We report a case of Adult-onset Still’s Disease (AoSD) in a 55-year-old male without prior rheumatological history. The disease is an autoinflammatory condition with features including fevers, joint pain, and salmon-colored lesions. Diagnosis is through clinical classification systems including the Yamaguchi or Fautrel criteria and considered after a thorough diagnosis of exclusion. However, the disease is rare and difficult to recognize given its nonspecific presentation. This patient depicts the challenges in noticing the disease, especially in the setting of confounding physical exam findings. Prognosis is favorable, but prolonged periods without treatment can lead to the development of harmful complications including fulminant hepatitis, lymphohistiocytic activation syndrome, and disseminated intravascular coagulation.
Discovered by E.G. Bywaters in 1971, Adult-onset Still’s Disease (AoSD) is the adult manifestation of Systemic Juvenile Idiopathic Arthritis (SJIA) 1. This condition is uncommon with one retrospective study finding an incidence of 1.6 cases per 1,000,000 [1-2] 1. The etiology is unclear but centers on immune cell activation resulting in an autoinflammatory cascade akin to a “cytokine storm” 3. Diagnosis is clinical with high suspicion for those presenting with a fever that has no clear source in conjunction with rashes, arthralgias, or elevated serum markers. Of the various classification systems, the Yamaguchi criteria is the most sensitive 4.
However, diagnosis is challenging as AoSD is rare, has overlapping presentations with other conditions, and lacks definitive diagnostic labs or imaging. The workup is extensive and necessitates exclusion of multiple pathologies. This often results in improper and delayed diagnosis in up to 80% of patients eventually diagnosed with AoSD 5.
Our case showcases a challenging diagnosis of AoSD in a patient whose cardiac murmur and initial presentation were initially presumed to be from endocarditis.
A 55-year-old male presented for workup of intermittently persistent bilateral lower extremity pain and swelling with generalized body aches in his arms and shoulders that have been ongoing for the past few months. The patient described his pain as more muscular rather than skeletal and at times debilitating to the point where he has trouble moving. Of note, he describes pharyngitis and pleuritic chest pain prior to onset of pain. There was also a prolonged period of daily fevers, but this was not well documented. Past medical history includes post-traumatic stress disorder, anxiety, and hypertension. He denied any history of rheumatological conditions, alcohol, smoking, illicit drug usage, and previous episodes of discomfort like this current admission.
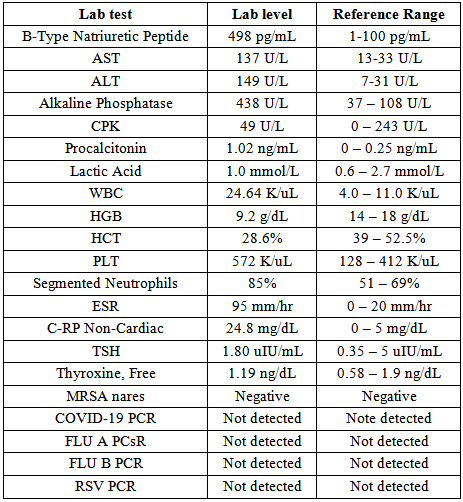
In the emergency department he was tachycardic with a heart rate of 116, mildly febrile with a temperature of 100.4 degrees Fahrenheit, and endorsed a pain score of 10/10. His respiratory rate and blood pressure were unremarkable. Pertinent physical exam findings included a systolic murmur heard at the cardiac apex with diffuse tenderness to palpation on all his extremities. His neurological exam was normal and there were no visible skin abnormalities. Complete lab work on admission is listed below in Table 1.
Imaging revealed cardiomegaly on CXR, an enlarged right hilar lymph node on CT chest, and hepatomegaly on CT abdomen pelvis. Transthoracic echocardiogram (TTE) revealed moderate aortic stenosis but was negative for valvular vegetations. Despite the TTE, empiric vancomycin and ceftriaxone were started since there was still concern for infection. The following day he reported no clinical improvement on antibiotics. There was increased suspicion for a rheumatological condition, and a dose of empiric colchicine was provided. Further lab work revealed an unremarkable Rheumatoid Factor (RF), Human Immunodeficiency Virus (HIV), and Antinuclear Antibody (ANA), but the patient’s improvement on colchicine, coupled with no growth on cultures, pointed away from an infection. Ferritin was also significantly elevated at >1500 ng/mL. AoSD was suspected and the patient was started on daily prednisone 40 mg. Inflammatory markers immediately began to downtrend, white blood cell count dropped, liver function tests (LFTs) normalized, and the patient began to drastically improve with no complaints of body aches. Cultures remained negative, the entire hospital admission and antibiotics were discontinued. On the day of discharge, one week after admission, repeat ferritin decreased to 1188.4 ng/mL and the patient was set up for outpatient rheumatology follow up.
Diagnosis of AoSD was challenging in our patient given the nonspecific symptoms mimicking infection coupled with a cardiac murmur later found to be aortic stenosis. Without a TEE, there remained heightened suspicion for blood culture-negative endocarditis despite a negative TTE and cultures without growth. Only after a lack of clinical improvement on antibiotics and elevation of multiple inflammatory markers was an autoimmune condition including AoSD considered.
Multiple classification systems exist to diagnose AoSD, but the Japanese Yamaguchi criteria seen below in Table 2 is widely adopted with a sensitivity of 93.5% 6.
Our patient satisfied 2 major criteria of arthralgia and leukocytosis and 4 minor criteria of abnormal LFTs, lymphadenopathy, hepatomegaly, and negative ANA and RF.
A newer French classification system known as the Fautrel criteria seen below in Table 3 is less sensitive than the Yamaguchi criteria, but more specific 7.
We cannot say with certainty enough criteria for the Fautrel classification system were met. Two major criteria of arthralgia, and elevated polymorphonuclear cells were definitively met. Given the markedly elevated serum ferritin, there is ample reason to suspect criteria of glycosylated ferritin would have been satisfied had the lab test been conducted. Additionally, the patient endorsed prolonged subjective fevers that were not documented along with pharyngitis prior to disease onset.
3.2. Additional FindingsLabs are not themselves diagnostic for AoSD, but many patients tend to exhibit elevated markers, which we see incorporated into various classification criteria. LFTs are commonly elevated with reports of elevated markers in up to 75% of cases, including our patient 8. This manifestation is believed to be affiliated with interleukin (IL) – 18, which was found to be elevated in those with acute liver injury but not chronic injury 9. This cytokine functions by inducing other cytokines and activating T helper cells, macrophages, natural killer cells, etc. 10. One such case found elevated IL-18 in macrophages and Kupffer cells within the liver parenchyma 11. Common findings on biopsy of AoSD with liver dysfunction include lobular inflammation, Kupffer cell hyperplasia, focal hepatocellular degermation, periportal mononuclear infiltrates, etc. 9.
Hyperferritinemia is another common observation reported in those with AoSD. Up to 90% of patients with AoSD are found with elevated serum ferritin levels 12. Our patient was no exception with serum ferritin levels greater than 1500 ng/mL. Ferritin appears promising as a diagnostic marker as values greater than five times the upper limit of normal (>1,000 ng/mL) have shown sensitivities up to 80% in patients who have a fever with no clear cause. When coupled with glycosylated ferritin less than 20%, sensitivity increases up to 93% 13. Additionally, we see correlations between ferritin levels and disease activity, making it a potential biomarker for treatment response 14. In our own case, ferritin levels were initially unquantifiable before decreasing down to 1188.4 ng/mL on day of discharge. However, its usefulness is limited due to its elevated presence of multiple disease pathologies and the limited availability of glycosylated ferritin 15. Like with LFTs, pathogenesis is cytokine mediated involving molecules such as IL-18 that regulate ferritin synthesis and all stages 16. One study attributes this control through both a direct process and an indirect process through increased nitric oxide synthesis, which in turn induces ferritin production 17.
It is unlikely this patient’s aortic stenosis was a result of his AoSD. However, we see rare instances in the literature of cardiac involvement with AoSD. Around 5% of cases of AoSD involve the heart with the most common manifestation being pericardial effusion 18. Few cases report non-infective endocarditis with valvular manifestations, often left-sided 19. Histopathologic findings typically reveal fibrinoid necrosis with lymphohistiocytic infiltration that resolves after prolonged treatment with steroids [19-20] 19. The pathogenesis of cardiac manifestations is unclear, but research points to increased production of adhesion molecules including soluble intercellular adhesion molecule-1 (sICAM-1) that enhances leukocyte adhesion to the heart’s endocardial surface 21.
AoSD is a challenging diagnosis of exclusion as its differential is extensive, requiring rule out of infections, malignancy, drug interactions, and other rheumatological conditions. This often leads to frequent misdiagnosis and postponed care. Early diagnosis is essential as some of the complications may be life threatening. Until adequate lab tests are developed, an extensive history and physical remains the cornerstone of diagnosis in AoSD. Physicians should exercise a heightened level of suspicion and consider AoSD when presented with a fever that has no clear source.
| [1] | Bywaters, E.G, “Still’s Disease in the Adult.” | ||
| In article | View Article PubMed | ||
| [2] | Veetil, A., Manu, B., Yee, A.H., Warrington, K.J., Aksamit, A.J., and Mason, T.G., May. 2010. | ||
| In article | View Article PubMed | ||
| [3] | Ma, Y., Meng, J., Jia, J., Wang, M., Teng, J., Zhu, D., Yang, C., and Hu, Q., 2021. “Current and Emerging Biological Therapy in Adult-Onset Still’s Disease.” , June 2021. | ||
| In article | View Article PubMed | ||
| [4] | Kumar, S., Kunhiraman, D.S., and Rajam, L., 2012. “Application of the Yamaguchi Criteria for Classification of ‘suspected’ Systemic Juvenile Idiopathic Arthritis (sJIA).” , Nov 2012. | ||
| In article | View Article PubMed | ||
| [5] | Carreño, M. A., Carvallo, A., Trejo, C., Ballestero, F., and Martínez, C., 2009. “Adult Still’s Disease. A Great Simulator. Retrospective Review of 20 Patients,” , 1010-1016, Aug 2009. | ||
| In article | View Article | ||
| [6] | Masson, C., Loet, X.L., Liote, F., Dubost, J.J., Boissier, M.C., Perroux-Goumy, L., Bregeon, C., and Audran, M., 1996. “Comparative Study of 6 Types of Criteria in Adult Still’s Disease.” | ||
| In article | |||
| [7] | Lebrun, D., Mestrallet, S., Dehoux, M., Golmard, J.L., Granger, B., Georgin-Lavialle, S., Arnaud, L., Grateau, G., Pouchot, J., and Fautrel, B., “Validation of the Fautrel Classification Criteria for Adult-Onset Still’s Disease.” Seminars in Arthritis and Rheumatism 47 (4), 578-585, Feb 2018. | ||
| In article | View Article PubMed | ||
| [8] | Pouchot, J., Sampalis, J.S., Beaudet, F., Carette, S., Décary, F., Salusinsky-Sternbach, M., Hill, R.O., Gutkowski, A., Harth, M., and Myhal, D., “Adult Still’s Disease: Manifestations, Disease Course, and Outcome in 62 Patients.” , 118-136, Mar 1991. | ||
| In article | View Article PubMed | ||
| [9] | Lim, K.B.L., and Schiano, T.D., “Still Disease and the Liver—An Underappreciated Association.” -846, Dec 2011. | ||
| In article | |||
| [10] | Ihim, S.A., Abubakar, S.D., Zian, Z., Sasaki, T., Saffarioun, M., Maleknia, S., and Azizi, G., 2022. “Interleukin-18 Cytokine in Immunity, Inflammation, and Autoimmunity: Biological Role in Induction, Regulation, and Treatment.” | ||
| In article | View Article PubMed | ||
| [11] | Priori, R., Barone, F., Alessandri, C., Colafrancesco, S., McInnes, I.B., Pitzalis, C., Valesini, G., and Bombardieri, M., “Markedly Increased IL-18 Liver Expression in Adult-Onset Still’s Disease-Related Hepatitis.” | ||
| In article | View Article PubMed | ||
| [12] | Efthimiou, P., Kontzias, A., Hur, P., Rodha, K., Ramakrishna, G. S., and Nakasato, P., “Adult-Onset Still’s Disease in Focus: Clinical Manifestations, Diagnosis, Treatment, and Unmet Needs in the Era of Targeted Therapies.” | ||
| In article | View Article PubMed | ||
| [13] | Seco, T., Cerqueira, A., Costa, A., Fernandes, C., and Cotter, J., “Adult-Onset Still’s Disease: Typical Presentation, Delayed Diagnosis.” Cureus 12 (6), June 2020. [Online]. | ||
| In article | View Article | ||
| [14] | Akritidis, N., Giannakakis, I., and Giouglis, T., 1996. “Ferritin Levels and Response to Treatment in Patients with Adult Still’s Disease.” | ||
| In article | |||
| [15] | Bella, M., and Efthimiou, Petros.,“Ferritin in Adult-Onset Still’s Disease: Just a Useful Innocent Bystander?” | ||
| In article | |||
| [16] | Feist, E., Mitrovic, S., and Fautrel, B., “Mechanisms, Biomarkers and Targets for Adult-Onset Still’s Disease.” , Oct 2018. | ||
| In article | View Article PubMed | ||
| [17] | Weiss, G., Goossen, B., Doppler, W., Fuchs, D., Pantopoulos, K., Werner-Felmayer, G., Wachter, H., and Hentze, M.W., “Translational Regulation via Iron-Responsive Elements by the Nitric oxide/NO-Synthase Pathway.” -3657, Sep 1993. | ||
| In article | View Article PubMed | ||
| [18] | Zenagui, D., and De Coninck, J.P., “Atypical Presentation of Adult Still’s Disease Mimicking Acute Bacterial Endocarditis.” | ||
| In article | View Article PubMed | ||
| [19] | Dang, X., Han, Y., and Zhang, X., “Endocarditis in Adult-Onset Still Disease: A Case Report and Literature Review.” -1200, Aug 2018. | ||
| In article | View Article PubMed | ||
| [20] | Oka, K., Yuya, Y., Yasuda, M., and Otsuka, F., “Adult-269, Nov 2020. | ||
| In article | View Article PubMed | ||
| [21] | Bodard, Q., Langlois, V., Guilpain, P., | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2023 Su Hyun Jeong, Nishitha Shekhar, Matthew Amin, Amir Nabizadeh and Neelesh Mutyala
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
https://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
https://creativecommons.org/licenses/by/4.0/
| [1] | Bywaters, E.G, “Still’s Disease in the Adult.” | ||
| In article | View Article PubMed | ||
| [2] | Veetil, A., Manu, B., Yee, A.H., Warrington, K.J., Aksamit, A.J., and Mason, T.G., May. 2010. | ||
| In article | View Article PubMed | ||
| [3] | Ma, Y., Meng, J., Jia, J., Wang, M., Teng, J., Zhu, D., Yang, C., and Hu, Q., 2021. “Current and Emerging Biological Therapy in Adult-Onset Still’s Disease.” , June 2021. | ||
| In article | View Article PubMed | ||
| [4] | Kumar, S., Kunhiraman, D.S., and Rajam, L., 2012. “Application of the Yamaguchi Criteria for Classification of ‘suspected’ Systemic Juvenile Idiopathic Arthritis (sJIA).” , Nov 2012. | ||
| In article | View Article PubMed | ||
| [5] | Carreño, M. A., Carvallo, A., Trejo, C., Ballestero, F., and Martínez, C., 2009. “Adult Still’s Disease. A Great Simulator. Retrospective Review of 20 Patients,” , 1010-1016, Aug 2009. | ||
| In article | View Article | ||
| [6] | Masson, C., Loet, X.L., Liote, F., Dubost, J.J., Boissier, M.C., Perroux-Goumy, L., Bregeon, C., and Audran, M., 1996. “Comparative Study of 6 Types of Criteria in Adult Still’s Disease.” | ||
| In article | |||
| [7] | Lebrun, D., Mestrallet, S., Dehoux, M., Golmard, J.L., Granger, B., Georgin-Lavialle, S., Arnaud, L., Grateau, G., Pouchot, J., and Fautrel, B., “Validation of the Fautrel Classification Criteria for Adult-Onset Still’s Disease.” Seminars in Arthritis and Rheumatism 47 (4), 578-585, Feb 2018. | ||
| In article | View Article PubMed | ||
| [8] | Pouchot, J., Sampalis, J.S., Beaudet, F., Carette, S., Décary, F., Salusinsky-Sternbach, M., Hill, R.O., Gutkowski, A., Harth, M., and Myhal, D., “Adult Still’s Disease: Manifestations, Disease Course, and Outcome in 62 Patients.” , 118-136, Mar 1991. | ||
| In article | View Article PubMed | ||
| [9] | Lim, K.B.L., and Schiano, T.D., “Still Disease and the Liver—An Underappreciated Association.” -846, Dec 2011. | ||
| In article | |||
| [10] | Ihim, S.A., Abubakar, S.D., Zian, Z., Sasaki, T., Saffarioun, M., Maleknia, S., and Azizi, G., 2022. “Interleukin-18 Cytokine in Immunity, Inflammation, and Autoimmunity: Biological Role in Induction, Regulation, and Treatment.” | ||
| In article | View Article PubMed | ||
| [11] | Priori, R., Barone, F., Alessandri, C., Colafrancesco, S., McInnes, I.B., Pitzalis, C., Valesini, G., and Bombardieri, M., “Markedly Increased IL-18 Liver Expression in Adult-Onset Still’s Disease-Related Hepatitis.” | ||
| In article | View Article PubMed | ||
| [12] | Efthimiou, P., Kontzias, A., Hur, P., Rodha, K., Ramakrishna, G. S., and Nakasato, P., “Adult-Onset Still’s Disease in Focus: Clinical Manifestations, Diagnosis, Treatment, and Unmet Needs in the Era of Targeted Therapies.” | ||
| In article | View Article PubMed | ||
| [13] | Seco, T., Cerqueira, A., Costa, A., Fernandes, C., and Cotter, J., “Adult-Onset Still’s Disease: Typical Presentation, Delayed Diagnosis.” Cureus 12 (6), June 2020. [Online]. | ||
| In article | View Article | ||
| [14] | Akritidis, N., Giannakakis, I., and Giouglis, T., 1996. “Ferritin Levels and Response to Treatment in Patients with Adult Still’s Disease.” | ||
| In article | |||
| [15] | Bella, M., and Efthimiou, Petros.,“Ferritin in Adult-Onset Still’s Disease: Just a Useful Innocent Bystander?” | ||
| In article | |||
| [16] | Feist, E., Mitrovic, S., and Fautrel, B., “Mechanisms, Biomarkers and Targets for Adult-Onset Still’s Disease.” , Oct 2018. | ||
| In article | View Article PubMed | ||
| [17] | Weiss, G., Goossen, B., Doppler, W., Fuchs, D., Pantopoulos, K., Werner-Felmayer, G., Wachter, H., and Hentze, M.W., “Translational Regulation via Iron-Responsive Elements by the Nitric oxide/NO-Synthase Pathway.” -3657, Sep 1993. | ||
| In article | View Article PubMed | ||
| [18] | Zenagui, D., and De Coninck, J.P., “Atypical Presentation of Adult Still’s Disease Mimicking Acute Bacterial Endocarditis.” | ||
| In article | View Article PubMed | ||
| [19] | Dang, X., Han, Y., and Zhang, X., “Endocarditis in Adult-Onset Still Disease: A Case Report and Literature Review.” -1200, Aug 2018. | ||
| In article | View Article PubMed | ||
| [20] | Oka, K., Yuya, Y., Yasuda, M., and Otsuka, F., “Adult-269, Nov 2020. | ||
| In article | View Article PubMed | ||
| [21] | Bodard, Q., Langlois, V., Guilpain, P., | ||
| In article | View Article PubMed | ||