Background: Cancer patients receiving chemotherapy are highly vulnerable to environmental infections due to treatment-induced immunosuppression, yet bacterial contamination and antibiotic resistance patterns in African oncology facilities remain uncharacterized. We conducted a comprehensive environmental surveillance of a West African chemotherapy unit to identify infection risks threatening these vulnerable patients. Methods: We collected 39 environmental samples (36 surfaces, 3 air) from high-touch sites across the chemotherapy unit at Centre National de Radiothérapie et d'Oncologie Médicale Alassane Ouattara (August-October 2024). Bacterial isolates underwent identification using conventional methods and API systems, with antimicrobial susceptibility testing by Kirby-Bauer disk diffusion under EUCAST 2023 guidelines. Extended-spectrum β-lactamase (ESBL) production was confirmed by double-disk synergy testing. Results: Surface contamination occurred in 63.9% of samples; air remained sterile. Twenty-nine isolates recovered: Bacillus spp. (34.5%), coagulase-negative staphylococci (27.6%), Pseudomonas aeruginosa (20.7%), Enterobacteriaceae (17.2%). Water sources harbored Pseudomonas and ESBL-producers. Resistance was substantial: 40% Enterobacteriaceae produced ESBLs with fluoroquinolone co-resistance, 14.3% coagulase-negative staphylococci exhibited methicillin/aminoglycoside resistance, all P. aeruginosa (6/6) showed intermediate colistin susceptibility. Bacillus demonstrated aminopenicillin resistance but carbapenem susceptibility. No carbapenemase-producers detected. Conclusions: This chemotherapy unit surveillance reveals concerning environmental contamination with resistant opportunistic pathogens. Bacillus predominance and water-associated Pseudomonas/ESBL-Enterobacteriaceae colonization highlight unique tropical ecology patterns. Enhanced cleaning protocols, water system management, and antimicrobial stewardship adapted to local resistance are urgently needed. These baseline data inform infection prevention programs protecting vulnerable African cancer patients.
Healthcare-associated infections present a persistent threat to hospitalized patients worldwide, with particularly devastating consequences in vulnerable populations such as cancer patients undergoing chemotherapy. While wealthy nations report infection rates around 4-5%, resource-limited countries in Africa, Latin America, and Asia face substantially higher burdens reaching 14-18% 1, 2. These stark disparities reflect not only differences in healthcare infrastructure but also gaps in infection surveillance systems and prevention resources that leave the world's most vulnerable patients inadequately protected.
Within hospitals, the physical environment including bed rails, medical equipment, sinks, and frequently touched surfaces serves as an often-overlooked reservoir for disease-causing bacteria. These environmental niches harbor diverse microbial communities originating from patients, healthcare workers, and visitors, creating complex transmission networks 3. Though debate continues regarding the precise role of environmental contamination in causing infections, mounting evidence demonstrates that hospital surfaces act as important stepping stones in spreading dangerous drug-resistant organisms like methicillin-resistant Staphylococcus aureus (MRSA) 4, 5. The microbial composition of healthcare facilities fluctuates based on patient populations served, medical procedures performed, antibiotic usage patterns, and cleaning practices employed 6, 7. For patients with weakened immune systems particularly those receiving chemotherapy these environmental bacteria pose extraordinary risks, as even organisms typically considered harmless can cause life-threatening infections when the body's defenses are compromised. Chemotherapy drugs, while targeting cancer cells, simultaneously devastate the immune system 8. Extended hospitalizations during neutropenic episodes provide ample opportunity for patients to acquire hospital-adapted organisms that have evolved resistance to multiple antibiotics. Despite extensive research examining environmental microbiology in intensive care units, surgical suites, and other high-risk hospital areas 9, 10, a critical knowledge gap exists regarding bacterial contamination in oncology chemotherapy units, especially across sub-Saharan Africa. This vast region confronts unique challenges that amplify infection risks 11, 12.
The Centre National de Radiothérapie et d'Oncologie Médicale Alassane Ouattara (CNRAO) in Abidjan, Côte d'Ivoire, serves as the country's premier cancer treatment facility, delivering life-saving chemotherapy to patients from across the nation. Very few studies have mapped out the bacteria present and antibiotic resistance patterns in chemotherapy units across West Africa. Our study addresses this major gap by offering a clear microbiological snapshot of an oncology chemotherapy department in sub-Saharan Africa.
This study aimed to (i) characterize bacterial contamination patterns in a chemotherapy unit, (ii) identify species distribution, and (iii) assess antimicrobial resistance profiles of recovered isolates.
A cross-sectional environmental surveillance study was conducted from August 15 to October 15, 2024, at the chemotherapy unit of Centre National de Radiothérapie et d'Oncologie Médicale Alassane Ouattara (CNRAO), Abidjan, Côte d'Ivoire. The unit comprises eight infusion bays, individual patient rooms, a treatment room, and physician offices, serving approximately 120 immunocompromised patients monthly.
2.2. Sample CollectionEnvironmental sampling targeted high-touch surfaces and air quality across four zones: (i) individual patient rooms (n=7 sites: bedside table, bed rail, door handle, mattress, infusion pole, sink, air intake), (ii) infusion bays (n=11 sites: bed rail, lighting fixture, mattress, curtain, sink, infusion pole, oxygen device, medication cart, door handle, air intake, waste area), (iii) treatment room (n=5 sites: examination bed, mattress, sink, infusion pole, medication cart), and (iv) physician office (n=3 sites: patient chair, door handle, sink). We conducted a one-time cross-sectional survey between chemotherapy sessions to capture a realistic “snapshot” of contamination levels across the high-touch surfaces and air zones. This design is efficient and resource-friendly, allowing us to assess environmental risk without disrupting clinical operations. Regular surface cleaning activities were carried out in the morning before the service opened and after closing. Samples were therefore not taken immediately after the morning cleaning.
Surface samples were collected using sterile cotton swabs pre-moistened with physiological saline, employing the double-swab technique with parallel then perpendicular strokes (23). The areas of the surfaces sampled were standardised to an average of 26 cm². Air sampling utilized passive settle plates (nutrient agar exposed for 20 minutes at 1.2-1.5 m height). Samples were transported to the laboratory within 30 minutes.
2.3. Microbiological AnalysisSwabs underwent enrichment in brain-heart infusion broth at 37°C for 24-48 hours. Enrichment cultures were streaked onto selective media: nutrient agar (total counts), EMB agar (Gram-negatives), Hektoen enteric agar (enteric pathogens), blood agar (fastidious organisms), cetrimide agar (Pseudomonas), bile-esculin azide agar (Enterococcus), and mannitol salt agar (staphylococci). Plates were incubated at 37°C for 24-72 hours. Pure isolates were obtained by iterative subculture using four-quadrant streaking.
Bacterial identification employed standard methods: Gram staining, catalase and oxidase testing, and biochemical characterization using Leminor miniaturized galleries for Enterobacteriaceae. API 20E and API 20NE systems (bioMérieux, France) provided confirmatory identification. Staphylococcus species were differentiated by coagulase and DNase testing. Bacillus species were identified by characteristic morphology (3-5 μm rods with square ends).
2.4. Antimicrobial Susceptibility TestingAntibiotic resistance was determined by Kirby-Bauer disk diffusion on Mueller-Hinton agar following SFM/EUCAST 2023 guidelines (25). Inocula (0.5 McFarland standard) were flooded onto pre-dried plates. Antibiotic panels included:
Enterobacteriaceae (n=14): ampicillin, amoxicillin-clavulanate, mecillinam, cefoxitin, cefotaxime, ceftazidime, cefepime, meropenem, imipenem, gentamicin, amikacin, ciprofloxacin, levofloxacin, fosfomycin.
Non-fermenters (n=11): ampicillin, ticarcillin-clavulanate, ceftazidime, cefepime, imipenem, meropenem, tobramycin, amikacin, ciprofloxacin, levofloxacin, colistin.
Staphylococci (n=10): cefoxitin, gentamicin, tobramycin, kanamycin, erythromycin, tetracycline, fusidic acid, rifampicin, norfloxacin, moxifloxacin.
Bacillus (n=6): ampicillin, amoxicillin-clavulanate, gentamicin, tetracycline, imipenem, meropenem.
Disks were placed ≥15 mm from plate edges and ≥30 mm apart. After pre-diffusion, plates were incubated at 37°C for 18-20 hours. Inhibition zones were measured with digital calipers and interpreted per SFM/EUCAST 2023 breakpoints. Quality control employed Escherichia coli ATCC 25922, Staphylococcus aureus ATCC 25923, and Pseudomonas aeruginosa ATCC 27853.
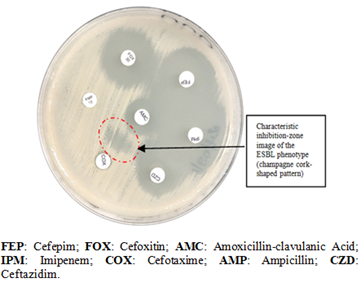
ESBL production was confirmed by double-disk synergy testing with ceftazidime/cefotaxime and amoxicillin-clavulanate (20-25 mm apart). Methicillin resistance was screened using cefoxitin disks (27). MDR was defined as non-susceptibility to ≥1 agent in ≥3 antimicrobial categories (28).
2.5. Data AnalysisData were recorded on standardized forms and analyzed using Microsoft Excel 2016 and Epi Info 7.2.3.1. Descriptive statistics included frequencies and percentages for categorical variables (species distribution, contamination rates, resistance patterns). Results were visualized using tables and diagrams.
2.6. Ethicals ConsiderationsThis environmental surveillance was approved by CNRAO administration as part of routine infection control activities. No human subjects or patient samples were involved. Biosafety level 2 protocols were followed per WHO guidelines.
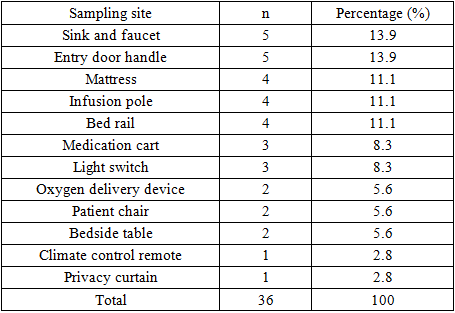
We systematically examined 39 sites across the Chemo-therapy unit over two months, focusing predominantly on physical surfaces (36 samples, 92.3%) with limited air sampling (3 samples, 7.7%). The shared infusion bay, where patients spend hours receiving treatment, contributed nearly one-third of specimens (30.8%). Individual patient rooms, treatment areas, and physician offices accounted for 28.2%, 23.1%, and 17.9% respectively.
Water sources sinks and faucets and frequently touched door handles each represented 13.9% of surface samples, followed by patient contact surfaces: mattresses, infusion poles, and bed rails (11.1% each) (Table 1) This deliberate sampling strategy targeted surfaces identified as critical transmission points for healthcare-associated pathogens.
Surface samples yielded positive bacterial cultures in 63.9% of cases (23/36), revealing substantial environmental microbial burden despite routine disinfection protocols. In contrast, all air samples (3/3) remained sterile.
The positive culture rate among surfaces varied by location, with shared infusion areas and water sources demonstrating higher contamination frequency compared to low-touch vertical surfaces.
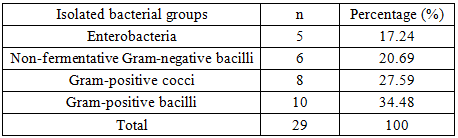
3.3. Bacterial Diversity and Taxonomic DistributionTwenty-nine bacterial isolates were recovered from positive cultures, representing diverse taxonomic groups reflective of environmental, skin commensal, and opportunistic pathogen reservoirs. Gram-positive bacilli predominated (34.5%, 10/29), followed by Gram-positive cocci (27.6%, 8/29), non-fermenting Gram-negative bacilli (20.7%, 6/29), and Enterobacteriaceae (17.2%, 5/29).
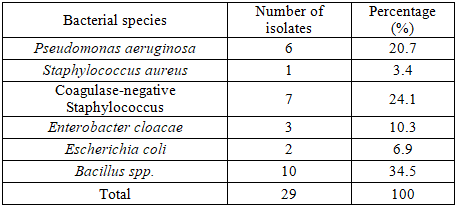
At the species level, Bacillus spp. emerged as the most prevalent organism (34.5%, 10/29), consistent with ubiquitous environmental spore-forming bacilli capable of surviving standard disinfection procedures. Coagulase-negative staphylococci (CoNS) ranked second (24.1%, 7/29). Pseudomonas aeruginosa, a notorious opportunistic pathogen in immunocompromised hosts, accounted for 20.7% of isolates (6/29), predominantly recovered from water-associated sites. Enterobacteriaceae comprised Escherichia coli (6.9%, 2/29) and Enterobacter cloacae (10.3%, 3/29), with Staphylococcus aureus detected as a single isolate (3.4%, 1/29). (Table 3)
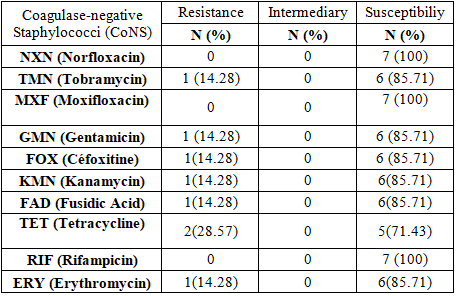
The single Staphylococcus aureus isolate demonstrated pan-susceptibility to all tested agents including cefoxitin (methicillin-susceptible, MSSA), aminoglycosides, fluoroquinolones, rifampicin, tetracycline, and fusidic acid. However, macrolide resistance was detected (erythromycin-resistant), suggesting potential inducible clindamycin resistance (MLSb phenotype).
Among the seven coagulase-negative Staphylococcus (CoNS) strains studied, one strain was methicillin-resistant (MR-CoNS) and showed resistance to kanamycin, tobramycin, and gentamicin (KTG phenotype). This strain was isolated from a swab of the Privacy curtain (paravent) of the common chemotherapy room (Table 4).
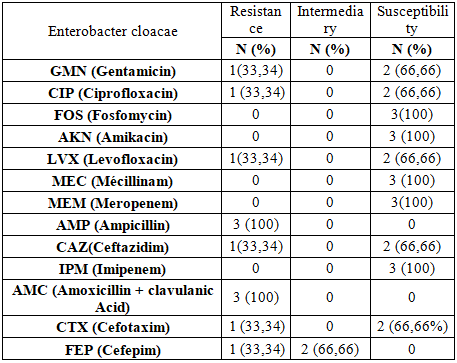
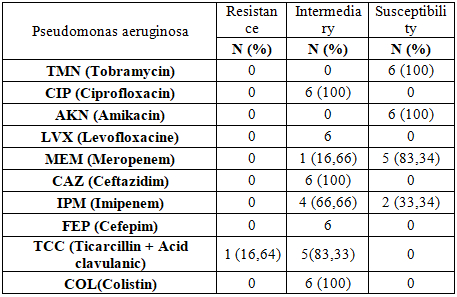
Of the two Escherichia coli isolates obtained, one was an extended-spectrum β-lactamase (ESBL) producer. This strain originated from the specimen collected from the sink in Category Room No. 2 (Figure 1). Among the three Enterobacter cloacae strains isolated, one was an extended-spectrum β-lactamase (ESBL) producer associated with resistance to fluoroquinolones (Table 5). This strain was isolated from the sample collected from the infirmary sink. All Pseudomonas aeruginosa isolates exhibited intermediate susceptibility to colistin, and one isolate was resistant to ticarcillin + clavulanic acid (TCC) (Table 6)
All Bacillus spp. isolates were resistant to amoxicillin-clavulanic acid (AMC) and ampicillin (AMP); conversely, they were all susceptible to gentamicin (GMN) and meropenem (MEM).
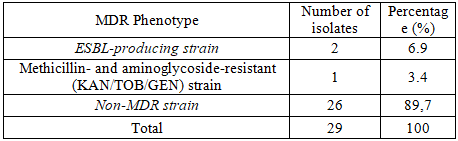
Overall, most environmental isolates (89.7 %) belonged to the non-MDR category. ESBL-producing and methicillin-plus-aminoglycoside-resistant strains made up 6.9 % and 3.4 % of isolates, respectively (Table 7)
This cross-sectional surveillance study provides one of the first comprehensive characterization of the bacterial ecosystem and antimicrobial resistance landscape in a West African chemotherapy unit, revealing substantial environmental contamination with clinically relevant opportunistic pathogens and emerging resistance phenotypes.
Surface contamination was detected in 63.9% of sampled sites, substantially exceeding rates reported in previous African healthcare facility surveys. Meité et al. documented 46.4% positivity in surgical intensive care units in Côte d'Ivoire 13, while Samira et al. found 40% contamination in Algerian hospital environments 14. This elevated burden may reflect several converging factors: the open-bay infusion area design facilitating cross-contamination between adjacent patient stations, high patient throughput with frequent surface contact during prolonged chemotherapy sessions, potential gaps in environmental cleaning frequency or technique, and tropical climate conditions favoring microbial survival on fomites.
During neutropenic nadirs, patients lose their primary defense against bacterial invasion, rendering environmental pathogens that pose negligible risk to immunocompetent individuals capable of causing life-threatening bacteremia and sepsis 15. The documented recovery of Pseudomonas aeruginosa, Enterobacteriaceae, and methicillin-resistant staphylococci from high-touch surfaces establishes plausible transmission pathways for healthcare-associated infections in this vulnerable population.
Interestingly, all air samples (3/3) yielded sterile results despite substantial surface contamination. This discordance likely reflects multiple factors: passive settle plate methodology demonstrates limited sensitivity for airborne bacteria compared to active volumetric sampling 16, the sampling duration may have been insufficient to capture transient airborne events, and functional HVAC systems in sampled zones may effectively remove airborne particles.
The predominance of Gram-positive bacilli (34.5%), specifically Bacillus spp., represents a notable departure from typical nosocomial ecology where Gram-negative organisms dominate in most high-income country surveillance studies 17. This finding aligns more closely with environmental microbiology studies from tropical regions where spore-forming bacilli persist despite disinfection protocols. Andrianjafy et al. in Madagascar 18 and Barbosa et al. in Brazil 19 similarly reported Staphylococcus spp. predominance in hospital environments, though their studies did not systematically culture Bacillus, often dismissed as non-pathogenic environmental contaminants.
Bacillus cereus group organisms cause catheter-associated bloodstream infections, pneumonia, and wound infections in neutropenic patients with case fatality rates approaching 20-30% 20. Our recovery of Bacillus from 34.5% of isolates across diverse surfaces including mattresses, bed rails, and infusion poles suggests widespread environmental colonization requiring enhanced cleaning protocols and potential consideration in empirical antimicrobial regimens.
The substantial recovery of Pseudomonas aeruginosa (20.7% of isolates) exclusively from water-associated sites (sinks, oxygen humidifiers) corroborates extensive literature documenting hospital plumbing systems as persistent Pseudomonas reservoirs 21. This Gram-negative opportunist demonstrates remarkable adaptability to oligotrophic aquatic environments, forming robust biofilms within drain pipes and faucet aerators that continuously seed the healthcare environment 22. Several nosocomial Pseudomonas outbreaks in oncology and transplant units have been traced to contaminated water sources, with whole-genome sequencing confirming patient isolates matched drain genotypes 23.
The detection of methicillin-resistant coagulase-negative staphylococci (MR-CoNS) exhibiting the classic KTG (kanamycin-tobramycin-gentamicin) co-resistance phenotype represents a concerning finding with important clinical and epidemiological implications. This resistance constellation, mediated by mecA gene-encoded altered penicillin-binding protein 2a (PBP2a) for methicillin resistance and aminoglycoside-modifying enzymes for KTG resistance, typifies healthcare-adapted staphylococcal clones that emerge under intense antimicrobial selection pressure 24.
While CoNS are traditionally regarded as low-virulence commensals, they represent leading causes of catheter-related bloodstream infections, particularly in patients with long-term central venous access devices ubiquitous in chemotherapy administration 25. The environmental detection of MR-CoNS on a privacy curtain in the shared infusion bay, a high-touch surface contacted by multiple healthcare workers between patient encounters, suggests healthcare worker hands as probable transmission vectors.
This finding mirrors results from Meité et al. 13 who documented high methicillin resistance prevalence in environmental Staphylococcus isolates from Ivorian intensive care units, suggesting endemic circulation of resistant staphylococcal clones in West African healthcare facilities. The single S. aureus isolate demonstrated susceptibility to all agents except erythromycin, a more favorable profile than reported from many settings.
The recovery of ESBL-producing E. coli and E. cloacae (40% ESBL prevalence among Enterobacteriaceae isolates) from patient room and treatment area sinks represents a critical infection control concern. ESBL-producing Enterobacteriaceae have emerged as dominant nosocomial pathogens globally, causing healthcare-associated urinary tract infections, bloodstream infections, and pneumonia with increased mortality compared to susceptible strains 26.
Hospital wastewater systems serve as ecological niches where ESBL-producing bacteria persist despite antimicrobial exposure, with drain biofilms harboring concentrations exceeding 10⁶ CFU/mL 27. Retrograde splashing during handwashing, aerosolization during sink use, and inadequate hand hygiene after sink contact facilitate transmission from drains to patient care zones. Several documented outbreaks in hematology-oncology units have been terminated only after complete drain removal and replacement 28.
This multidrug-resistant phenotype, often plasmid-mediated and horizontally transferable, severely constrains empirical therapy options for suspected Gram-negative infections. The preservation of carbapenem susceptibility across all Enterobacteriaceae isolates represents an encouraging finding, suggesting carbapenemase-producing organisms have not yet become established in this environment, though continued surveillance remains essential.
Most clinical microbiology laboratories dismiss Bacillus as culture contaminants, particularly when isolated from non-sterile sites like environmental surfaces. However, several factors support their clinical relevance in this chemotherapy setting: ubiquitous recovery across multiple sites and sampling occasions argues against random contamination, their documented capacity to cause invasive infection in neutropenic hosts, and their intrinsic resistance to empirical antibiotics commonly used for febrile neutropenia (β-lactams) creates opportunities for breakthrough infection.
Environmental Bacillus control presents unique challenges given spore resistance to standard disinfectants. Quaternary ammonium compounds and alcohol-based products demonstrate minimal sporicidal activity, while hypochlorite solutions at appropriate concentrations remain the most effective environmental control measure 29.
Several methodological factors warrant acknowledgment when interpreting our findings. The choice of swab-based surface sampling, while practical and widely used, demonstrates reduced sensitivity for Gram-positive cocci compared to contact agar plates, potentially underestimating staphylococcal contamination 22. Conversely, moistened swabs may enhance Gram-negative bacilli recovery, possibly inflating Pseudomonas and Enterobacteriaceae detection. Future surveillance incorporating both methodologies would provide more comprehensive environmental characterization.
The single cross-sectional survey design limits our ability to assess temporal contamination dynamics, identify persistent versus transient organisms, or evaluate seasonal variations potentially relevant in tropical settings. Longitudinal surveillance tracking contamination patterns before and after cleaning, across day and night shifts, would strengthen understanding of environmental microbiology in this setting.
Sample size constraints, particularly the limited Enterobacteriaceae recovery (n=5), reduce statistical power for resistance prevalence estimation and preclude multivariable analysis of contamination risk factors. Nevertheless, even this modest surveillance revealed clinically significant resistant organisms (ESBL-producers, MR-CoNS) warranting intervention.
The absence of molecular characterization limits our ability to determine whether resistant isolates represent clonal expansion of single strains versus polyclonal diversity, distinguish hospital-adapted versus community-acquired organisms, or identify specific resistance genes. Future studies incorporating genomic epidemiology would illuminate transmission dynamics and inform targeted interventions.
This inaugural environmental surveillance study from a West African chemotherapy unit reveals substantial bacterial contamination with opportunistic pathogens demonstrating concerning resistance patterns including ESBL production, methicillin resistance, and intermediate susceptibility to last-line agents. The predominance of Bacillus spp., often dismissed as contaminants but capable of causing invasive infection in immunocompromised hosts, highlights taxonomic patterns potentially unique to tropical healthcare settings. Water sources emerge as critical reservoirs for Pseudomonas aeruginosa and ESBL-producing Enterobacteriaceae, warranting targeted engineering and disinfection interventions.
These baseline data establish the foundation for evidence-based infection prevention programs protecting vulnerable cancer patients and provide a framework for expanded surveillance across African oncology centers. Future research should incorporate longitudinal sampling designs, molecular epidemiology to elucidate transmission dynamics, and intervention studies assessing the impact of enhanced environmental control measures on contamination reduction and ultimately, healthcare-associated infection rates. As cancer incidence rises across sub-Saharan Africa and chemotherapy access expands, ensuring microbiologically safe care environments represents a fundamental component of comprehensive oncology care delivery.
The authors declare no potential conflicts of interest in the research, writing, and/or publication of this article.
After several readings and corrections of the manuscript, the authors approved the publication of this article.
The authors would like to express their sincere gratitude to the management of the CNRAO and the microbiology teaching unit of the UFR Medical Sciences of Abidjan.
| [1] | World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide. Geneva: WHO; 2011. PDF disponible: https:// apps.who.int/ iris/bitstream/ handle/10665/80135/9789241501507_eng.pdf?sequence=1. | ||
| In article | |||
| [2] | Burden of endemic healthcareassociated infection in developing countries: systematic review and metaanalysis – B Allegranzi et al. Lancet. 2011;377(9761):228-241. PDF: https:// www. thelancet.com/ journals/ lancet/article /PIIS0140-6736(10) 61458-4/fulltext. | ||
| In article | View Article PubMed | ||
| [3] | Donskey CJ. Does improving surface cleaning and disinfection reduce health care–associated infections? Am J Infect Control. 2013; 41(5 Suppl): S12–9. | ||
| In article | View Article PubMed | ||
| [4] | Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect Control Hosp Epidemiol. 2011; 32(7): 687–699. | ||
| In article | View Article PubMed | ||
| [5] | Weber DJ, Anderson D, Rutala WA. The role of the surface environment in healthcare-associated infections. Curr Opin Infect Dis. 2013; 26(4): 338–344. | ||
| In article | View Article PubMed | ||
| [6] | Lax S, Gilbert JA. Hospital-associated microbiota and implications for nosocomial infections. Trends Mol Med. 2015; 21(7): 427–432. | ||
| In article | View Article PubMed | ||
| [7] | Brooks B, Firek BA, Miller CS, Sharon I, Thomas BC, Baker R, Morowitz MJ, Banfield JF. Microbes in the neonatal intensive care unit resemble those found in the gut of premature infants. Microbiome. 2014 Jan 28; 2(1): 1. | ||
| In article | View Article PubMed | ||
| [8] | Taplitz RA, Kennedy EB, Bow EJ, Crews J, Gleason C, Hawley DK, et al. Antimicrobial prophylaxis for adult patients with cancer-related immunosuppression: ASCO and IDSA clinical practice guideline update. J Clin Oncol. 2018; 36(30): 3043–3054. | ||
| In article | View Article PubMed | ||
| [9] | Weber DJ, Rutala WA, Miller MB, Huslage K, Sickbert-Bennett EE. Role of hospital surfaces in the transmission of emerging health care–associated pathogens: norovirus, Clostridium difficile, and Acinetobacter species. Am J Infect Control. 2010; 38(5 Suppl 1): S25–33. | ||
| In article | View Article PubMed | ||
| [10] | Boyce JM. Environmental contamination makes an important contribution to hospital infection. J Hosp Infect. 2007; 65 Suppl 2: 50–54. | ||
| In article | View Article PubMed | ||
| [11] | Irek EO, Amupitan AA, Obadare TO & Aboderin AO. A systematic review of healthcare-associated infections in Africa: An antimicrobial resistance perspective Afr J Lab Med. 2018; 7(2), a796. | ||
| In article | View Article PubMed | ||
| [12] | Founou RC, Founou LL, Essack SY. Clinical and economic impact of antibiotic resistance in developing countries: a systematic review and meta-analysis. PLOS One. 2017; 17(1): 577. | ||
| In article | View Article PubMed | ||
| [13] | Méité S, Boni-Cissé C, Monemo P, Mlantanoa AP, Faye-ketté H, Dosso H. Surveillance microbiologique des surfaces au niveau d’un établissement hospitalier de niveau tertiaire: exemple du CHU de Yopougon (Abidjan,Côte d’Ivoire). J Sci Pharm Biol 2010; 11(1): 73—81 | ||
| In article | |||
| [14] | Samira B, Soraya B, Zahia H. Assessment of hospital environmental bacterial contamination in the western region of Algeria. Asian Pacific Journal of Tropical Disease. 2015; 5(6): 436-440. | ||
| In article | |||
| [15] | Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 2011; 52(4): e56-e93. | ||
| In article | View Article PubMed | ||
| [16] | Napoli C, Marcotrigiano V, Montagna MT. Air sampling procedures to evaluate microbial contamination: a comparison between active and passive methods in operating theatres. BMC Public Health. 2012; 12: 594. | ||
| In article | View Article PubMed | ||
| [17] | Peleg AY, Hooper DC. Hospital-acquired infections due to gram-negative bacteria. N Engl J Med. 2010 May 13; 362(19): 1804-13. | ||
| In article | View Article PubMed | ||
| [18] | Andrianjafy TM, Rasamindrakotroka MT, Henintsoa RN, et al. Bacterial contamination of medical devices and the hospital environment in the intensive care unit at the University Hospital in Antananarivo, Madagascar. Journal of Infection in Developing Countries. 2017; 11(8): 623-628. | ||
| In article | |||
| [19] | Barbosa TM, Serra CR, La Ragione RM, Woodward MJ, Henriques AO. Screening for Bacillus isolates in the broiler gastrointestinal tract. Applied and Environmental Microbiology. 2005; 71(2): 968-978. | ||
| In article | View Article PubMed | ||
| [20] | Bottone EJ. Bacillus cereus, a volatile human pathogen. Clinical Microbiology Reviews. 2010; 23(2): 382-398. | ||
| In article | View Article PubMed | ||
| [21] | Loveday HP, Wilson JA, Kerr K, et al. Association between healthcare water systems and Pseudomonas aeruginosa infections: a rapid systematic review. Journal of Hospital Infection. 2014; 86(1): 7-15. | ||
| In article | View Article PubMed | ||
| [22] | Russotto V, Cortegiani A, Raineri SM, Giarratano A. Bacterial contamination of inanimate surfaces and equipment in the intensive care unit. Journal of Intensive Care. 2015; 3: 54. | ||
| In article | View Article PubMed | ||
| [23] | Kizny Gordon AE, Mathers AJ, Cheong EYL, et al. The hospital water environment as a reservoir for carbapenem-resistant organisms causing hospital-acquired infections—a systematic review of the literature. Clinical Infectious Diseases. 2017; 64(10): 1435-1444. | ||
| In article | View Article PubMed | ||
| [24] | Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clinical Microbiology Reviews. 2014;27(4):870-926. | ||
| In article | View Article PubMed | ||
| [25] | Favre B, Hugonnet S, Correa L, Sax H, Rohner P, Pittet D. Nosocomial bacteremia: clinical significance of a single blood culture positive for coagulase-negative staphylococci. Infection Control and Hospital Epidemiology. 2005; 26(8): 697-702. | ||
| In article | View Article PubMed | ||
| [26] | Schwaber MJ, Carmeli Y. Mortality and delay in effective therapy associated with extended-spectrum β-lactamase production in Enterobacteriaceae bacteraemia: a systematic review and meta-analysis. Journal of Antimicrobial Chemotherapy. 2007; 60(5): 913-920. | ||
| In article | View Article PubMed | ||
| [27] | Kotay S, Chai W, Guilford W, Barry K, Mathers AJ. Spread from the sink to the patient: in situ study using green fluorescent protein (GFP)-expressing Escherichia coli to model bacterial dispersion from hand-washing sink-trap reservoirs. Applied and Environmental Microbiology. 2017; 83(8): e03327-16. | ||
| In article | View Article PubMed | ||
| [28] | Leitner E, Zarfel G, Luxner J, et al. Contaminated handwashing sinks as the source of a clonal outbreak of KPC-2-producing Klebsiella oxytoca on a hematology ward. Antimicrobial Agents and Chemotherapy. 2015; 59(1): 714-716. | ||
| In article | View Article PubMed | ||
| [29] | Li, N., Siddique, A., Liu, N., Teng, L., Ed-Dra, A., Yue, M., & Li, Y. (2025). Global Epidemiology and health risks of Bacillus cereus Infections: Special focus on infant foods. Food research international (Ottawa, Ont.), 201, 115650. | ||
| In article | View Article | ||
Published with license by Science and Education Publishing, Copyright © 2025 Boni Catherine, Yapi Adompo Jaurès Cedric, Méité Syndou, Yapi Ivanne Alexia, Gnegouri Rachelle, Bahan Gninissemet Armel, Koffi Stephane, Kacou-N’douba Adèle and Kouassi-M’bengue Alphonsine
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide. Geneva: WHO; 2011. PDF disponible: https:// apps.who.int/ iris/bitstream/ handle/10665/80135/9789241501507_eng.pdf?sequence=1. | ||
| In article | |||
| [2] | Burden of endemic healthcareassociated infection in developing countries: systematic review and metaanalysis – B Allegranzi et al. Lancet. 2011;377(9761):228-241. PDF: https:// www. thelancet.com/ journals/ lancet/article /PIIS0140-6736(10) 61458-4/fulltext. | ||
| In article | View Article PubMed | ||
| [3] | Donskey CJ. Does improving surface cleaning and disinfection reduce health care–associated infections? Am J Infect Control. 2013; 41(5 Suppl): S12–9. | ||
| In article | View Article PubMed | ||
| [4] | Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect Control Hosp Epidemiol. 2011; 32(7): 687–699. | ||
| In article | View Article PubMed | ||
| [5] | Weber DJ, Anderson D, Rutala WA. The role of the surface environment in healthcare-associated infections. Curr Opin Infect Dis. 2013; 26(4): 338–344. | ||
| In article | View Article PubMed | ||
| [6] | Lax S, Gilbert JA. Hospital-associated microbiota and implications for nosocomial infections. Trends Mol Med. 2015; 21(7): 427–432. | ||
| In article | View Article PubMed | ||
| [7] | Brooks B, Firek BA, Miller CS, Sharon I, Thomas BC, Baker R, Morowitz MJ, Banfield JF. Microbes in the neonatal intensive care unit resemble those found in the gut of premature infants. Microbiome. 2014 Jan 28; 2(1): 1. | ||
| In article | View Article PubMed | ||
| [8] | Taplitz RA, Kennedy EB, Bow EJ, Crews J, Gleason C, Hawley DK, et al. Antimicrobial prophylaxis for adult patients with cancer-related immunosuppression: ASCO and IDSA clinical practice guideline update. J Clin Oncol. 2018; 36(30): 3043–3054. | ||
| In article | View Article PubMed | ||
| [9] | Weber DJ, Rutala WA, Miller MB, Huslage K, Sickbert-Bennett EE. Role of hospital surfaces in the transmission of emerging health care–associated pathogens: norovirus, Clostridium difficile, and Acinetobacter species. Am J Infect Control. 2010; 38(5 Suppl 1): S25–33. | ||
| In article | View Article PubMed | ||
| [10] | Boyce JM. Environmental contamination makes an important contribution to hospital infection. J Hosp Infect. 2007; 65 Suppl 2: 50–54. | ||
| In article | View Article PubMed | ||
| [11] | Irek EO, Amupitan AA, Obadare TO & Aboderin AO. A systematic review of healthcare-associated infections in Africa: An antimicrobial resistance perspective Afr J Lab Med. 2018; 7(2), a796. | ||
| In article | View Article PubMed | ||
| [12] | Founou RC, Founou LL, Essack SY. Clinical and economic impact of antibiotic resistance in developing countries: a systematic review and meta-analysis. PLOS One. 2017; 17(1): 577. | ||
| In article | View Article PubMed | ||
| [13] | Méité S, Boni-Cissé C, Monemo P, Mlantanoa AP, Faye-ketté H, Dosso H. Surveillance microbiologique des surfaces au niveau d’un établissement hospitalier de niveau tertiaire: exemple du CHU de Yopougon (Abidjan,Côte d’Ivoire). J Sci Pharm Biol 2010; 11(1): 73—81 | ||
| In article | |||
| [14] | Samira B, Soraya B, Zahia H. Assessment of hospital environmental bacterial contamination in the western region of Algeria. Asian Pacific Journal of Tropical Disease. 2015; 5(6): 436-440. | ||
| In article | |||
| [15] | Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 2011; 52(4): e56-e93. | ||
| In article | View Article PubMed | ||
| [16] | Napoli C, Marcotrigiano V, Montagna MT. Air sampling procedures to evaluate microbial contamination: a comparison between active and passive methods in operating theatres. BMC Public Health. 2012; 12: 594. | ||
| In article | View Article PubMed | ||
| [17] | Peleg AY, Hooper DC. Hospital-acquired infections due to gram-negative bacteria. N Engl J Med. 2010 May 13; 362(19): 1804-13. | ||
| In article | View Article PubMed | ||
| [18] | Andrianjafy TM, Rasamindrakotroka MT, Henintsoa RN, et al. Bacterial contamination of medical devices and the hospital environment in the intensive care unit at the University Hospital in Antananarivo, Madagascar. Journal of Infection in Developing Countries. 2017; 11(8): 623-628. | ||
| In article | |||
| [19] | Barbosa TM, Serra CR, La Ragione RM, Woodward MJ, Henriques AO. Screening for Bacillus isolates in the broiler gastrointestinal tract. Applied and Environmental Microbiology. 2005; 71(2): 968-978. | ||
| In article | View Article PubMed | ||
| [20] | Bottone EJ. Bacillus cereus, a volatile human pathogen. Clinical Microbiology Reviews. 2010; 23(2): 382-398. | ||
| In article | View Article PubMed | ||
| [21] | Loveday HP, Wilson JA, Kerr K, et al. Association between healthcare water systems and Pseudomonas aeruginosa infections: a rapid systematic review. Journal of Hospital Infection. 2014; 86(1): 7-15. | ||
| In article | View Article PubMed | ||
| [22] | Russotto V, Cortegiani A, Raineri SM, Giarratano A. Bacterial contamination of inanimate surfaces and equipment in the intensive care unit. Journal of Intensive Care. 2015; 3: 54. | ||
| In article | View Article PubMed | ||
| [23] | Kizny Gordon AE, Mathers AJ, Cheong EYL, et al. The hospital water environment as a reservoir for carbapenem-resistant organisms causing hospital-acquired infections—a systematic review of the literature. Clinical Infectious Diseases. 2017; 64(10): 1435-1444. | ||
| In article | View Article PubMed | ||
| [24] | Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clinical Microbiology Reviews. 2014;27(4):870-926. | ||
| In article | View Article PubMed | ||
| [25] | Favre B, Hugonnet S, Correa L, Sax H, Rohner P, Pittet D. Nosocomial bacteremia: clinical significance of a single blood culture positive for coagulase-negative staphylococci. Infection Control and Hospital Epidemiology. 2005; 26(8): 697-702. | ||
| In article | View Article PubMed | ||
| [26] | Schwaber MJ, Carmeli Y. Mortality and delay in effective therapy associated with extended-spectrum β-lactamase production in Enterobacteriaceae bacteraemia: a systematic review and meta-analysis. Journal of Antimicrobial Chemotherapy. 2007; 60(5): 913-920. | ||
| In article | View Article PubMed | ||
| [27] | Kotay S, Chai W, Guilford W, Barry K, Mathers AJ. Spread from the sink to the patient: in situ study using green fluorescent protein (GFP)-expressing Escherichia coli to model bacterial dispersion from hand-washing sink-trap reservoirs. Applied and Environmental Microbiology. 2017; 83(8): e03327-16. | ||
| In article | View Article PubMed | ||
| [28] | Leitner E, Zarfel G, Luxner J, et al. Contaminated handwashing sinks as the source of a clonal outbreak of KPC-2-producing Klebsiella oxytoca on a hematology ward. Antimicrobial Agents and Chemotherapy. 2015; 59(1): 714-716. | ||
| In article | View Article PubMed | ||
| [29] | Li, N., Siddique, A., Liu, N., Teng, L., Ed-Dra, A., Yue, M., & Li, Y. (2025). Global Epidemiology and health risks of Bacillus cereus Infections: Special focus on infant foods. Food research international (Ottawa, Ont.), 201, 115650. | ||
| In article | View Article | ||



{kind=link}