Gout and septic arthritis share similar clinical characteristics, including acute joint pain, swelling, fever, and increased inflammatory markers, which make the diagnosis and differentiation more complicated. This challenge is further exacerbated in patients with chronic kidney disease (CKD), who are at risk for both crystal arthropathy and infections. We present a 73-year-old male with CKD stage 3 who initially presented with monoarthritis and systemic symptoms suggestive of septic arthritis; however, synovial fluid analysis showed monosodium urate crystals and sterile cultures. His history of recurrent gout supported the final diagnosis. Following corticosteroid treatment, the patient had rapid improvement in symptoms. This case highlights the diagnostic difficulties and the essential role of synovial fluid analysis in differentiating gout from septic arthritis in CKD patients, stressing the need for a high index of suspicion and tailored management.
Gout is one of the most common types of inflammatory arthritis, which is caused by the deposition of monosodium urate crystals in synovial tissues 1. It affects around 12.1 million adults in the United States, with a prevalence of 5.1% 1. Despite the high prevalence, gouty arthritis continues to be frequently misdiagnosed and inadequately managed 2. Its clinical presentation can closely mimic infection, particularly septic arthritis, with acute joint pain, swelling, erythema, fever, and elevated inflammatory markers 3 4.
Chronic kidney disease (CKD) patients represent a unique population in gout diagnosis and management because of the weak immune responses in CKD patients and limitations in standard treatment options. CKD is associated with impaired immune responses, which makes patients more susceptible to infections 5. On the other hand, reduced renal clearance of uric acid further contributes to hyperuricemia and increases the risk of gout in this population. Treatment options are also limited, as commonly used medications such as NSAIDs, are generally contraindicated in patients with advanced chronic kidney disease due to nephrotoxic risks, and drugs like colchicine require dose adjustments to avoid toxicity. These factors highlight the complexity of diagnosing and managing gout in CKD patients 6.
In summary, differentiation between these two conditions is essential, since septic arthritis needs immediate antimicrobial and often surgical intervention, while gout requires anti-inflammatory therapy adjusted to renal function 6. This case demonstrates the complexities in diagnosing and managing gout in a CKD patient presenting with monoarthritis and systemic inflammatory response signs.
Our patient is a 73-year-old man with a medical history of chronic kidney disease (CKD) stage 3, coronary artery disease (CAD), heart failure with reduced ejection fraction (HFrEF), atrial fibrillation, and recurrent gout, not on prophylactic therapy. He presented to the emergency department with a three-day history of left knee pain, swelling, and redness. He reported decreased range of motion along with systemic symptoms of fever, chills, nausea, and dizziness. There was no history of trauma.
In the emergency department, he was febrile with a temperature of 100.9°F, hypotensive, and tachycardic. On physical examination, the left knee was warm, swollen, erythematous, and extremely tender, with a severely limited range of motion.
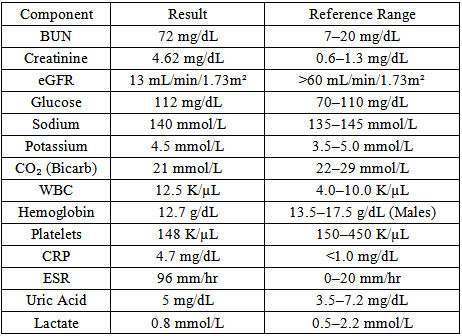
The laboratory workup, as shown in Table 1, demonstrated an elevated white blood cell (WBC) count of 12,500/µL. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were elevated. Uric acid and lactate levels were within normal limits. Renal markers (creatinine and glomerular filtration rate) were above the patient's baseline, indicative of acute-on-chronic kidney disease. Given his tachycardia, fever, and leukocytosis, he met SIRS criteria for sepsis.
A left knee X-ray (Figure 1) and (Figure 2) showed moderate joint effusion, medial compartment osteoarthritis, and chondrocalcinosis. Given the presence of SIRS criteria, physical exam findings, and radiographic joint effusion, there was a high clinical suspicion for septic arthritis. Orthopedics was urgently consulted. A diagnostic arthrocentesis was performed in the ED before initiating antibiotics, yielding 15 mL of cloudy, straw-colored fluid sent for Gram stain, culture, and crystal analysis. Empiric treatment with ceftriaxone and renally dosed vancomycin was initiated, and infectious disease consultation was obtained.


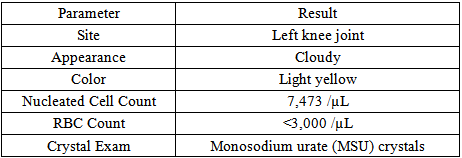
Over the next 48 hours, the patient had no improvement in his symptoms and continued to have intermittent fevers (up to 101°F). Labs showed worsening of his kidney function. Synovial fluid analysis (Table 2) revealed 7,473 nucleated cells/μL and monosodium urate (MSU) crystals. Gram stain and cultures (both synovial fluid and blood) remained negative. Antibiotics were discontinued, and oral prednisone 40 mg once a day was started given the patient’s chronic kidney disease, which limited the use of NSAIDs and colchicine.
The patient’s knee pain, swelling, fever, tachycardia, and leukocytosis improved dramatically within 24 hours of corticosteroid initiation. His kidney function also returned to baseline. He was discharged after four days of admission on oral steroids and referred to rheumatology for initiation of prophylactic therapy.
Gout is one of the most common and prevalent types of inflammatory arthritis 1. It usually presents with monoarticular joint pain, swelling, and erythema. However, there are overlapping characteristics between gout and septic arthritis, as both can present with sudden joint inflammation, fever, leukocytosis, and elevated inflammatory markers such as ESR and CRP, making differentiation difficult in the absence of synovial fluid analysis 3 4 7 8 9 10 11. In patients with chronic kidney disease (CKD), diagnosis becomes even more challenging due to their susceptibility to both gout and infections, which is influenced by reduced uric acid excretion and immune system dysfunction 5.
Synovial fluid analysis remains the gold standard for distinguishing between gout and septic arthritis. Prompt arthrocentesis with fluid analysis is essential. The presence of monosodium urate (MSU) crystals confirms gout; however, it does not rule out a concomitant infection. There are multiple reports of patients presenting with both crystal-induced and septic arthritis, especially in those who are immunocompromised or have CKD 7 8 9 10 11.
Radiographic imaging may reveal nonspecific findings, such as joint effusion or chondrocalcinosis, which do not distinguish between gout and infection. Similarly, serum uric acid level is not reliable, as it is usually within the normal range during an acute flare. Elevated ESR and CRP reflect inflammation but are not specific for differentiating infectious from non-infectious arthritis.
Treatment of acute gout flare-ups mainly involves non-steroidal anti-inflammatory drugs, colchicine, or oral corticosteroids. Managing gout in CKD requires special consideration due to increased risk of renal toxicity, making the treatment options limited, as non-steroidal anti-inflammatory drugs should be avoided, and colchicine poses nephrotoxic risks and requires dose adjustments or avoidance 6. Corticosteroids, administered systemically or intra-articularly, are usually the safest and most effective option in CKD patients 6. Early diagnostic clarity can prevent unnecessary invasive procedures and antibiotic exposure, which could lead to additional renal toxicity risk.
Several published cases reinforce the challenge in diagnosing and distinguishing between gout and infection. Londono et al. presented a case with systemic inflammatory response and multifocal joint involvement, initially thought to be infectious. Infectious workup was negative, and rheumatology consultation led to a diagnosis of polyarticular gout confirmed by arthrocentesis 3. Similarly, Alsinan et al. presented an atypical case of gouty arthritis that mimicked a hand soft tissue infection, initially presumed to be cellulitis with abscess formation. Despite antibiotic therapy, the patient’s symptoms continued until a diagnosis of gout was made after exclusion of infection by negative cultures, demonstrating the diagnostic challenge when gout presents with symptoms closely resembling infection, especially at uncommon sites 4.
Gheit et al. reported a rare and severe case of chronic tophaceous gout complicated by septic arthritis, osteomyelitis, and septic shock, highlighting that chronic tophi can serve as a source of serious infections and discussing the diagnostic difficulty of differentiating gout flares from concurrent joint infections, particularly in elderly patients 7. Tzanis et al. reported two cases of concomitant gout and septic arthritis, emphasizing that the presence of monosodium urate (MSU) crystals does not exclude infection, and that patients with chronic gout are particularly susceptible to joint infections, while infection can also precipitate gout flares 8.
Yu et al. analyzed 30 cases of concomitant septic and gouty arthritis and found that diagnostic confusion is common, with one-third of patients presenting afebrile and some showing normal leukocyte or synovial WBC counts, emphasizing the need for synovial fluid cultures even in atypical presentations 9. Lim, Lu, and Choi conducted a large population-based cohort study using data from the UK Health Improvement Network, demonstrating that patients with incident gout had a significantly increased risk of developing septic arthritis compared to the control group. The adjusted hazard ratio was 2.60 (95% CI 1.93–3.51), more than double the risk in the gout cohort 10.
In a retrospective analysis, Hong et al. examined outcomes of patients who had both septic arthritis and gout. In contrast to patients with septic arthritis alone, their results showed that individuals with both conditions had a much longer hospital stay (an average of 12.6 days) and a higher risk of limb amputation 11. These studies collectively highlight the diagnostic challenge of distinguishing gout from septic arthritis or cellulitis, especially when gout presents at uncommon sites or mimics an infection.
Our case represents a strong example of this diagnostic challenge. Despite his history of chronic kidney disease (CKD) and gout, a gout flare-up was not initially suspected. His clinical presentation and SIRS criteria misled us into initially diagnosing him with septic arthritis and treating him with broad-spectrum antibiotics for two days without significant improvement. However, the negative Gram stain and culture, combined with the history of gout and clinical improvement following corticosteroids, made septic arthritis less likely. This shows that the gout flare-up was diagnosed by exclusion rather than considered as an initial potential diagnosis, along with ruling out serious differential diagnoses like septic arthritis.
In addition to more serious diagnoses, the author of this case report suggests taking a gout flare into consideration initially, given the overlap of the presentation between these two conditions, along with the possibility of the concomitant presence of gout and septic arthritis or one precipitating the other. This shines a light on the need to consider both and perform immediate arthrocentesis, consult specialists when necessary, and tailor the management plan accordingly. These strategies can reduce the length of stay, provide quicker symptom relief, and prevent iatrogenic harm from antibiotics or interventions, as in the case of the patient presented here. We advise aspirating synovial fluid from afflicted joints and analyzing it as soon as possible. This can avoid needless interventions such as lengthy intravenous antibiotics and procedures, which raise the risk of subsequent complications and result in greater use of hospital resources, while also ensuring prompt diagnosis and appropriate treatment.
Furthermore, the author stresses the need for developing a valid diagnostic scoring system to help with the early diagnosis of gout. Prospective clinical trials are also suggested to assess the effectiveness of these tools in real clinical settings, with the ultimate goal of increasing diagnostic accuracy and assisting physicians in more effectively prioritizing differential diagnoses.
Finally, management should follow current guidelines while carefully considering comorbidities such as CKD to avoid harm.
In patients with CKD who present with acute monoarthritis and systemic inflammatory features, clinicians must maintain a high index of suspicion for gout, even when septic arthritis is strongly suspected. Synovial fluid analysis remains the gold standard for an accurate diagnosis. Lastly, understanding gout treatment in CKD patients is essential for achieving the best outcomes and avoiding harm from unnecessary interventions and treatments.
None declared.
None.
| [1] | FitzGerald, J.D., "Gout", Annals of Internal Medicine, 178 (3), ITC33–ITC48, March 2025. | ||
| In article | View Article PubMed | ||
| [2] | Wilson, L. and Saseen, J.J., "Gouty Arthritis: A Review of Acute Management and Prevention", Pharmacotherapy, 36 (8), 906–922, August 2016. | ||
| In article | |||
| [3] | Londono, L., Makutonin, M., Dure, A., Canakis, J. and Dominguez, L.W., "An Atypical Presentation of a Polyarticular Gout Flare: Case Report", Cureus, 15 (10), e46967, October 2023. | ||
| In article | View Article PubMed | ||
| [4] | AlSinan, F.M., Sabaa, F., Alkhaldi, M.S., AlArafah, S., Alshuqayfi, H.A. and Almutairi, F., "Atypical Presentation of Gouty Arthritis That Mimics Hand Soft Tissue Infection: Case Report", Rheumatology, 2024. | ||
| In article | View Article PubMed | ||
| [5] | Espi, M., Koppe, L., Fouque, D. and Thaunat, O., "Chronic Kidney Disease-Associated Immune Dysfunctions: Impact of Protein-Bound Uremic Retention Solutes on Immune Cells", Toxins, 12 (5), 300, May 2020. | ||
| In article | |||
| [6] | Kannuthurai, V. and Gaffo, A., "Management of Patients with Gout and Kidney Disease: A Review of Available Therapies and Common Missteps", Kidney360, 4 (9), e1332–e1340, September 2023. | ||
| In article | |||
| [7] | Gheit, Y., Gheit, I.S., Ierulli, J. and Mbaga, I., "Rare Case of Gout Leading to Septic Arthritis, Osteomyelitis, and Septic Shock in an Elderly Patient", Cureus, 15 (11), e48836, November 2023. | ||
| In article | |||
| [8] | Tzanis, P., Klavdianou, K., Lazarini, A., Theotikos, E., Balanika, A., Fanouriakis, A. and Elezoglou, A., "Septic Arthritis Complicating a Gout Flare: Report of Two Cases and Review of the Literature", Mediterranean Journal of Rheumatology, 33 (1), 75–80, March 2022. | ||
| In article | |||
| [9] | Yu, K.H., Luo, S.F., Liou, L.B., Wu, Y.J., Tsai, W.P., Chen, J.Y. and Ho, H.H., "Concomitant septic and gouty arthritis—an analysis of 30 cases", Rheumatology (Oxford, England), 42 (9), 1062–1066, September 2003. | ||
| In article | |||
| [10] | Lim, S.Y., Lu, N. and Choi, H.K., "Septic arthritis in gout patients: a population-based cohort study", Rheumatology (Oxford, England), 54 (11), 2095–2099, November 2015. | ||
| In article | |||
| [11] | Hong, C.C., Chan, M.C., Wu, T., Toh, M., Tay, Y.J. and Tan, J.H., "Does concomitant gout in septic arthritis affect surgical outcomes?", Injury, 54 (2), 409–415, February 2023. | ||
| In article | |||
Published with license by Science and Education Publishing, Copyright © 2025 Najlaa Al-Sudani
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | FitzGerald, J.D., "Gout", Annals of Internal Medicine, 178 (3), ITC33–ITC48, March 2025. | ||
| In article | View Article PubMed | ||
| [2] | Wilson, L. and Saseen, J.J., "Gouty Arthritis: A Review of Acute Management and Prevention", Pharmacotherapy, 36 (8), 906–922, August 2016. | ||
| In article | |||
| [3] | Londono, L., Makutonin, M., Dure, A., Canakis, J. and Dominguez, L.W., "An Atypical Presentation of a Polyarticular Gout Flare: Case Report", Cureus, 15 (10), e46967, October 2023. | ||
| In article | View Article PubMed | ||
| [4] | AlSinan, F.M., Sabaa, F., Alkhaldi, M.S., AlArafah, S., Alshuqayfi, H.A. and Almutairi, F., "Atypical Presentation of Gouty Arthritis That Mimics Hand Soft Tissue Infection: Case Report", Rheumatology, 2024. | ||
| In article | View Article PubMed | ||
| [5] | Espi, M., Koppe, L., Fouque, D. and Thaunat, O., "Chronic Kidney Disease-Associated Immune Dysfunctions: Impact of Protein-Bound Uremic Retention Solutes on Immune Cells", Toxins, 12 (5), 300, May 2020. | ||
| In article | |||
| [6] | Kannuthurai, V. and Gaffo, A., "Management of Patients with Gout and Kidney Disease: A Review of Available Therapies and Common Missteps", Kidney360, 4 (9), e1332–e1340, September 2023. | ||
| In article | |||
| [7] | Gheit, Y., Gheit, I.S., Ierulli, J. and Mbaga, I., "Rare Case of Gout Leading to Septic Arthritis, Osteomyelitis, and Septic Shock in an Elderly Patient", Cureus, 15 (11), e48836, November 2023. | ||
| In article | |||
| [8] | Tzanis, P., Klavdianou, K., Lazarini, A., Theotikos, E., Balanika, A., Fanouriakis, A. and Elezoglou, A., "Septic Arthritis Complicating a Gout Flare: Report of Two Cases and Review of the Literature", Mediterranean Journal of Rheumatology, 33 (1), 75–80, March 2022. | ||
| In article | |||
| [9] | Yu, K.H., Luo, S.F., Liou, L.B., Wu, Y.J., Tsai, W.P., Chen, J.Y. and Ho, H.H., "Concomitant septic and gouty arthritis—an analysis of 30 cases", Rheumatology (Oxford, England), 42 (9), 1062–1066, September 2003. | ||
| In article | |||
| [10] | Lim, S.Y., Lu, N. and Choi, H.K., "Septic arthritis in gout patients: a population-based cohort study", Rheumatology (Oxford, England), 54 (11), 2095–2099, November 2015. | ||
| In article | |||
| [11] | Hong, C.C., Chan, M.C., Wu, T., Toh, M., Tay, Y.J. and Tan, J.H., "Does concomitant gout in septic arthritis affect surgical outcomes?", Injury, 54 (2), 409–415, February 2023. | ||
| In article | |||



{kind=link}
{kind=link}