Previous studies have shown that remimazolam has a lesser effect on hemodynamics and postoperative cognitive function than propofol. In this study, we recruited sixty elderly patients undergoing neurointerventional operation under remimazolam or propofol anesthesia. The results showed that in comparison with propofol, remimazolam provided more stable hemodynamics but higher bispectral index during anesthesia induction. Patients' cognitive function declined slightly after operation, but did not differ between the two anesthetic protocols.
Anesthesia induction and tracheal intubation frequently induces hemodynamic fluctuations, especially in elderly patients 1. Propofol is the most commonly used anesthetic agent for general anesthesia because of its rapid onset and offset. However, propofol often causes hypotension and injection pain 2. To avoid severe adverse events due to hypotension and hypertension, other anesthetics have been used instead of propofol for anesthesia induction and tracheal intubation in elderly patients such as etomidate. However, etomidate may induce myoclonus which has been a concern 3. Therefore, finding a better anesthetic with less effect on hemodynamics and fewer side effects is always an issue for anesthesiologists.
Remimazolam is a short-acting benzodiazepine. Recently, many studies have shown that remimazolam induces less hypotension and injection pain compared with propofol in anesthesia 4, 5, 6. Several studies have shown that remimazolam may provide better hemodynamic anesthesia than propofol in elderly patients 7, 8. However, Sekiguchi et al. 9 found no difference in hemodynamics between the two drugs during anesthesia induction in middle-aged and elderly patients. In addition, elderly patients with neurological impairment were more susceptible to general anesthesia 10. Evidence comparing remimazolam and propofol on hemodynamics during induction of anesthesia and postoperative cognitive function in elderly patients undergoing neurointerventional operation has been limited. This study was designed to evaluate hemodynamics during induction of anesthesia and postoperative cognitive function using remimazolam compared with propofol in elderly patients undergoing neurointerventional operation.
This study was approved by the Ethics Committee of Hunan Provincial People’s Hospital (2021-11). Inclusion criteria were age ≥ 60 years, American Society of Anesthesiologists (ASA) classification I to III, and those who were undergoing neurological endovascular therapy under general anesthesia with tracheal intubation. Exclusion criteria were allergy to propofol, remimazolam, or opioids; combined severe cardiac, pulmonary, hepatic, or renal disease; mental impairment; and those who were unable to communicate with health care providers. Sixty patients were randomized into two groups. Signed informed consent was obtained from all participants.
2.2. InterventionsUpon arrival in the operating room, patients were monitored with ECG, pulse oximetry, and noninvasive blood pressure. An intravenous line was placed on the dorsal hand and Ringer's solution was dripped. Bispectral index (BIS) was monitored on the patient's forehead. Before induction of anesthesia, patients inhaled oxygen at a flow rate of 5 L/min through a face mask. Anesthesia induction was started with an intravenous injection of 0.3 ug/kg sufentanil, patients in group R were injected with additional remimazolam for a total dose of 0.2 to 0.4 mg/kg, patients in group P were injected with additional propofol for a total dose of 1 to 2 mg/kg, then 0.2 mg/kg cisatracurium was injected for muscle relaxation. Patients were ventilated manually for 3 minutes. If the BIS value was less than 60, the patients were intubated using a video laryngoscope. Mechanical ventilation was adjusted to a tidal volume of 6 to 8 ml/kg, a respiratory rate of 10 to 15 breaths/min, an inspired oxygen fraction of 40% to 60%, and a fresh gas flow of 2 L/min. Anesthesia was maintained with remimazolam 0.5 to 2 mg/kg/h in group R and propofol 4 to 10 mg/kg/h in group P, respectively, with BIS maintained at 40-60. Remifentanil was infused at 0.05-0.1 ug/kg/min for analgesia, and cisatracurium was injected intermittently for muscle relaxation. During anesthesia, dopamine 1 to 2 mg was injected when systolic blood pressure (SBP) was less than 80 mmHg, and atropine 0.2 to 0.5 mg was injected when heart rate (HR) was less than 45 bpm. If SBP was greater than 180 mmHg or HR was greater than 100 bpm, sufentanil, remifentanil, or urapidil could be injected at the discretion of the anesthesiologist. If hypotension was frequent, vasopressors such as dopamine and norepinephrine could be infused. At the end of operation, the anesthetic infusion was stopped and the patient was transferred to the post-anesthesia care unit (PACU) for recovery. Upon recovery of consciousness and muscle strength, the patients were extubated and transferred to the ward for nursing care.
2.3. Data CollectionPatient demographics, education level, comorbidities, operative time, and extubation time were recorded. During induction of anesthesia, SBP, mean arterial pressure (MAP), diastolic blood pressure (DBP), HR, and BIS were recorded at T0 (baseline), T1 (after sufentanil injection), T2 (immediately before tracheal intubation), T3 (immediately after tracheal intubation), T4 (2 min after tracheal intubation), T5 (4 min after tracheal intubation), and T6 (5 min after extubation). The incidence of hypotension (SBP < 90 mmHg), hypertension (SBP > 180 mmHg), bradycardia (HR < 50 bpm), tachycardia (HR > 100 bpm), hiccups, injection pain, dopamine and atropine use during induction of anesthesia, and vasopressor infusion during operation were also recorded. Patients' cognitive function was assessed with Mini-Mental State Examination (MMSE) scores preoperatively and on days 1 and 3 postoperatively 11. The incidence of postoperative cognitive dysfunction (POCD), defined as a decrease in MMSE score of more than 2 after operation, was also recorded on days 1 and 3 after operation.
2.4. OutcomesThe primary outcomes of the study were hemodynamics during induction of anesthesia and postoperative MMSE scores. Secondary outcomes included the incidence of hypotension, hypertension, bradycardia, tachycardia, hiccups, injection pain, BIS changes, use of dopamine and atropine during induction of anesthesia, intraoperative vasopressor infusion, extubation time (time from completion of operation to extubation), and the incidence of POCD.
2.5. Statistical AnalysisSPSS 24 was used for statistical analysis. Data are presented as mean with standard deviation (SD) and number with percentage. Patient demographics, operative time, extubation time, and MMSE scores were compared by Student's t-test. SBP, DBP, MAP, HR, and BIS were compared by two-way analysis of variance. Incidence of adverse events and use of vasoactive medications were compared by χ2 test or Fisher's exact test. A p-value < 0.05 was considered statistically different.
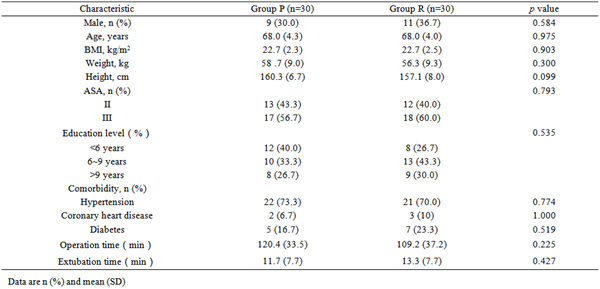
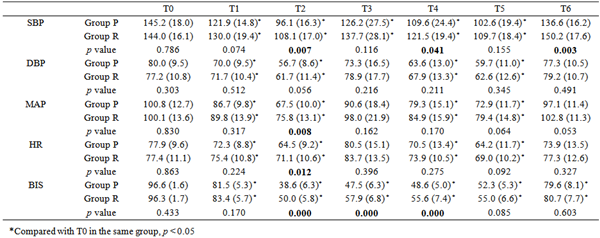
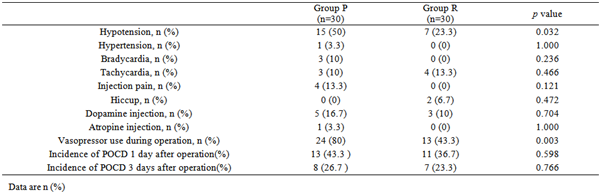
As shown in Table 1, patient demographics were not significantly different (p > 0.05). As shown in Table 2, SBP, DBP, MAP, HR and BIS decreased significantly in both groups during induction of anesthesia (p < 0.05). However, SBP, MAP, and HR at T2 were significantly higher in group R than in group P (p = 0.007, p = 0.008, and p = 0.012, respectively). SBP at T4 and T6 was also significantly higher in group R than in group P (p = 0.041). BIS at T2 to T4 was significantly higher in group R than in group P (p < 0.001). In addition, as shown in Table 3, the incidence of hypotension during induction of anesthesia was significantly higher in group P than in group R (50% vs. 23.3%, p = 0.032). More patients in group P received intraoperative vasopressor infusion compared to group R (80% vs. 43.3%, p = 0.003). Other adverse events and the use of dopamine or atropine during induction of anesthesia were comparable between groups (p > 0.05).
As shown in Table 4, preoperative MMSE scores were comparable between groups (p = 0.553). On the first postoperative day, the MMSE scores decreased significantly, and on the third postoperative day, the MMSE scores increased slightly in both groups. However, postoperative MMSE scores were significantly lower than preoperative scores in both groups (p < 0.05), and no significant difference was found between the two groups (p > 0.05).
This study showed that compared with propofol, remimazolam produced more stable blood pressure, heart rate, and BIS during induction of anesthesia and tracheal intubation in elderly patients undergoing neurointerventional operation. Remimazolam induced fewer episodes of hypotension during induction than propofol and reduced the need for intraoperative vasopressor use. However, we found no differences in postoperative cognitive function between remimazolam and propofol anesthesia.
In the early days, remimazolam was used for procedural sedation, and the incidence of hypotension and injection pain with remimazolam infusion was lower than with propofol 5, 6. For tracheal intubation during induction of anesthesia, patients should be deeply anesthetized, so the dose of remimazolam may be higher than for procedural sedation. A previous study by Dai et al. 4 showed that Remimazolam decreased blood pressure in a dose-dependent manner, and the incidence of hypotension induced by 0.4 mg/kg remimazolam was not significantly different from that induced by 2 mg/kg propofol. Elderly patients are generally sensitive to anesthetics and are likely to experience hemodynamic fluctuations during induction of anesthesia and tracheal intubation 1. To avoid confounding hypotension during induction of anesthesia in elderly patients, etomidate, an early developed anesthetic, was usually used instead of propofol 12. However, etomidate frequently induces myoclonus, which is of concern to anesthesiologists 3, 12. Therefore, remimazolam may be a better candidate for induction of anesthesia in elderly patients. Xu et al. 7 compared remimazolam with propofol for induction of anesthesia and tracheal intubation in elderly patients and found that MAP was significantly higher in remimazolam anesthetized patients than in propofol anesthetized patients. However, the sufentanil dose in the study was inconsistent among patients (ranging from 0.3 to 0.5 ug/kg), resulting in variable tolerance to anesthesia and intubation stimulation 13. Gao et al. 14 compared remimazolam and propofol used for induction of anesthesia in elderly patients and found that the MAPs at different time points were comparable except for the time just before intubation. In addition, Sekiguchi et al. 9 induced anesthesia with infusion of remimazolam (12 mg/kg/h) and target-controlled infusion of propofol (3 ug/ml) in middle-aged and elderly patients, MAP and HR decreased in both anesthesia induction protocols and were not significantly different between the protocols. Therefore, it was still unclear whether remimazolam was superior to propofol on hemodynamics during induction of anesthesia and intubation in elderly patients. In our study, we used sufentanil 0.3 ug/kg in both groups, and the results showed that SBP, MAP, HR, and BIS were slightly but significantly higher in group R than in group P during induction of anesthesia. In addition, remimazolam provided more stable vital signs during neurointerventional operation, resulting in fewer patients requiring the use of vasopressors than propofol anesthesia.
Kuang et al. 15 compared remimazolam and propofol on cognitive function using multiple neuropsychological tests in elderly patients undergoing pulmonary lobectomy, they found that the MMSE scores on day 7 after surgery were comparable between remimazolam and propofol anesthesia. Postoperative cognitive function was affected by variable factors, including diabetes, hypothermia, anesthetic medications, etc. 16. In our study, patients' education level, comorbidities, and MMSE scores were similar between groups, and MMSE scores decreased slightly after operation in both groups. However, the MMSE scores on day 1 and day 3 after neurointerventional operation were comparable between the groups, which was consistent with the previous study. These results indicated that despite more stable intraoperative blood pressure, HR, and BIS value, cognitive function was still impaired after operation. In addition, this study also suggested that remimazolam anesthesia may be non-inferior to propofol on cognitive function after neurointerventional operation in elderly patients.
There were several limitations in the study. First, the sample size was small, a larger scale study may be necessary to validate the findings of the study. Second, we merely evaluated cognitive function by MMSE scores on day 1 and day 3 after operation, performing multiple cognitive function evaluations may be more convincing. Third, a long time follow-up on postoperative cognitive function such as 1 or 3 months after operation may be more valuable.
In comparison with propofol, remimazolam provided more stable hemodynamics during anesthesia induction in elderly patients. Patients cognitive function slightly declined after neurointerventional operation but did not differ between the two anesthesia protocol.
This research is funded by Health Commission of Hunan Province (202104111828).
| [1] | Boztas N, Oztekin S, Ozkardesler S, Akan M, Ozbilgin S, Baytok A. Effects of different doses of remifentanil on hemodynamic response to anesthesia induction in healthy elderly patients. Curr Med Res Opin. 2017 Jan; 33(1): 85-90. | ||
| In article | |||
| [2] | Liu X, Xiao Q, Zhuang S. Comparison of propofol-esketamine versus propofol for anesthesia in gastroscopy: a double-blind, randomized controlled clinical trial. Front Med (Lausanne). 2023 Aug 8; 10: 1184709. | ||
| In article | |||
| [3] | Zhang KD, Wang LY, Zhang DX, Zhang ZH, Wang HL. Comparison of the Effectiveness of Various Drug Interventions to Prevent Etomidate-Induced Myoclonus: A Bayesian Network Meta-Analysis. Front Med (Lausanne). 2022 Apr 26; 9: 799156. | ||
| In article | |||
| [4] | Dai G, Pei L, Duan F, Liao M, Zhang Y, Zhu M, Zhao Z, Zhang X. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia. Minerva Anestesiol. 2021 Oct; 87(10): 1073-1079. | ||
| In article | |||
| [5] | Zhang X, Li S, Liu J. Efficacy and safety of remimazolam besylate versus propofol during hysteroscopy: single-centre randomized controlled trial. BMC Anesthesiol. 2021 May 20; 21(1): 156. | ||
| In article | |||
| [6] | Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020 Aug; 34(4): 543-553. | ||
| In article | |||
| [7] | Xu Q, Wu J, Shan W, Duan G, Lan H. Effects of remimazolam combined with sufentanil on hemodynamics during anesthetic induction in elderly patients with mild hypertension undergoing orthopedic surgery of the lower limbs: a randomized controlled trial. BMC Anesthesiol. 2023 Sep 14; 23(1): 311. | ||
| In article | |||
| [8] | Kim TK, Kwak HJ, Jung WS, Choi GB, Park SY, Kim JY. Effects of Remimazolam Anesthesia with Two Induction Doses on Hemodynamics and Recovery Profile in Older Patients: Comparison with Propofol Anesthesia. J Clin Med. 2023 Aug 14; 12(16): 5285. | ||
| In article | |||
| [9] | Sekiguchi R, Kinoshita M, Kawanishi R, Kakuta N, Sakai Y, Tanaka K. Comparison of hemodynamics during induction of general anesthesia with remimazolam and target-controlled propofol in middle-aged and elderly patients: a single-center, randomized, controlled trial. BMC Anesthesiol. 2023 Jan 10; 23(1): 14. | ||
| In article | |||
| [10] | Abou-Chebl A, Yeatts SD, Yan B, Cockroft K, Goyal M, Jovin T, Khatri P, Meyers P, Spilker J, Sugg R, Wartenberg KE, Tomsick T, Broderick J, Hill MD. Impact of General Anesthesia on Safety and Outcomes in the Endovascular Arm of Interventional Management of Stroke (IMS) III Trial. Stroke. 2015 Aug; 46(8): 2142-8. | ||
| In article | |||
| [11] | Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975 Nov; 12(3): 189-98. | ||
| In article | |||
| [12] | Shen XC, Ao X, Cao Y, Lan L, Liu XM, Sun WJ, Li P, Lan CH. Etomidate-remifentanil is more suitable for monitored anesthesia care during gastroscopy in older patients than propofol-remifentanil. Med Sci Monit. 2015 Jan 1; 21: 1-8. | ||
| In article | |||
| [13] | Choi BH, Lee YC. Effective Bolus Dose of Sufentanil to Attenuate Cardiovascular Responses in Laryngoscopic Double-Lumen Endobronchial Intubation. Anesth Pain Med. 2016 Apr 4; 6(2): e33640. | ||
| In article | |||
| [14] | Gao J, Yang C, Ji Q, Li J. Effect of remimazolam versus propofol for the induction of general anesthesia on cerebral blood flow and oxygen saturation in elderly patients undergoing carotid endarterectomy. BMC Anesthesiol. 2023 May 4; 23(1): 153. | ||
| In article | |||
| [15] | Kuang Q, Zhong N, Ye C, Zhu X, Wei F. Propofol Versus Remimazolam on Cognitive Function, Hemodynamics, and Oxygenation During One-Lung Ventilation in Older Patients Undergoing Pulmonary Lobectomy: A Randomized Controlled Trial. J Cardiothorac Vasc Anesth. 2023 Oct; 37(10): 1996-2005. | ||
| In article | |||
| [16] | Wang L, Chen B, Liu T, Luo T, Kang W, Liu W. Risk factors for delayed neurocognitive recovery in elderly patients undergoing thoracic surgery. BMC Anesthesiol. 2023 Mar 31; 23(1): 102. | ||
| In article | |||
Published with license by Science and Education Publishing, Copyright © 2024 Qian Huang, Tao Hu, Ying Yang, Yuying He, Yingzi Ling, Gaoyin Kong and Yi Zou
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Boztas N, Oztekin S, Ozkardesler S, Akan M, Ozbilgin S, Baytok A. Effects of different doses of remifentanil on hemodynamic response to anesthesia induction in healthy elderly patients. Curr Med Res Opin. 2017 Jan; 33(1): 85-90. | ||
| In article | |||
| [2] | Liu X, Xiao Q, Zhuang S. Comparison of propofol-esketamine versus propofol for anesthesia in gastroscopy: a double-blind, randomized controlled clinical trial. Front Med (Lausanne). 2023 Aug 8; 10: 1184709. | ||
| In article | |||
| [3] | Zhang KD, Wang LY, Zhang DX, Zhang ZH, Wang HL. Comparison of the Effectiveness of Various Drug Interventions to Prevent Etomidate-Induced Myoclonus: A Bayesian Network Meta-Analysis. Front Med (Lausanne). 2022 Apr 26; 9: 799156. | ||
| In article | |||
| [4] | Dai G, Pei L, Duan F, Liao M, Zhang Y, Zhu M, Zhao Z, Zhang X. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia. Minerva Anestesiol. 2021 Oct; 87(10): 1073-1079. | ||
| In article | |||
| [5] | Zhang X, Li S, Liu J. Efficacy and safety of remimazolam besylate versus propofol during hysteroscopy: single-centre randomized controlled trial. BMC Anesthesiol. 2021 May 20; 21(1): 156. | ||
| In article | |||
| [6] | Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020 Aug; 34(4): 543-553. | ||
| In article | |||
| [7] | Xu Q, Wu J, Shan W, Duan G, Lan H. Effects of remimazolam combined with sufentanil on hemodynamics during anesthetic induction in elderly patients with mild hypertension undergoing orthopedic surgery of the lower limbs: a randomized controlled trial. BMC Anesthesiol. 2023 Sep 14; 23(1): 311. | ||
| In article | |||
| [8] | Kim TK, Kwak HJ, Jung WS, Choi GB, Park SY, Kim JY. Effects of Remimazolam Anesthesia with Two Induction Doses on Hemodynamics and Recovery Profile in Older Patients: Comparison with Propofol Anesthesia. J Clin Med. 2023 Aug 14; 12(16): 5285. | ||
| In article | |||
| [9] | Sekiguchi R, Kinoshita M, Kawanishi R, Kakuta N, Sakai Y, Tanaka K. Comparison of hemodynamics during induction of general anesthesia with remimazolam and target-controlled propofol in middle-aged and elderly patients: a single-center, randomized, controlled trial. BMC Anesthesiol. 2023 Jan 10; 23(1): 14. | ||
| In article | |||
| [10] | Abou-Chebl A, Yeatts SD, Yan B, Cockroft K, Goyal M, Jovin T, Khatri P, Meyers P, Spilker J, Sugg R, Wartenberg KE, Tomsick T, Broderick J, Hill MD. Impact of General Anesthesia on Safety and Outcomes in the Endovascular Arm of Interventional Management of Stroke (IMS) III Trial. Stroke. 2015 Aug; 46(8): 2142-8. | ||
| In article | |||
| [11] | Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975 Nov; 12(3): 189-98. | ||
| In article | |||
| [12] | Shen XC, Ao X, Cao Y, Lan L, Liu XM, Sun WJ, Li P, Lan CH. Etomidate-remifentanil is more suitable for monitored anesthesia care during gastroscopy in older patients than propofol-remifentanil. Med Sci Monit. 2015 Jan 1; 21: 1-8. | ||
| In article | |||
| [13] | Choi BH, Lee YC. Effective Bolus Dose of Sufentanil to Attenuate Cardiovascular Responses in Laryngoscopic Double-Lumen Endobronchial Intubation. Anesth Pain Med. 2016 Apr 4; 6(2): e33640. | ||
| In article | |||
| [14] | Gao J, Yang C, Ji Q, Li J. Effect of remimazolam versus propofol for the induction of general anesthesia on cerebral blood flow and oxygen saturation in elderly patients undergoing carotid endarterectomy. BMC Anesthesiol. 2023 May 4; 23(1): 153. | ||
| In article | |||
| [15] | Kuang Q, Zhong N, Ye C, Zhu X, Wei F. Propofol Versus Remimazolam on Cognitive Function, Hemodynamics, and Oxygenation During One-Lung Ventilation in Older Patients Undergoing Pulmonary Lobectomy: A Randomized Controlled Trial. J Cardiothorac Vasc Anesth. 2023 Oct; 37(10): 1996-2005. | ||
| In article | |||
| [16] | Wang L, Chen B, Liu T, Luo T, Kang W, Liu W. Risk factors for delayed neurocognitive recovery in elderly patients undergoing thoracic surgery. BMC Anesthesiol. 2023 Mar 31; 23(1): 102. | ||
| In article | |||