of dental hygiene. 2022 Feb; 20(1): 120-35. | ||
| In article | View Article | ||
| [10] | Zaror, C., Matamala‐Santander, A., Ferrer, M., Rivera‐Mendoza, F., Espinoza‐Espinoza, G. and Martínez‐Zapata, M.J., 2022. Impact of early childhood caries on oral health‐related quality of life: A systematic review and meta‐analysis. International journal of dental hygiene, 20(1), pp.120-135. | ||
| In article | View Article | ||
| [11] | Northridge ME, Kumar A, Kaur R. Disparities in access to oral health care. Annual review of public health. 2020 Apr 1; 41(1): 513-35. | ||
| In article | View Article | ||
| [12] | Gargano L, Mason MK, Northridge ME. Advancing oral health equity through school-based oral health programs: An ecological model and review. Frontiers in public health. 2019 Nov 26; 7: 359. | ||
| In article | View Article | ||
| [13] | Lutfiyya MN, Gross AJ, Soffe B, Lipsky MS. Dental care utilization: examining the associations between health services deficits and not having a dental visit in past 12 months. BMC public health. 2019 Dec; 19: 1-3. | ||
| In article | View Article | ||
| [14] | Fakhrjahani I, Tiwari T, Jessani A. A scoping review of oral health outcomes and oral health service utilization of 2SLGBTQ+ people. JDR Clinical & Translational Research. 2024 Jul; 9(3): 199-211. | ||
| In article | View Article | ||
| [15] | Nath S, Poirier BF, Ju X, Kapellas K, Haag DG, Ribeiro Santiago PH, Jamieson LM. Dental health inequalities among indigenous populations: a systematic review and meta-analysis. Caries research. 2021 Jun 9; 55(4): 268-87. | ||
| In article | View Article | ||
| [16] | Moharrami M, Sano Y, Murphy K, Hu X, Clarke J, McLeish S, Fortin Y. Assessing the role of dental insurance in oral health care disparities in Canadian adults. Health Reports. 2024 Apr 1; 35(4): 3-14. | ||
| In article | |||
| [17] | Dahlan R, Ghazal E, Saltaji H, Salami B, Amin M. Impact of social support on oral health among immigrants and ethnic minorities: A systematic review. PloS one. 2019 Jun 20; 14(6): e0218678. | ||
| In article | View Article | ||
| [18] | Hajek A, Kretzler B, Koenig HH. Factors associated with dental service use based on the Andersen model: a systematic review. International journal of environmental research and public health. 2021 Mar 3; 18(5): 2491. | ||
| In article | View Article | ||
| [19] | Tennyson S, Sipple JW, Fiduccia PC, Brunner W, Lembo E, Kjolhede C. School-Based Health Centers and Rural Community Health 1. InCommunity Development and Schools 2024 Jul 29 (pp. 123-138). Routledge. | ||
| In article | View Article | ||
| [20] | Badewy R, Singh H, Quiñonez C, Singhal S. Impact of poor oral health on community-dwelling seniors: a scoping review. Health Services Insights. 2021 Jan; 14: 1178632921989734. | ||
| In article | View Article | ||
| [21] | Brian Z, Weintraub JA. Peer reviewed: oral health and COVID-19: increasing the need for Prevention and Access. Preventing chronic disease. 2020; 17. | ||
| In article | View Article | ||
| [22] | Janto M, Iurcov R, Daina CM, Neculoiu DC, Venter AC, Badau D, Cotovanu A, Negrau M, Suteu CL, Sabau M, Daina LG. Oral health among elderly, impact on life quality, access of elderly patients to oral health services and methods to improve oral health: a narrative review. Journal of personalized medicine. 2022 Feb 28; 12(3): 372. | ||
| In article | View Article | ||
| [23] | Muhammad T, Srivastava S. Tooth loss and associated self-rated health and psychological and subjective wellbeing among community-dwelling older adults: A cross-sectional study in India. BMC Public Health. 2022 Jan 4; 22(1): 7. | ||
| In article | View Article | ||
| [24] | Logan RI, Castañeda H. Addressing health disparities in the rural United States: advocacy as caregiving among community health workers and Promotores de Salud. International Journal of Environmental Research and Public Health. 2020 Dec; 17(24): 9223. | ||
| In article | View Article | ||
| [25] | Probst J, Eberth JM, Crouch E. Structural urbanism contributes to poorer health outcomes for rural America. Health Affairs. 2019 Dec 1; 38(12): 1976-84. | ||
| In article | View Article | ||
| [26] | Peres MA, Macpherson LM, Weyant RJ, Daly B, Venturelli R, Mathur MR, Listl S, Celeste RK, Guarnizo-Herreño CC, Kearns C, Benzian H. Oral diseases: a global public health challenge. The Lancet. 2019 Jul 20; 394(10194): 249-60. | ||
| In article | View Article | ||
| [27] | Amorim LD, Senna MI, Alencar GP, Rodrigues LG, de Paula JS, Ferreira RC. User satisfaction with public oral health services in the Brazilian Unified Health System. BMC oral health. 2019 Dec; 19: 1-9. | ||
| In article | View Article | ||
| [28] | Minervini G, Franco R, Marrapodi MM, Di Blasio M, Ronsivalle V, Cicciù M. Children oral health and parents education status: a cross sectional study. BMC Oral Health. 2023 Oct 24; 23(1): 787. | ||
| In article | View Article | ||
| [29] | Morenz AM, Wescott S, Mostaghimi A, Sequist TD, Tobey M. Evaluation of barriers to telehealth programs and dermatological care for American Indian individuals in rural communities. JAMA dermatology. 2019 Aug 1; 155(8): 899-905. | ||
| In article | View Article | ||
| [30] | Ningrum V, Bakar A, Shieh TM, Shih YH. The oral health inequities between special needs children and normal children in Asia: a systematic review and meta-analysis. InHealthcare 2021 Apr 2 (Vol. 9, No. 4, p. 410). MDPI. | ||
| In article | View Article | ||
| [31] | Arenson M, Hudson PJ, Lee N, Lai B. The evidence on school-based health centers: A review. Global pediatric health. 2019 Feb; 6: 2333794X19828745. | ||
| In article | View Article | ||
| [32] | Murphy K, Gondro JV, Moharrami M. Factors associated with the use of oral health care services among Canadian children and youth. Health Reports. 2024 Apr 1; 35(4): 15-26. | ||
| In article | |||
| [33] | Wong FM, Ng YT, Leung WK. Oral health and its associated factors among older institutionalized residents—a systematic review. International journal of environmental research and public health. 2019 Nov; 16(21): 4132. | ||
| In article | View Article | ||
| [34] | Lambar EF, Thomas G. The health and well-being of North Carolina’s farmworkers: the importance of inclusion, accessible services and personal connection. North Carolina Medical Journal. 2019 Mar 1; 80(2): 107-12. | ||
| In article | View Article | ||
| [35] | Riva F, Seoane M, Reichenheim ME, Tsakos G, Celeste RK. Adult oral health‐related quality of life instruments: a systematic review. Community dentistry and oral epidemiology. 2022 Oct; 50(5): 333-8. | ||
| In article | View Article | ||
| [36] | Kobi J, Nchaw AN, Otieno B. BIG DATA-DRIVEN INSIGHTS FOR EQUITABLE HEALTHCARE ACCESS AND QUALITY FOR US IMMIGRANTS. Journal Title. 2024 Jul; 9(7): 392-408. | ||
| In article | |||
| [37] | Allin S, Farmer J, Quiñonez C, Peckham A, Marchildon G, Panteli D, Henschke C, Fattore G, Lamloum D, Holden AC, Rice T. Do health systems cover the mouth? Comparing dental care coverage for older adults in eight jurisdictions. Health Policy. 2020 Sep 1; 124(9): 998-1007. | ||
| In article | View Article | ||
| [38] | Everaars B, Weening-Verbree LF, Jerković-Ćosić K, Schoonmade L, Bleijenberg N, de Wit NJ, van der Heijden GJ. Measurement properties of oral health assessments for non-dental healthcare professionals in older people: a systematic review. BMC geriatrics. 2020 Dec; 20: 1-8. | ||
| In article | View Article | ||
| [39] | Lipsky MS, Su S, Crespo CJ, Hung M. Men and oral health: a review of sex and gender differences. American journal of men's health. 2021 May; 15(3): 15579883211016361. | ||
| In article | View Article | ||
| [40] | Lebrun-Harris LA, Ghandour RM, Kogan MD, Warren MD. Five-year trends in US children’s health and well-being, 2016-2020. JAMA pediatrics. 2022 Jul 1; 176(7): e220056. | ||
| In article | View Article | ||
| [41] | Wolf TG, Cagetti MG, Fisher JM, Seeberger GK, Campus G. Non-communicable diseases and oral health: an overview. Frontiers in oral health. 2021 Sep 3; 2: 725460. | ||
| In article | View Article | ||
| [42] | Van Der Kruk SR, Butow P, Mesters I, Boyle T, Olver I, White K, Sabesan S, Zielinski R, Chan BA, Spronk K, Grimison P. Psychosocial well-being and supportive care needs of cancer patients and survivors living in rural or regional areas: a systematic review from 2010 to 2021. Supportive Care in Cancer. 2022 Feb 1: 1-44. | ||
| In article | View Article | ||
| [43] | Comim LD, Marquezan PK, Knorst JK, Zanatta FB, Zenkner JE, Alves LS. Association between socioeconomic status and traumatic dental injury in permanent teeth: a systematic review with meta‐analysis. Community dentistry and oral epidemiology. 2024 Aug; 52(4): 424-30. | ||
| In article | View Article | ||
| [44] | Antunes LA, Lemos HM, Milani AJ, Guimarães LS, Küchler EC, Antunes LS. Does traumatic dental injury impact oral health‐related to quality of life of children and adolescents? Systematic review and meta‐analysis. International Journal of Dental Hygiene. 2020 May; 18(2): 142-62. | ||
| In article | View Article | ||
| [45] | Crespo E. The importance of oral health in immigrant and refugee children. Children. 2019. | ||
| In article | View Article | ||



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}