Blastomycosis is a systemic fungal infection known to be endemic in North America, particularly in the Midwest, Central, and Southeastern United States, as well as Great Lakes, Ohio, and Mississippi River Valleys. It is frequently caused by thermal dimorphic fungi, Blastomyces dermatitidis or Blastomyces gilchristii that exist as mold in the environment and transform to yeast in tissues. The infection typically begins in the lungs as the fungal spores or conidia are inhaled from the environment resulting in pulmonary symptoms. Here, we present an atypical form of disseminated blastomycosis in which the patient initially developed cutaneous manifestations followed by pulmonary and liver involvement. The atypical sequence of symptom onset diverges from the classic presentation where pulmonary disease usually precedes extrapulmonary dissemination. He was initially misdiagnosed with multiple rounds of antibiotics and steroids prior to presentation to our facility. This case highlights the importance of considering disseminated fungal infection in the differential diagnosis of cutaneous lesions especially in patients with exposure to endemic regions. Early recognition is crucial for timely diagnosis and management.
Blastomycosis is an infection caused by the dimorphic fungus Blastomyces. It is known to be endemic to North America - most commonly in the Midwest, Central, and Southeastern United States, Great Lakes, Ohio and Mississippi River Valleys 1. In the United States, blastomycosis is most frequently caused by Blastomyces dermatitidis or Blastomyces gilchristii 2. These organisms are dimorphic in that they grow as mold at less than 30°C (86℉) and as yeast at greater than 33°C (91.4℉) 3. The infection typically begins in the lungs after the conidia are inhaled from the environment resulting in pulmonary disease 1, 4. In the lungs, the organism exists as a yeast causing localized infection. The clinical presentation of pulmonary blastomycosis can vary from a subclinical infection with no symptoms to pneumonia complicated by acute respiratory distress syndrome (ARDS) 1, 4. It can then spread hematogenously to other areas such as the skin, bone, and central nervous system 3. Extrapulmonary involvement takes place in about 25 to 30% of patients with skin being the most common site 4.
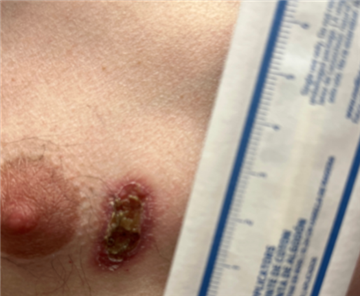
A 49 year old male with a past medical history of seizure disorder presented to the clinic with complaints of ulcerating skin lesions that started 2 to 3 months ago and became worse in the past few weeks. He was initially seen at an outside facility for symptoms, where they performed an incision and drainage along with culture of the left cheek lesion. This returned positive for Staphylococcus aureus and Escherichia coli. He was prescribed a course of Cephalexin and Trimethoprim-Sulfamethoxazole with presumed diagnosis being abscess versus cellulitis. Despite antibiotics, he had no resolution of symptoms. He was then evaluated again in the Emergency Department and was started on Mupirocin ointment, Doxycycline and Prednisone. This also failed to improve his symptoms, so he presented a week later to our clinic. The patient noted that initially the lesion was just on the left cheek. But over the last three weeks, he observed new lesions on his left ear, left arm, and right chest. He worked in a tractor supply store for a living with regular chicken exposure. Prior work history included construction work with insulation, roofing, and framing. He denied any recent travel, camping or spelunking, sick contacts, or new pets/exotic animal exposure. The patient lives in Indiana.
The patient was referred to a dermatologist who performed a punch biopsy of the right chest lesion. Biopsy of the chest lesion was remarkable for ulcerated suppurative granulomatous inflammation with multiple yeast structures including some with broad based budding. The patient was also seen by an Infectious Disease specialist. He reported having intermittent sharp pain to the lesions, pruritus, along with occasional dry cough and night sweat that was not present on initial clinic visit two weeks ago. Considering his cutaneous lesions, lung imaging findings, elevated liver function tests, and positive urine antigen, he was diagnosed with disseminated blastomycosis. He was started on a loading dose of Itraconazole with a plan to continue medication for six months. On follow up, the patient was noted to have improved cutaneous lesions and is being followed closed by the Infectious Diseases specialist.



Pulmonary involvement in blastomycosis presents across a broad clinical spectrum, ranging from asymptomatic infection and flu-like symptoms to acute or chronic pneumonia, which may progress to respiratory failure and acute respiratory distress syndrome (ARDS) 1. Chest imaging findings in blastomycosis are non-specific and often indistinguishable from other pulmonary infections 1. The most reported radiographic finding is lobar consolidation 1. Additional imaging features may include pulmonary masses, interstitial infiltrates, and nodules, with a noted predominance in the upper lobes 1, 5. Extrapulmonary dissemination typically follows chronic pulmonary infection and most frequently involves the skin, bones, central nervous system, and prostate. Cutaneous involvement is the most common extrapulmonary manifestation and usually results from hematogenous spread rather than direct inoculation. The characteristic skin lesion is verrucous in appearance described as elevated, clearly defined, with surface crusting, and may clinically mimic squamous cell carcinoma. Other cutaneous presentations include diffuse pustular lesions and subcutaneous masses.
Our patient presented atypically with skin lesions without pulmonary symptoms. On further evaluation, he was found to have lung abnormalities on chest imaging suggesting he had disseminated disease with silent pulmonary infection. The history, physical examination, and clinical presentation lay the foundation for diagnosis of blastomycosis 6. A detailed history regarding occupational and leisure activities can aid in the diagnosis of blastomycosis. Occupational activities such as work in construction, a microbiology laboratory, or in the veterinary field are typically associated with Blastomycosis 1. Leisure activities such as hiking, fishing at riverbanks, canoeing, beaver dam exploration, and utilization of community compost piles are often noted in patients with Blastomycosis 1. Our patient was inherently at risk due to residing in the Midwest region of the United States. That risk was likely further increased by his prior construction work during which he could have developed the initial infection. Otherwise, he had no known high risk exposures.
Once the clinical suspicion is present, a multimodal approach is done for diagnosis. In patients with pulmonary disease, sputum culture has a diagnostic yield of around 75% but growth is slow requiring up to five weeks of incubation. Non-culture testing such as antigen testing via enzyme immunoassay and serologic testing with immunodiffusion and complement fixation have a rapid turn-around time of a few days in comparison to culture and biopsy results. Urine antigen is the test of choice with a sensitivity of 75 to 90% 6. The antigen assay is known to cross react with other dimorphic fungi such as Histoplasma capsulatum, Paraccoccidiodes, and Talaromyces marneffei 1. The cross reaction phenomenon is due to the similarity of the galactofuranose side chains in galactomannan present in varying fungal organisms 1. This decreases the specificity of the assay to a range of 76.9% to 79%. Serologic testing has a poor sensitivity (<40%) and can be even less reliable in localized disease. Serum β-(1,3)-glucan test (Fungitell) is unreliable for diagnosis as very little of it comprises the Blastomyces yeast cell wall 1.
Staining of the clinical samples is the fastest and least utilized method in identifying Blastomyces yeast with a sensitivity of 50% to 90% for respiratory secretions. In patients with disseminated blastomycosis, histopathologic evaluation of the site of extrapulmonary involvement is crucial and aids in diagnosis 6. The classic finding of blastomycosis in fungal stains is the presence of “broad-based budding yeast (8-20 µm) with a doubly refractile cell wall” 1. The sensitivity of testing can be lower in immunocompetent patients or when there is a smaller burden of disease present and is highly dependent on the quality of the sample obtained.
The treatment of blastomycosis depends on the site of involvement, severity of the disease, and immune status of the patient 6. Itraconazole is usually the first-line option with a dosage regimen of 200 to 400 mg daily for a median of six months and success rate of about 95%. Fluconazole is noted to be inferior in comparison to Itraconazole with a success rate of 64%> Amphotericin B is typically used in patients with severe pulmonary involvement, severe disseminated blastomycosis with or without central nervous system involvement, and immunosuppressed patients with any form of blastomycosis 6. This is typically the initial form of treatment due to rapid onset of action and better central nervous system penetration. After clinical improvement, Amphotericin is typically de-escalated to Itraconazole. 91% of pregnant patients with blastomycosis typically present in the second or third trimester 1. Amphotericin is the treatment of choice for pregnant patients and is typically given until the mother delivers the baby or until the eradication of the infection 6. Amphotericin is used instead of azoles in this patient population because of harm to fetal development. Our patient did not require Amphotericin B as he was immunocompetent and otherwise hemodynamically stable with mild pulmonary involvement. It is crucial to screen for immunocompromising conditions such as Human Immunodeficiency Virus (HIV) in these patients as they tend to have an increased severity of the disease and the presence of these conditions can change treatment.
Our patient was initially misdiagnosed prior to presentation at out facility with multiple rounds of antibiotics and steroids. This is vital as doctors are typically the first point of contact with presenting complaints and can help avoid the delays in diagnosis associated with blastomycosis. In endemic regions, the diagnosis of blastomycosis is usually more than 1 to 2 months 1. The median duration from presentation to diagnosis varies from 23 to 128 days - resulting in worsening severity and increased risk of mortality due to delays in treatment 7.
Our patient had an atypical presentation of disseminated blastomycosis in which his cutaneous lesions preceded pulmonary and hepatic involvement. Notably, the lung findings on his chest x-ray were atypical and non-specific diverging from the classic imaging findings associated with pulmonary blastomycosis. Clinicians should maintain a high index of suspicion for blastomycosis in immunocompromised patients, patients with respiratory symptoms and known exposure to endemic areas, those with pneumonia that are not responsive to antibiotics, and patients with both pulmonary and atypical dermatologic findings.
| [1] | Gauthier, G., & Klein, B. (2020). Blastomycosis. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases (9th ed., pp. 3177–3188). Elsevier, Inc. | ||
| In article | |||
| [2] | Centers for Disease Control and Prevention. (2024). Clinical overview of Blastomycosis. https:// www.cdc.gov/ blastomycosis/ hcp/clinical-overview/index.html. | ||
| In article | |||
| [3] | Mazi, P. B., Rauseo, A. M., & Spec, A. (2021). Blastomycosis. Infectious Disease Clinics of North America, 35(2), 515–530. | ||
| In article | |||
| [4] | Hashim, S., & Barrios, C. (2020). Disseminated blastomycosis. ID Cases, 21, e00786. | ||
| In article | |||
| [5] | Patel, R. G., Patel, B., Petrini, M. F., Carter, R. R., 3rd, & Griffith, J. (1999). Clinical presentation, radiographic findings, and diagnostic methods of pulmonary blastomycosis: a review of 100 consecutive cases. Southern medical journal, 92(3), 289–295. | ||
| In article | |||
| [6] | Pullen, M. F., Alpern, J. D., & Bahr, N. C. (2022). Blastomycosis-Some Progress but Still Much to Learn. Journal of fungi (Basel, Switzerland), 8(8), 824. | ||
| In article | |||
| [7] | Tekin, A., Pinevich, Y., Herasevich, V., Pickering, B. W., Vergidis, P., Gajic, O., & O'Horo, J. C. (2023). Diagnostic delay in pulmonary blastomycosis: a case series reflecting a referral center experience. Infection, 51(1), 193–201. | ||
| In article | |||
Published with license by Science and Education Publishing, Copyright © 2025 Folake Ishola, Cassandra Daet, Omar Elsheikh and Michelle Solik
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Gauthier, G., & Klein, B. (2020). Blastomycosis. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases (9th ed., pp. 3177–3188). Elsevier, Inc. | ||
| In article | |||
| [2] | Centers for Disease Control and Prevention. (2024). Clinical overview of Blastomycosis. https:// www.cdc.gov/ blastomycosis/ hcp/clinical-overview/index.html. | ||
| In article | |||
| [3] | Mazi, P. B., Rauseo, A. M., & Spec, A. (2021). Blastomycosis. Infectious Disease Clinics of North America, 35(2), 515–530. | ||
| In article | |||
| [4] | Hashim, S., & Barrios, C. (2020). Disseminated blastomycosis. ID Cases, 21, e00786. | ||
| In article | |||
| [5] | Patel, R. G., Patel, B., Petrini, M. F., Carter, R. R., 3rd, & Griffith, J. (1999). Clinical presentation, radiographic findings, and diagnostic methods of pulmonary blastomycosis: a review of 100 consecutive cases. Southern medical journal, 92(3), 289–295. | ||
| In article | |||
| [6] | Pullen, M. F., Alpern, J. D., & Bahr, N. C. (2022). Blastomycosis-Some Progress but Still Much to Learn. Journal of fungi (Basel, Switzerland), 8(8), 824. | ||
| In article | |||
| [7] | Tekin, A., Pinevich, Y., Herasevich, V., Pickering, B. W., Vergidis, P., Gajic, O., & O'Horo, J. C. (2023). Diagnostic delay in pulmonary blastomycosis: a case series reflecting a referral center experience. Infection, 51(1), 193–201. | ||
| In article | |||



{kind=link}
{kind=link}
{kind=link}
{kind=link}