This paper examined the Factors influencing Menstrual Hygiene Management among junior secondary school pupils at Libala, Chilenje and Kamwala. Menstrual hygiene management (MHM) aims at ensuring women and girls can manage their periods in a way that is not only healthy, but that enables their full participation in school, work, and other activities. This study allowed for a better understanding of the factors influencing Menstrual Hygiene Management (MHM) among junior secondary school pupils. The study revealed that most of respondents had good MHM practice and supportive MHM facilities. However, slightly more than half lacked knowledge on menstruation and MHM. Chi-square test revealed that socio demographics had a significant influence on the practice of MHM with a p value of 0.000 at 95% confidence level. Similarly, tradition and cultural concepts as well as home and school environment had significant influence on practice of MHM with a p value of 0.010 and 0.000 respectively at 95% confidence level. On the other hand, Knowledge on menstruation did not show a significant influence on MHM. This was demonstrated by a p value of 0.312 at 95% confidence level. This implies that stakeholders need to address the deficiencies identified in order to ensure safe menstruation and good MHM practice.
Menstruation is the natural bodily process of releasing blood and associated matter from the uterus through the vagina as part of the menstrual cycle 1. Globally, 52% of females are of reproductive age 2. Many girls in low and middle income countries start their menses not knowing about it and without adequate facilities to properly manage it 3.
Menstrual Hygiene Management (MHM) is defined as “a practice in which Women and adolescent girls use a clean material to absorb or collect menstrual blood, and this material can be changed in privacy as often as necessary for the duration of menstruation. MHM also includes using soap and water for washing the body as required, and having access to facilities to dispose of used menstrual management materials” 4. Good MHM requires access to necessary resources (menstrual materials to absorb or collect menstrual blood, soap and water), facilities (private place to wash, change and dry re-usable menstrual materials, in addition to an adequate disposal system for menstrual materials), and education about MHM. However, most schools in developing countries have inadequate facilities including water supply for girls to wash hands, external genitalia and soiled clothes. Nor do they have provision for privacy, soap, sanitary pads and disposal of soiled sanitary 5.
Around the world women and girls have developed their own personal strategies to cope with menstruation, which vary from country to country and depend on economic status, the individual’s personal preferences, local traditions and cultural beliefs and education status 6. The onset of menstruation presents multiple challenges for school girls. Many girls lack the knowledge, support and resources to manage menstruation in school.
In Africa, menstruating women and girls are still often considered ‘dirty’ or ‘impure’ which may lead to forced seclusion, reduced mobility and dietary restrictions. Further, the stigmatization of menstruation has substantial effects on girls’ and women’s education. One in ten girls in Sub-Saharan Africa misses school due to her menstrual cycle which equals to as much as 20% of a given school year 7.
In 2019, Zambia had a projected population of 16,445,079 of which 51% represent females 8. This means that MHM is an area that needs much closer attention, due to its ability to have cross cutting impacts on the social and economic well-being of citizens as it affects sexual reproductive health, education and productivity of females. Despite this reality, little attention has been given to the provision of appropriate and adequate MHM friendly hygiene facilities 9.
The ability for women and girls to manage their periods is affected by a number of factors which include but not limited to demographics, knowledge, social economic factors and environmental factors. Poorly addressing these factors may result in many women and girls managing their menstruation in ineffective and unhygienic ways, which may predispose them to various genito-urinary infections. This would affect class attendace for girls and it could lead to detrimental effects on their quality of life and their overall health. Prioritizing female health in Africa is smart economics for the continent.
MHM has become a globally recognized public health topic but MHM programming is relatively new in Zambia and hence very little research has been conducted around menstruation 9. Most studies on MHM have been done in the rural area but limited studies have been documented to have been done in the urban area. Therefore, undertaking this study yielded new information on factors influencing MHM practice among selected urban junior secondary school pupils in Lusaka (Libala, Chilenje South and Kamwala secondary Schools).
This was a school based cross-sectional study which was conducted among grade 9 pupils in an urban area of Lusaka district. The sample size in this study comprised of 168 respondents, 56 female grade 9 pupils were selected using random sampling method from each of the selected Schools. The sample was calculated using Cochran formula and modified Cochran formula. The Cochran formula is as follows; no = Z2 pq/e2, where; no is the Cochran’s sample size recommendation, e is the desired level of precision (i.e. the margin of error), p is the (estimated) proportion of the population which has the attribute in question, q is 1 – p and Z is the z-statistics for the desired level of confidence. Modified Cochran formula is as follows; n = no/ 1 + (no - 1)/ N, Where; no is Cochran’s sample size recommendation, N is the population size, n is the new, adjusted sample size.
A self-administered semi structured questionnaire was used to collect data in English. Pupils chose one option unless specified otherwise. Open-ended questions were given wherever description of answers was required. Completed questionnaires were compiled and entered into SPSS version 25 and chi-square was used to test the significance. Descriptive and inferential statistics such as frequency tables, percentages and bar graphs were also be used to ensure easy understanding of data collected. Findings from the study have been presented according to the sequence of questions in the questionnaire in order to show relationships.
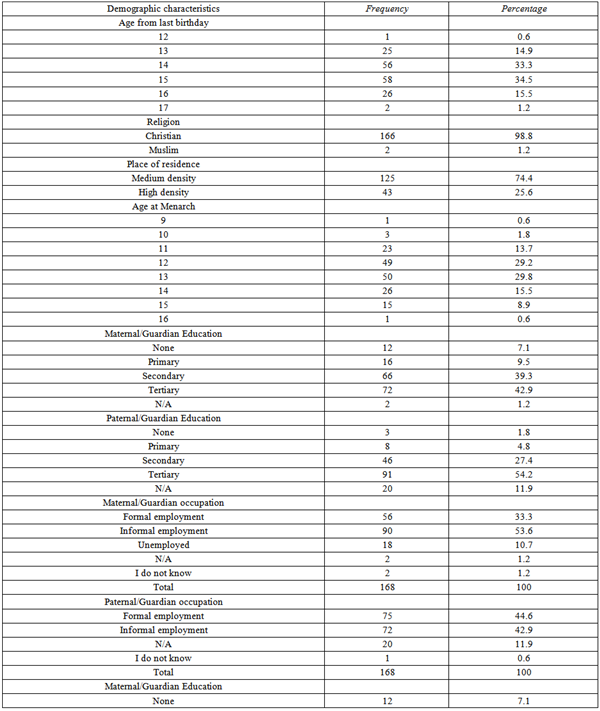
Data for this study was collected from a total of 168 respondents from the three selected secondary schools (see Table 1). This study had a response rate of 100% as of the 168 questionnaires that were administered to respondents, 168 questionnaires were returned and analyzed. The age group of respondents was from 12 to 17 years with a modal age of 15 years. Majority 98.8% (166) of the respondents were Christians while 2 (1.2%) were Muslim. Of the 168 respondents, 74.4% (125) respondents were from medium density areas while 25.6% (43) were from high density areas. Thirteen (13) was the mean, mode and median age at menarche represented by 29.8% (50), however it is cardinal to note that the age at menarche was normally distributed ranging from 9 to 16 years. 42.9% (72) of the maternal parents/guardians had reached tertiary level of education while 7.1% (12) had no level of education. Slightly more than half 54.2% (91) of the paternal parents/guardians had attained tertiary education while 1.8% (3) had no level of education. More than half of the maternal parents/guardians 53.6% (90) were in informal employment while 10.7% (18) were unemployed. About 44.6% (75) paternal parents/guardians were in formal employment while 42.9% (72) were in informal employment.
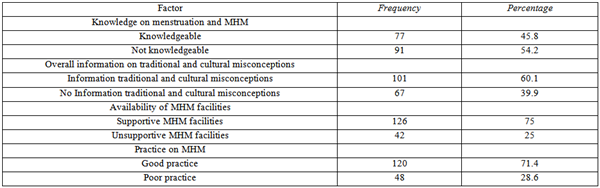
Table 2 shows results on Knowledge on menstruation and menstrual hygiene, information on traditional and cultural misconceptions and practice on MHM. Of the 168 respondents, 45.8% were knowledgeable while 54.2% were not knowledgeable about menstruation and MHM. In addition, 60.1% (101) did not have information on tradition and cultural misconceptions and myths while 39.9% (67) had information on tradition and cultural misconceptions and myths. Furthermore, 71.4% (120) have good practice while 28.6% (48) have poor practice.
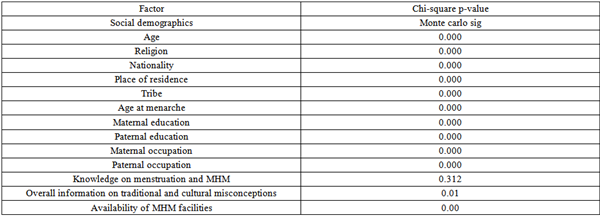
Table 3 shows factors influencing the practice of MHM among pupils. The influence of social demographic factors (age, religion, place of residence, age at menarche, maternal education, paternal education, maternal occupation and paternal occupation) on the practice of MHM was found to be statistically significant p value of 0.000 at 95% confidence level. In addition, the association between Knowledge on menstruation and the practice of MHM was not statistically significant as indicated by p value of 0.312. Furthermore, the association between tradition and cultural misconceptions, and the practice of MHM was statistically significant as indicated by p value of 0. 01. Finally, the association between availability of MHM facilities with the practice of MHM was statistically significant as indicated by p value of 0.000.
The modal age of the respondents was 15 years with a frequency of 58 at 34.5%, followed by 14 years with a frequency of 56 at 33.3% and the lowest was 12 years with a frequency of 1 at 0.6%. The reason for having 15 years as the modal class could be that approximately 42.7% of female pupils in Lusaka province started school at 7 years 9. This translates to being 15 years in grade 9 excluding failure and other circumstances that can delay grade progression.
Majority 98.8% (166) of the respondents were Christian while 1.2% (2) were Muslim. This data distribution could be attributed to the fact that Christianity is a widely practiced religion in Zambia. According to the 2010 census of population and housing, in terms of religious affiliation, Protestants and Catholics made up 75% and 20.2% of the population respectively. Muslims and other religious affiliations made up 2.5% of the Zambian population 10. This showed that majority (95.2%) of Zambians are Christians by religion. Furthermore, Zambia was declared a Christian nation by its second republican president Dr Fredrick Chiluba in 1991 5. This declaration could have affirmed the practice of Christianity in Zambia and could also be a reason why most the respondents were Christians.
The findings on place of residence revealed that 74.4% (125) respondents were from medium density areas while 25.6% (43) were from high density areas. This could be due to the fact that the target schools are surrounded by medium and high density residential places.
The respondents belonged to 15 tribes of which most 64% (38.1) were Bemba and majority 98.8% (166) of the respondents were Zambian while 0.6% was South African and 0.6% (1) was Tanzanian. This finding could be due to the fact that people from different provinces and tribes migrate to Lusaka in search of jobs and business opportunities. This is because it is among the highly industrialised districts owing to the fact that it is the capital city of Zambia.
The age at menarche was a normal distribution with a range of 9 to 16 years and 13 years represented by 29.8% (50) as the mean, mode and median. This is similar to what was found in a study on MHM in Zambia by Kaoma (2018) 12. This study found the median age at menarche to be 13.
Out of 168 respondents, 42.9% (72) of the maternal parents/guardians had reached tertiary level of education while 7.1% (12) had not been to school and slightly more than half 54.2% (91) of the paternal parents/guardians had attained tertiary education while 1.8% (3) had not been to school. This data distribution could be due to the fact that men have a slightly greater education attainment than men. A conclusion similar to the Zambia Demographic Health Survey (ZDHS) 2018 finding where 8% of women were found to have no formal education, compared with only 4% of men and only 6% of women and 8% of men have attended or completed tertiary education 7.
Most 53.6% (90) maternal parents/guardians were in informal employment while 10.7% (18) were unemployed and more 44.6% (75) paternal parents/guardians were in formal employment while 42.9% (72) were in informal employment with none unemployed. These findings imply that men are more likely to be employed than women. This is similar to findings ZDHS findings where Men were found to be more likely (75%) to be currently employed than women (45%) and 21% of men and 48% of women were not employed in the 12 months preceding the survey 11.
Regarding knowledge on menstruation and MHM, this study found that most respondents did not know the physiological basis of menstruation. This is similar to a study by Chinyama et al 2019 10 who found that despite the Zambian school curriculum covering menstruation as part of health science subjects, the majority of the girls did not know its physiological basis.
Furthermore, overall knowledge of the respondents on menstruation and MHM was limited as only 45.8% of the 168 respondents were knowledgeable. Unlike this study findings, a study by Koirr et al (2018) 13 on MHM practices among primary school girls from a pastoralist community in Kenya found that overall, 51.6% had good menstruation knowledge while 23.4% and 25% had average and poor knowledge respectfully. This could be probably be due to the fact that Kenya is more keen on ensuring that MHM is taught in schools and that MHM sensitization is being conducted on a regular basis. Based on this background, There is need to strengthen MHM in reproductive health education to empower girls through detailed MHM information in the school sexual reproductive and health education curriculum so that girls and teachers are equally informed and can support girls to practice MHM effectively.
Traditional and cultural misconceptions revealed information on foods forbidden to eat when menstruating, social or religious restrictions during menstruation, activities forbidden and some traditional myths know by the respondents. The following were responses with the highest frequencies respectively; 8.3% (14) stated that food with a lot of salt is forbidden because it causes extreme period pains, 29.7% (50) stated putting salt in relish as a restriction as it causes a cough (TB or pneumonia), 45% (75) stated that running is a forbidden activity during menstruation because the pad or menstrual material can fall off and throwing pads anyhow would predispose one to being bewitched by witches.
Forbidding menstruating women to eat certain food or restricting them to perform certain activities is quiet common in the African culture. This is demonstrated by several studies that have been conducted. For instance, Mutunda (2018) 14 found that menstruating girls are forbidden to do certain things when preparing food, as doing so is believed to transmit a variety of diseases to men. Most seriously, and known to all girls, is the belief that when menstruating females add salt to a dish, and when the dish is consequently consumed by a man, the latter might develop chest pains and/or pneumonia or even contract TB. Another study by Korrir et al (2018) 13 in Kenya found that Muslim and traditional religious groups considered menstruating girls unclean and prohibited their participation in any social forums, including school, which left girls ostracized and alienated. These myths and beliefs impact how menstruating girls are treated which may lead them to hide that they are menstruating in fear of being accused of causing disease. This may consequently affect how they practice their MHM.
Overall, more 60.1% (101) did not have information on tradition and cultural misconceptions and myths. This could be because the respondents are from an urban area and are less exposed to tradition.
Overall, the respondents had supportive MHM facilities as 75% (126) of the 168 respondents had supportive home and school MHM facilities. This is in contrast to what the study done in rural Zambia found by Chinyama et al (2019) 10 where toilets in most of the schools did not meet World Health Organization (WHO) functional standards because they had no doors, locks, anal cleansing materials, water, and soap or ash. Unlike rural Zambia, Schools in Urban Zambia are trying to meet the National MHM guidelines which prescribe that MHM facilities provide menstruating girls with privacy and space for changing, cleaning, drying or discarding materials, as well as water for personal hygiene. This provides a conducive environment for girls to practice good MHM. The reason for this could be that resources are easily accessible in urban areas as compared to rural areas.
The practice of good MHM found to be 71.4% (120). Despite this being a good percentage, there still more than 20% of respondents that need to be enlightened on safer and better ways of MHM practice. A study by Korir et al (2018) 13 found that poor MHM practices were documented in 28.8% of primary school girls from a pastoralist community in Kenya, results similar to findings of this study. This could be because both studies were done in schools and that WASH facilities were equally similar.
In this study, Social demographic variables were found to have a statistically significant influence on MHM. Similarly, Shallo et al (2018) 15, found that variables like age, religion, father’s educational status ad frequency of discussing menses with mothers’ were significantly associated with MHM practice in Ambo city of Ethiopia. On the contrary, a study in Kenya by Korir et al (2018) 13, found that the only socio-demographic factors that are associated with poor MHM were age and religion. This shows that different socio-demographic factors influence MHM practice depending on the country and cultural context.
Further, information on tradition and cultural concepts as well as availability of MHM facilities were found to have influence on the practice of MHM at 95% confidence level with a p-value of 0.000.
Knowledge on the other hand does not a significant influence on MHM. This is demonstrated by a p value of 0.312 at 95% confidence level. This result could be due to high percentage 71.4% of good MHM practice despite the low knowledge levels. Therefore, it cannot be concluded that knowledge does not have influence on one’s MHM practice. It would be best if more studies exploring the influence of knowledge on MHM practice were done. This would improve the general understanding of the relationship between the two variables.
In conclusion evidence from this study shows that most of respondents had good MHM practice and generally most of the respondents had supportive MHM facilities. Furthermore, slightly more than half lacked knowledge on menstruation and MHM. To address this Ministry of General Education and other stakeholders should develop elaborate curricula for MHM at primary and secondary school level as well as support publication of books on MHM. This will increase the knowledge and understanding of pupils on menstruation and MHM. In addition, Ministry of General Education should work in collaboration with Ministry of infrastructure, housing and Urban Development and other stakeholders in ensuring that WASH facilities in schools are constructed with consideration of MHM. Chi-square test revealed that socio demographics had a significant influence on the practice of MHM with a p value of 0.000 at 95% confidence level. Similarly, tradition and cultural concepts as well as home and school environment had significant influence on practice of MHM with a p value of 0.010 and 0.000 respectively, significant at 95% confidence level. MHM is a critical component of reproductive health and an important entry point for adolescent sexual and reproductive health. Therefore, Ministry of health and other stakeholders should incorporate MHM in school health services. This will reemphasize the importance of practicing MHM and consequently prevent urogenital infections thus improving sexual and reproductive health of females during their school years. Finally, more studies on MHM in both rural and urban should be done so that MHM practice is fully understood and improved.
Gratitude goes to District Education Board Secretary (DEBS) Lusaka and head teachers and the staff for granting permission to collect data at Kamwala, Libala and Chilenje South Secondary schools. Gratitude also goes our families for the support rendered throughout the period of conducting this research. Finally and most importantly we are highly indebted to God Almighty for his presence in our lives, good health and the guidance throughout the preparation and finalization of this paper.
| [1] | UNICEF. (2019) Guidance on Menstrual Health and Hygiene, 1st Ed. Newyork; UNICEF. | ||
| In article | |||
| [2] | House, S., Mahon, T. & Cavill, S. (2013) Bookshelf: Menstrual Hygiene Matters: a resource for improving menstrual hygiene around the world, Reproductive Health Matters 21(41): 257–59. | ||
| In article | View Article | ||
| [3] | Sumpter, C. and Torondel, B. (2013) A systematic review of the health and social effects of menstrual hygiene management, PLoS ONE 8(4): e62004. | ||
| In article | View Article PubMed | ||
| [4] | WHO & UNICEF (2012) Progress on drinking water and sanitation: Joint Monitoring Programme update. [online] Available at <https:// www.who.int/ water_sanitation_health/ publications/jmp_report-2012/en/> [Accessed on 08.01.2020]. | ||
| In article | |||
| [5] | Cheyeka, A.M., 2016. Zambia, a ‘Christian nation’in Post Movement for Multiparty Democracy (MMD) Era, 2011–2016. International Journal of Humanities and Social Science, 6(7), pp.159-172. | ||
| In article | |||
| [6] | Biruk. E, Tafera. W, Tadesse. N & Sisay. A (2018), Assessment of Menstrual Hygiene Management and its Determinants among Adolescent girls in Addis Ababa Ethiopia, [online] Available at <https://www.biorxiv.org/content/10.1101/450007v2.full> [accessed on 17.03.2020]. | ||
| In article | |||
| [7] | WHO (2018) Stigmatization of Menstruation [online] Available at <http://modelun.com/cjmunc/wp-content/ uploads/sites/14/ 2018/05/WHO-Stigmatization-of-Menstruation-1.pdf> [Accessed on 20.03.2020]. | ||
| In article | |||
| [8] | CSO. (2019) Zambia’s population [online] Available at <https://www.cso.ie/en/csolatestnews/2019/> [Accessed on 20.03.2020]. | ||
| In article | |||
| [9] | Ministry of Education (2016). Menstrual Hygiene Management National Guidelines-Zambia [online] Available at <https:// www.washinschoolsindex.com/document/190> [Accessed on 7.01.2020. | ||
| In article | |||
| [10] | Chinyama, J., Chipungu, J., Rudd, C. et al. (2019) Menstrual hygiene management in rural schools of Zambia: a descriptive study of knowledge, experiences and challenges faced by schoolgirls. BMC Public Health 19(16). | ||
| In article | View Article PubMed | ||
| [11] | Zambia Statistics Agency, Ministry of Health (MOH) Zambia, and ICF. 2019. Zambia Demographic and Health Survey 2018. Lusaka, Zambia, and Rockville, Maryland, USA: Zambia Statistics Agency, Ministry of Health, and ICF. | ||
| In article | |||
| [12] | Kaoma. S.N, (2018), Menstrual Hygiene Management in Zambia, Health Press Zambia Bull 2(5).p 1-3 [online] Available at <http:// znphi.co.zm/thehealthpress/menstrual-hygiene-management-in-zambia/> [accessed on 07.02.2020]. | ||
| In article | |||
| [13] | Korir. E, kwara. G & Okumbe G, (2018) Menstrual hygiene management practices among primary school girls from a pastoralist community in Kenya: a cross sectional survey, Pan African Medical Journal 31(222); PMC 6691306 [online] Available at <https:// www.ncbi.nlm.nih.gov/ pmc/articles/ PMC6691306/#> [Accessed on 07.02.2020]. | ||
| In article | View Article PubMed | ||
| [14] | Mutunda. A. (2013). Factors Impacting on the Menstrual Hygiene among School Going Adolescent Girls in Mongu District, ZambiaI. MPH thesis. University of the Western Cape. | ||
| In article | |||
| [15] | Shallo. S.A, Willi. W & Abubakar A. (2018) Menstrual hygiene management practice and factors affecting it among high school females in Ambo City, Oromia state, Ethiopia, 2018: A cross-sectional mixed method, [online] Available at <https:// www.biorxiv.org/ content/10.1101/806422v1.full> [Accessed on 18.03.2020]. | ||
| In article | View Article | ||
Published with license by Science and Education Publishing, Copyright © 2024 Abigail Chuma Kalemba, Ireen Kamoto Phiri and Oliver Phiri
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | UNICEF. (2019) Guidance on Menstrual Health and Hygiene, 1st Ed. Newyork; UNICEF. | ||
| In article | |||
| [2] | House, S., Mahon, T. & Cavill, S. (2013) Bookshelf: Menstrual Hygiene Matters: a resource for improving menstrual hygiene around the world, Reproductive Health Matters 21(41): 257–59. | ||
| In article | View Article | ||
| [3] | Sumpter, C. and Torondel, B. (2013) A systematic review of the health and social effects of menstrual hygiene management, PLoS ONE 8(4): e62004. | ||
| In article | View Article PubMed | ||
| [4] | WHO & UNICEF (2012) Progress on drinking water and sanitation: Joint Monitoring Programme update. [online] Available at <https:// www.who.int/ water_sanitation_health/ publications/jmp_report-2012/en/> [Accessed on 08.01.2020]. | ||
| In article | |||
| [5] | Cheyeka, A.M., 2016. Zambia, a ‘Christian nation’in Post Movement for Multiparty Democracy (MMD) Era, 2011–2016. International Journal of Humanities and Social Science, 6(7), pp.159-172. | ||
| In article | |||
| [6] | Biruk. E, Tafera. W, Tadesse. N & Sisay. A (2018), Assessment of Menstrual Hygiene Management and its Determinants among Adolescent girls in Addis Ababa Ethiopia, [online] Available at <https://www.biorxiv.org/content/10.1101/450007v2.full> [accessed on 17.03.2020]. | ||
| In article | |||
| [7] | WHO (2018) Stigmatization of Menstruation [online] Available at <http://modelun.com/cjmunc/wp-content/ uploads/sites/14/ 2018/05/WHO-Stigmatization-of-Menstruation-1.pdf> [Accessed on 20.03.2020]. | ||
| In article | |||
| [8] | CSO. (2019) Zambia’s population [online] Available at <https://www.cso.ie/en/csolatestnews/2019/> [Accessed on 20.03.2020]. | ||
| In article | |||
| [9] | Ministry of Education (2016). Menstrual Hygiene Management National Guidelines-Zambia [online] Available at <https:// www.washinschoolsindex.com/document/190> [Accessed on 7.01.2020. | ||
| In article | |||
| [10] | Chinyama, J., Chipungu, J., Rudd, C. et al. (2019) Menstrual hygiene management in rural schools of Zambia: a descriptive study of knowledge, experiences and challenges faced by schoolgirls. BMC Public Health 19(16). | ||
| In article | View Article PubMed | ||
| [11] | Zambia Statistics Agency, Ministry of Health (MOH) Zambia, and ICF. 2019. Zambia Demographic and Health Survey 2018. Lusaka, Zambia, and Rockville, Maryland, USA: Zambia Statistics Agency, Ministry of Health, and ICF. | ||
| In article | |||
| [12] | Kaoma. S.N, (2018), Menstrual Hygiene Management in Zambia, Health Press Zambia Bull 2(5).p 1-3 [online] Available at <http:// znphi.co.zm/thehealthpress/menstrual-hygiene-management-in-zambia/> [accessed on 07.02.2020]. | ||
| In article | |||
| [13] | Korir. E, kwara. G & Okumbe G, (2018) Menstrual hygiene management practices among primary school girls from a pastoralist community in Kenya: a cross sectional survey, Pan African Medical Journal 31(222); PMC 6691306 [online] Available at <https:// www.ncbi.nlm.nih.gov/ pmc/articles/ PMC6691306/#> [Accessed on 07.02.2020]. | ||
| In article | View Article PubMed | ||
| [14] | Mutunda. A. (2013). Factors Impacting on the Menstrual Hygiene among School Going Adolescent Girls in Mongu District, ZambiaI. MPH thesis. University of the Western Cape. | ||
| In article | |||
| [15] | Shallo. S.A, Willi. W & Abubakar A. (2018) Menstrual hygiene management practice and factors affecting it among high school females in Ambo City, Oromia state, Ethiopia, 2018: A cross-sectional mixed method, [online] Available at <https:// www.biorxiv.org/ content/10.1101/806422v1.full> [Accessed on 18.03.2020]. | ||
| In article | View Article | ||