Coronary embolism is a non-atherosclerotic cause of acute coronary syndromes. It is frequently observed in patients with atrial fibrillation or prosthetic heart valves. We report the case of a 40-year-old woman with no cardiovascular risk factors but a history of mechanical mitral valve replacement, who had discontinued her vitamin K antagonist (VKA) therapy without medical supervision. She presented with sudden-onset, typical anginal chest pain at rest, described as retrosternal pressure radiating to the left arm and associated with dyspnea. Transthoracic echocardiography revealed an abnormality on the mitral prosthesis, and transesophageal echocardiography confirmed the presence of a thrombus. Coronary angiography identified a subocclusive thrombotic lesion in the mid-left anterior descending (LAD) artery, consistent with coronary embolism. The patient underwent successful manual thrombectomy without stent implantation.
Acute coronary syndrome (ACS) is most commonly caused by atherosclerotic plaque rupture, which can lead to myocardial ischemia. However, non-atherosclerotic causes such as coronary embolism, though rare, should not be overlooked — particularly in patients with low cardiovascular risk profiles. Coronary embolism is an underrecognized cause of ACS, accounting for approximately 2.9% to 4.0% of cases in angiographic and autopsy series 1. It can present with the same clinical and electrocardiographic features as classic atherothrombotic myocardial infarction, making diagnosis particularly challenging 2, 3.
Atrial fibrillation, endocarditis, intracardiac thrombi, and the presence of mechanical prosthetic valves are conditions that predispose to coronary embolism. In patients with prosthetic heart valves, continuous anticoagulation is essential to prevent thromboembolic events. Poor adherence to anticoagulation therapy significantly increases the risk of coronary embolism.
Although rare, coronary embolism is associated with significant morbidity and a potentially severe prognosis, particularly in the absence of prompt diagnosis and management. Delayed recognition may result in larger infarcts, mechanical complications, or sudden cardiac death.
We report the case of a 40-year-old woman with a history of mechanical mitral valve replacement who had discontinued anticoagulation therapy for over three years. She presented with sudden-onset typical anginal chest pain at rest and was diagnosed with an acute coronary syndrome. Coronary angiography revealed a thrombotic occlusion of a coronary artery, that was successfully treated with manual thrombectomy. A diagnosis of coronary embolism was established.
A 40-year-old woman with a history of mechanical mitral valve replacement for rheumatic mitral stenosis and concomitant tricuspid valve plasty performed nine years earlier was admitted for the management of acute chest pain at rest. The pain had started suddenly five hours before admission. It was described as severe, constrictive retrosternal discomfort radiating to the left arm, and was associated with dyspnea and sweating. The pain was continuous and not relieved by rest. Notably, the patient had discontinued her vitamin K antagonist (VKA) therapy three years earlier due to heavy menstrual bleeding. No medical consultation had been sought at the time, and she was not taking any other medications.
On examination, she was hemodynamically stable. Cardiac auscultation revealed an irregular rhythm and an audible mechanical valve click. The electrocardiogram (ECG) showed atrial fibrillation at 95 beats per minute, with negative T waves in the septal, lateral, and inferior leads. According to the patient, her atrial fibrillation had preceded the surgery, likely as a complication of rheumatic mitral stenosis and left atrial enlargement.
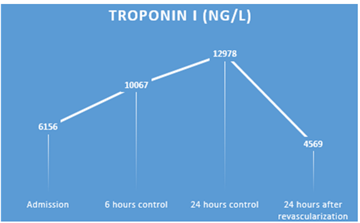
Troponin levels were elevated to 400 times the normal value, with the rest of the laboratory results being normal (Table 1).
Given the clinical presentation suggestive of acute coronary syndrome (ACS), the patient was managed according to standard protocols. She received a loading dose of aspirin and clopidogrel. Serial troponin measurements were performed throughout her hospitalization. (Figure 1).
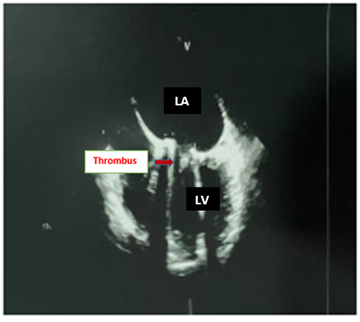
Transthoracic echocardiography demonstrated left ventricular dilatation with apical akinesia and a moderately reduced ejection fraction estimated at 39%. Dysfunction of the mechanical mitral valve was suspected. Both atria were dilated, whereas the right ventricle exhibited normal dimensions and preserved systolic function. Transesophageal echocardiography identified a mobile echogenic mass attached to the ventricular side of the mitral prosthesis, highly suggestive of a thrombus (Figure 2).
Coronary angiography revealed a subocclusive thrombotic lesion in the mid-left anterior descending (LAD) artery, with preserved distal flow, suggestive of coronary embolism (Figure 3).
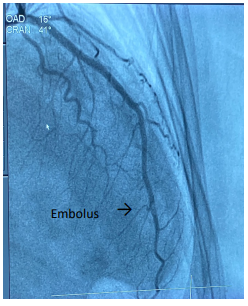
The remainder of the coronary tree appeared angiographically normal. A manual thrombectomy was performed in the LAD, resulting in successful thrombus extraction and restoration of normal coronary flow, along with the administration of a GPIIb/IIIa receptor inhibitor. No stent was implanted, as no underlying atherosclerotic lesion was identified. Anticoagulation therapy with a vitamin K antagonist (VKA) was reinstated, accompanied by thorough patient education and regular INR monitoring.
Embolic phenomena in the coronary circulation are rare under normal physiological conditions due to the protective anatomy of the coronary arteries and the shielding effect of the aortic valve cusps during systole. However, the risk of coronary embolism increases significantly in patients with atrial fibrillation, prosthetic heart valves, infective endocarditis 4, or hypercoagulable states. In such cases, ineffective anticoagulation with International Normalized Ratio (INR) levels outside the therapeutic range or discontinuation of vitamin K antagonists (VKAs) may predispose to thrombus formation. Our patient presented a high thrombotic risk due to the presence of a mechanical mitral valve, atrial fibrillation, and a history of anticoagulation discontinuation. Clinically, coronary embolism typically presents as an acute coronary syndrome in patients with low cardiovascular risk but known thrombotic risk factors. Biologically, a marked elevation in cardiac biomarkers is often observed. However, electrocardiography (ECG) and transthoracic echocardiography (TTE) generally do not allow differentiation between coronary embolism and atherosclerotic acute coronary syndrome.
Transesophageal echocardiography (TEE) remains the key diagnostic tool, allowing detailed visualization of the heart valves and detection of intracardiac thrombi. Cardiac catheterization may reveal atypical findings, such as occlusion of one or more coronary vessels in the absence of underlying atherosclerosis — specifically, no evidence of unstable plaques, dissections, or mural thrombi.
To date, no established treatment guidelines exist 5. In our patient’s case, thrombectomy was carefully performed. Coronary thrombectomies are infrequently performed due to the technical expertise required and the significant risk of complications associated with the procedure. Common complications include coronary dissection, failure in cases of adherent thrombus with a no-reflow phenomenon, systemic embolism, and thrombus migration 6. The addition of a glycoprotein IIb/IIIa receptor inhibitor is often indicated 7 to enhance thrombectomy effectiveness.
Another key consideration in managing these patients is whether or not to place a stent 8. In cases of failure or partial success, balloon angioplasty combined with stent placement, alongside anticoagulant and antiplatelet therapy, can be beneficial 9.
In our patient’s case, no stent was implanted, as the coronary vessels appeared smooth and showed no signs of atherosclerosis. Furthermore, distal flow beyond the lesion was preserved (TIMI III). Stent implantation would have necessitated lifelong anticoagulation, which posed a significant risk given the patient’s history of treatment interruption.
Maintaining effective anticoagulation therapy is essential to prevent embolic events, especially in patients with atrial fibrillation 10. In our patient’s case, direct oral anticoagulant (DOAC) therapy was proposed due to its proven efficacy and ease of management compared to vitamin K antagonists (VKAs) 11, but the treatment was declined by the patient because of financial constraints. Recent studies and meta-analyses 12 have demonstrated that DOACs are as effective as VKAs in preventing thromboembolic events in patients with atrial fibrillation secondary to valvular heart disease, while offering a comparable or improved safety profile—particularly with a lower risk of intracranial hemorrhage—and greater ease of use.
Coronary embolism should be suspected in any case of acute coronary syndrome occurring in a patient with low cardiovascular risk but a high thrombotic risk . Accurate diagnosis relies on integrating the clinical context with advanced imaging modalities, such as transesophageal echocardiography, which can identify intracardiac sources of emboli, and coronary angiography, which remains the gold standard for definitive confirmation. The management of coronary embolism must be carefully individualized, taking into account the patient’s coronary anatomy and the angiographic features of the culprit lesion.
| [1] | Shibata T, Kawakami S, Noguchi T, et al. Prevalence, clinical features, and prognosis of acute myocardial infarction attributable to coronary artery embolism. Circulation. 2015; 132(4): 241–250. | ||
| In article | View Article PubMed | ||
| [2] | Karakoyun S, Gürsoy MO, Kalçık M, Yesin M, Özkan M. A case series of prosthetic heart valve thrombosis-derived coronary embolism. Turk Kardiyol Dern Ars. 2014 Jul;42(5):467-71. | ||
| In article | View Article PubMed | ||
| [3] | Lacey MJ, Raza S, Rehman H, Puri R, Bhatt DL, Kalra A. Coronary Embolism: A Systematic Review. Cardiovasc Revasc Med. 2020 Mar; 21(3): 367-374. | ||
| In article | View Article PubMed | ||
| [4] | Garvey GJ, Neu HC. Infective endocarditis—An evolving disease: A review of endocarditis at the Columbia-Presbyterian medical center, vol. 57; 1978; 1968–73 Medicine (Baltimore). | ||
| In article | View Article PubMed | ||
| [5] | Budavari AI, Glenn TJ, Will KK, Askew JW, Fortuin FD. A case of simultaneous pulmonary embolism and acute myocardial infarction secondary to a previously undiagnosed patent foramen ovale. J Hosp Med United States 2009; 4: E5–9. | ||
| In article | View Article PubMed | ||
| [6] | Hernandez F, Pombo M, Dalmau R, Andreu J, Alonso M, Albarran A, et al. Acute coronary embolism: angiographic diagnosis and treatment with primary angioplasty. Catheter Cardiovasc Interv United States 2002; 55 :491–4. | ||
| In article | View Article PubMed | ||
| [7] | Adnan G, Singh DP, Mahajan K. Coronary Artery Thrombus. [Updated 2022 Oct 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. | ||
| In article | |||
| [8] | Kotooka N, Otsuka Y, Yasuda S, Morii I, Kawamura A, Miyazaki S. Three cases of acute myocardial infarction due to coronary embolism: treatment using a thrombus aspiration device. Jpn Heart J Japan 2004; 45: 861–6. | ||
| In article | View Article PubMed | ||
| [9] | Giri S, Hwang I, Alsafwah S. A case of left main coronary artery embolus further embolising to the left anterior descending artery. BMJ Case Rep England 2014; 2014. | ||
| In article | View Article PubMed | ||
| [10] | Acikel S, Dogan M, Aksoy MMN, Akdemir R. Coronary embolism causing non-ST elevation myocardial infarction in a patient with paroxysmal atrial fibrillation: treatment with thrombus aspiration catheter. Int J Cardiol Netherlands 2011:e33–5. | ||
| In article | View Article PubMed | ||
| [11] | Yokoyama Y, Briasoulis A, Ueyama H, Mori M, Iwagami M, Misumida N, Takagi H, Kuno T. Direct oral anticoagulants versus vitamin K antagonists in patients with atrial fibrillation and bioprosthetic valves: A meta-analysis. J Thorac Cardiovasc Surg. 2023 Jun; 165(6): 2052-2059. e4. | ||
| In article | View Article PubMed | ||
| [12] | de Souza Lima Bitar Y, Neto MG, Filho JAL, Pereira LV, Travassos KSO, Akrami KM, Roever L, Duraes AR. Comparison of the New Oral Anticoagulants and Warfarin in Patients with Atrial Fibrillation and Valvular Heart Disease: Systematic Review and Meta-Analysis. Drugs R D. 2019 Jun; 19(2): 117-126. | ||
| In article | |||
Published with license by Science and Education Publishing, Copyright © 2025 Laoufi Zaynab, Lokman Hafsa, Benyass Aatif, Mouine Najat and Lakhal Zouhair
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Shibata T, Kawakami S, Noguchi T, et al. Prevalence, clinical features, and prognosis of acute myocardial infarction attributable to coronary artery embolism. Circulation. 2015; 132(4): 241–250. | ||
| In article | View Article PubMed | ||
| [2] | Karakoyun S, Gürsoy MO, Kalçık M, Yesin M, Özkan M. A case series of prosthetic heart valve thrombosis-derived coronary embolism. Turk Kardiyol Dern Ars. 2014 Jul;42(5):467-71. | ||
| In article | View Article PubMed | ||
| [3] | Lacey MJ, Raza S, Rehman H, Puri R, Bhatt DL, Kalra A. Coronary Embolism: A Systematic Review. Cardiovasc Revasc Med. 2020 Mar; 21(3): 367-374. | ||
| In article | View Article PubMed | ||
| [4] | Garvey GJ, Neu HC. Infective endocarditis—An evolving disease: A review of endocarditis at the Columbia-Presbyterian medical center, vol. 57; 1978; 1968–73 Medicine (Baltimore). | ||
| In article | View Article PubMed | ||
| [5] | Budavari AI, Glenn TJ, Will KK, Askew JW, Fortuin FD. A case of simultaneous pulmonary embolism and acute myocardial infarction secondary to a previously undiagnosed patent foramen ovale. J Hosp Med United States 2009; 4: E5–9. | ||
| In article | View Article PubMed | ||
| [6] | Hernandez F, Pombo M, Dalmau R, Andreu J, Alonso M, Albarran A, et al. Acute coronary embolism: angiographic diagnosis and treatment with primary angioplasty. Catheter Cardiovasc Interv United States 2002; 55 :491–4. | ||
| In article | View Article PubMed | ||
| [7] | Adnan G, Singh DP, Mahajan K. Coronary Artery Thrombus. [Updated 2022 Oct 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. | ||
| In article | |||
| [8] | Kotooka N, Otsuka Y, Yasuda S, Morii I, Kawamura A, Miyazaki S. Three cases of acute myocardial infarction due to coronary embolism: treatment using a thrombus aspiration device. Jpn Heart J Japan 2004; 45: 861–6. | ||
| In article | View Article PubMed | ||
| [9] | Giri S, Hwang I, Alsafwah S. A case of left main coronary artery embolus further embolising to the left anterior descending artery. BMJ Case Rep England 2014; 2014. | ||
| In article | View Article PubMed | ||
| [10] | Acikel S, Dogan M, Aksoy MMN, Akdemir R. Coronary embolism causing non-ST elevation myocardial infarction in a patient with paroxysmal atrial fibrillation: treatment with thrombus aspiration catheter. Int J Cardiol Netherlands 2011:e33–5. | ||
| In article | View Article PubMed | ||
| [11] | Yokoyama Y, Briasoulis A, Ueyama H, Mori M, Iwagami M, Misumida N, Takagi H, Kuno T. Direct oral anticoagulants versus vitamin K antagonists in patients with atrial fibrillation and bioprosthetic valves: A meta-analysis. J Thorac Cardiovasc Surg. 2023 Jun; 165(6): 2052-2059. e4. | ||
| In article | View Article PubMed | ||
| [12] | de Souza Lima Bitar Y, Neto MG, Filho JAL, Pereira LV, Travassos KSO, Akrami KM, Roever L, Duraes AR. Comparison of the New Oral Anticoagulants and Warfarin in Patients with Atrial Fibrillation and Valvular Heart Disease: Systematic Review and Meta-Analysis. Drugs R D. 2019 Jun; 19(2): 117-126. | ||
| In article | |||




{kind=link}
{kind=link}
{kind=link}