Over 200 recent Guillain-Barré syndrome (GBS) cases in India have raised public health concerns. Infections, notably Campylobacter jejuni and some vaccines, are known risk factors, but causes are still not fully understood. Reports link GBS with Hepatitis E virus (HEV) infection, especially since HEV is common in developing countries like India. This systematic review examines comorbidities, clinical features, and outcomes in GBS patients with HEV infection. A systematic review was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, focusing on published case reports of HEV infection in patients later diagnosed with GBS. Google Scholar was used to find relevant studies, including all available full-text reports of GBS after HEV infection. Data were organized in tables and analyzed, and the review protocol was registered with the International Prospective Register of Systematic Reviews (PROSERO: CRD420251102115). After applying selection criteria, 15 case reports from 13 different countries were analyzed. Of the 15 patients (average age 44.6 years), 11 were male (73%). The primary treatment was intravenous immunoglobulin (IVIG), which resulted in complete recovery for 13 cases (87%), while 2 patients (13%) achieved only partial recovery, experiencing residual limb weakness. There were no fatalities reported. This review shows that GBS is a notable extra-hepatic complication of HEV infection. Diagnosing GBS in HEV cases requires thorough cerebrospinal fluid (CSF) analysis and nerve conduction tests. Patients with HEV should be monitored for neurological symptoms, as early detection and intervention can improve outcomes and minimize lasting neurological issues.
Hepatitis caused Hepatitis E virus (HEV) is a zoonotic disease which causes acute viral hepatitis. It is the leading cause of viral hepatitis in developing countries. HEV is a single- stranded RNA virus belonging to the Orthohepevirus genus of the Hepeviridae family and measures around 27 to 34 nm in diameter. HEV is primarily spread via contaminated water and undercooked meat. Its small size and non-enveloped structure facilitate feco-oral transmission, and aids in resistance to environmental stressors such as heat and acidic conditions, thereby contributing to its pathogenicity. People infected with HEV develop both hepatic and extra hepatic manifestations making the prognosis of patients extremely challenging. Most common extra hepatic manifestations include neurological complications such as Guillain Barré syndrome (GBS) and bilateral brachial neuritis 1, 2. Here, in this systematic review, we discuss the inter-relationship between HEV being the predisposing factor for GBS.
GBS, also known as acute inflammatory demyelinating polyradiculoneuropathy (AIDP) is a rare autoimmune disorder affecting mainly peripheral nervous system and produces neurological manifestations. GBS is of public health concern right now in various countries 3. The aetiology of GBS is multifactorial which includes infectious triggers like Campylobacter jejuni, Mycoplasma pneumoniae, Cytomegalovirus (CMV), Epstein Barr virus (EBV) etc., and other triggers include vaccinations, surgery and trauma 4. GBS generally has a history of starting few days after viral infections 5.
Although it was rare in the past, GBS linked to HEV infection has been on the rise in recent decades. Initial symptoms include fatigue and jaundice with elevated liver enzymes- alanine aminotransferase (ALT) and aspartate aminotransferase (AST). Additional hepatic manifestations of HEV infection include hepatomegaly, pale stools, dark urine, etc. Few patients also reported respiratory failure 6, myocarditis 7 muscle pain 8, peripheral neuropathy 9, and impaired superficial and deep reflexes 10 after the acute phase of HEV infection. This systematic review is carried out to elucidate potential comorbidities, presentations and outcomes of patients with HEV infections developing GBS.
This systematic review is reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The study period extends from March 2025 to February 2026 and to locate potential papers, we searched the PubMed and Google Scholar databases. Medical Subject Headings (MeSH) keywords including “Hepatitis E virus (HEV)” infection, “Guillain-Barré syndrome (GBS)”, “HEV and GBS case reports”, “HEV diagnosis”, “GBS diagnosis”, “Guillain-Barré syndrome pathophysiology”, “GBS electromyography, and nerve conduction investigations” were used throughout the literature extraction procedure (PROSERO, the International Prospective Register of Systematic Reviews registration number: CRD420251102115).
2.1. Diagnostic Criteria for Guillain–Barré SyndromeTo ensure consistency and validity in case identification, we applied established diagnostic criteria for GBS. Specifically, the Brighton Collaboration case definition was used, which provides standardized levels of diagnostic certainty based on clinical features, cerebrospinal fluid (CSF) analysis, and electrophysiological findings.
The core clinical criteria included:
a. Acute onset of bilateral and relatively symmetric limb weakness.
b. Decreased or absent deep tendon reflexes in affected limbs.
c. Monophasic illness pattern with progression over ≤ 4 weeks.
Supportive criteria included:
d. CSF findings of albuminocytologic dissociation (elevated protein with normal cell count).
e. Electrophysiological evidence of demyelination or axonal neuropathy.
Cases were classified according to Brighton levels of diagnostic certainty (Level 1–4), with Level 1 representing the highest diagnostic confidence. Where studies did not explicitly reference Brighton criteria, we assessed whether reported diagnostic features aligned with these standards.
By clearly defining and applying standardized diagnostic criteria, this review minimizes heterogeneity in case ascertainment and strengthens the reliability of conclusions regarding the association between HEV and GBS 11, 12.
2.2. Inclusion CriteriaThis investigation includes English-language literature, case reports of patients of all ages, patients with a positive HEV infection, and patients with a GBS diagnosis.
2.3. Exclusion CriteriaThe study excluded comprehensive reviews and meta-analyses, intervention studies such as randomized and clinical control trials, GBS cases resulting from other etiologies, duplicate case reports, and articles without full text access.
Patient demographics (age, sex, and country), the interval between the onset of HEV infection symptoms and GBS-like symptoms, neurological and non-neurological comorbidities, the methods used for GBS diagnosis, treatment, and management, and patient outcomes were all carefully recorded with reference to each case study that was part of the systematic review.
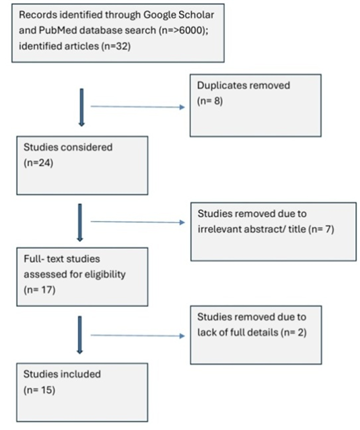
2.4. Assessment of Study Quality and Risk of BiasTo strengthen the validity of this review, we systematically assessed the methodological quality and risk of bias of all included studies. Two reviewers independently performed the assessments, with disagreements resolved by consensus. (Figure 1)
HEV-related GBS was found in 32 research articles; 8 duplicates were removed, and 24 papers were reviewed, 17 of which were full-text articles. According to the exclusion criteria, two items were still deemed unsuitable. 15 case reports were therefore included in the study.
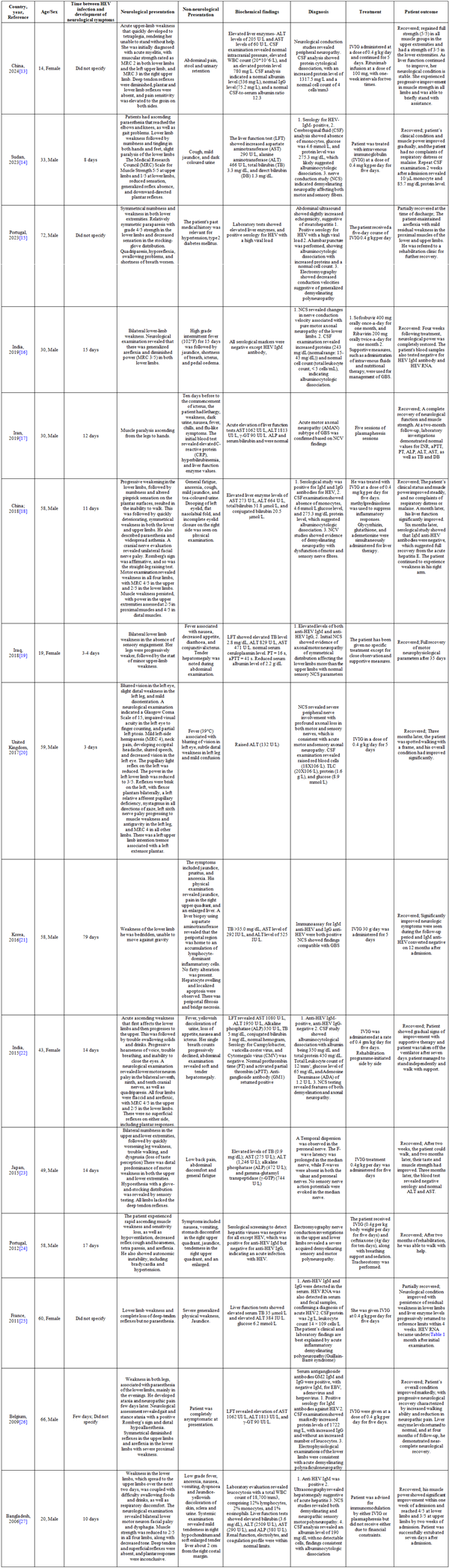
We included 15 reports from 13 different nations out of 32 articles. The patients' average age was 44.6 years. Of them, four (26.6%) were women and eleven (73.3%) were men. After receiving intravenous immunoglobulin (IVIG) treatment, 13 of them healed completely, while 2 only partially recovered with limb weakness. (Table 1)
HEV-Hepatitis E Virus, GBS-Guillain-Barré Syndrome, MRC-Medical Research Council, ALT – Alanine Aminotransferase, AST-Aspartate Aminotransferase, CSF-Cerebrospinal Fluid, IgG-Immunoglobulin G, IgM-Immunoglobulin M, IVIG-Intravenous Immunoglobulin, TB-Total Bilirubin, DB-Direct Bilirubin, LFT-Liver Function Test, NCS-Nerve Conduction Study, NCV-Nerve Conduction Velocity, AMAN-Acute Motor Axonal Neuropathy, γ-GT-Gamma-Glutamyl Transferase, ALP-Alkaline Phosphatase, INR-International Normalized Ratio, PT-Prothrombin Time, aPTT-Activated Partial Thromboplastin Time, TLC-Total Leukocyte Count, ADA-Adenosine Deaminase, GM1-Monosialotetrahexosylganglioside, GM2-Disialotetrahexosylganglioside, GD1a-Disialotetrahexosylganglioside (variant), GQ1b-Tetrasialotetrahexosylganglioside
This descriptive systematic review identified 15 cases of GBS associated with HEV infection, reported from 13 diverse countries, underscoring the global nature of this clinical phenomenon1–3. The mean age of the cohort was 44.6 years, with a predominance of male patients (11 males, 73.3%; 4 females, 26.6%), reflecting trends observed in previous epidemiological studies of HEV-associated neurological complications. Recovery outcomes were generally favourable: 13 patients (86.6%) achieved full recovery after treatment, while 2 patients (13.3%) experienced partial recovery and continued to suffer from residual muscle weakness, consistent with the variable prognosis seen in GBS irrespective of the underlying trigger. HEV was implicated as a precipitating factor for GBS, with the interval between HEV infection and onset of neurological symptoms ranging from as short as 2 days to as long as 79 days (mean 17±20 days), highlighting the unpredictable latency period and suggesting the need for vigilance in patients with recent viral hepatitis1. Diagnostic confirmation relied heavily on CSF analysis, which typically demonstrated albuminocytologic dissociation, and nerve conduction studies (NCS), both of which are regarded as critical investigations for accurate diagnosis of GBS in the context of HEV infection. Therapeutically, IVIG was the principal intervention and remains the cornerstone of GBS management, with high rates of success documented in HEV-associated cases. Nevertheless, a minority of patients may experience incomplete recovery, with persistent weakness or neurological deficits, which mirrors findings in other aetiologies of GBS. Importantly, the association between HEV and GBS has been described across multiple HEV genotypes and geographic regions, further emphasising its significance in global clinical practice and the necessity for multidisciplinary approaches to both diagnosis and management 28, 29, 30, 31.
4.2. Neurological and Systemic PresentationsThe neurological manifestations of HEV-associated GBS are diverse, with ascending symmetrical weakness being the most prominent clinical feature. Patients frequently reported paraesthesia affecting the distal extremities, which typically progressed proximally, often accompanied by generalised areflexia. Cranial nerve involvement was not uncommon, with bilateral lower motor neuron facial palsy and dysphagia being observed in several cases. Quadriparesis, ranging from mild to profound muscle weakness, was a hallmark of more severe presentations. Respiratory compromise, attributed to diaphragmatic or intercostal muscle involvement, occasionally necessitated mechanical ventilation, particularly in cases with bulbar symptoms or rapid disease progression.
Neurophysiological investigations, especially NCS, revealed a spectrum of findings. The most common pattern was demyelinating polyneuropathy, consistent with the acute inflammatory demyelinating polyneuropathy (AIDP) subtype of GBS. However, some individuals exhibited axonal motor neuropathy or mixed central and peripheral demyelination, highlighting the heterogeneity of the neurological involvement in HEV-associated GBS. Systemic symptoms often paralleled the neurological decline. Commonly reported features included low-grade fever, anorexia, nausea, vomiting, pruritus, and abdominal discomfort. In rare instances, patients developed severe complications such as myocarditis or acute respiratory failure, underscoring the potential for multi-organ involvement in HEV infection. Hepatic manifestations were also prominent and included clinical features such as jaundice, hepatomegaly, dark-coloured urine, and biochemical evidence of hepatic dysfunction, with elevated liver enzymes (ALT, AST, and bilirubin) documented in most cases. These findings reinforce the importance of a multidisciplinary approach to diagnosis and management, as both neurological and hepatic systems may be simultaneously affected in HEV-associated GBS 32.
4.3. Diagnostic MethodsThe diagnosis of HEV-associated GBS relies on a combination of serological, CSF, and neurophysiological investigations to confirm both the infectious and neurological components of the disease. Serological testing typically involves enzyme immunoassays for the detection of anti-HEV IgM and IgG antibodies, which serve as markers for acute and past infection, respectively. In cases where additional confirmation is required, molecular techniques such as polymerase chain reaction (PCR) are employed to identify HEV RNA in serum or stool samples, thereby establishing an active viral infection and increasing diagnostic specificity.
CSF analysis is a cornerstone in the diagnosis of GBS, with the most consistent finding being albuminocytologic dissociation, characterised by elevated protein concentrations in the absence of significant pleocytosis (increased cell count). This hallmark pattern supports the diagnosis of GBS in the appropriate clinical context. Neurophysiological studies, particularly NCS, are indispensable for further characterising the subtype of GBS. The majority of HEV-associated GBS cases demonstrate evidence of demyelinating polyneuropathy, though axonal neuropathy or mixed demyelinating and axonal features may also be observed. Collectively, these diagnostic modalities enable clinicians to differentiate HEV-associated GBS from other causes of acute flaccid paralysis and guide appropriate management strategies 28, 33, 34.
4.4. Treatment and Management StrategiesThe management of patients with HEV-associated GBS was multidisciplinary, focusing on both neurological and hepatic aspects of the disease. IVIG therapy represented the cornerstone of neurological intervention, with the standard regimen consisting of an infusion at a dose of 0.4 g/kg/day over five consecutive days. This approach was associated with favourable outcomes, including significant improvement in muscle strength and functional recovery in most cases. In instances where IVIG was not feasible due to financial or logistical constraints, plasmapheresis was considered as an alternative immunomodulatory therapy, although its use was less common in the reviewed cohort. Supportive care played a crucial role in the overall management strategy. Mechanical ventilation was initiated for patients experiencing respiratory compromise, often necessitated by bulbar involvement or ascending paralysis. In addition, comprehensive rehabilitation programmes, including physiotherapy, occupational therapy, and nutritional support, were implemented to facilitate neuromuscular recovery and prevent complications such as contractures or malnutrition. Hepatic management was tailored to the severity of liver involvement. Patients presenting with acute hepatitis manifestations, such as jaundice and hepatomegaly, were closely monitored and managed with hepatoprotective agents. In select cases, corticosteroids and antiviral medications were administered to mitigate hepatic inflammation and reduce viral replication, respectively. The integration of hepatic and neurological interventions, combined with vigilant supportive care, was instrumental in achieving optimal recovery and minimising the risk of long-term sequelae 34.
4.5. Geographical and Genotype VariationsAnalysis of patient outcomes in HEV-associated GBS reveals notable geographical and genotype-specific variations. In Asian regions such as India, China, Korea, Japan, Iraq, Iran, and Bangladesh, genotype 1 HEV appears to predominate, frequently presenting with severe hepatic manifestations alongside neurological symptoms. These patients typically exhibited pronounced jaundice, hepatomegaly, and elevated liver enzyme levels, with recovery outcomes often dependent on the prompt initiation of IVIG therapy. Notably, full recovery was observed in several cases, although the presence of severe hepatic involvement occasionally contributed to residual neurological deficits or prolonged convalescence 35. In African cohorts, exemplified by cases reported in Sudan, patients with HEV infection predominantly developed acute demyelinating neuropathy. The administration of IVIG was associated with favourable clinical outcomes, leading to complete neurological recovery in most instances. This suggests that regional differences in HEV genotype and healthcare access may influence both the severity of GBS presentations and the likelihood of optimal recovery.
In contrast, European cases, particularly those from France, Belgium, Portugal, and the United Kingdom, were often linked to genotype 3 HEV infection. These patients tended to be older and frequently presented with a broader spectrum of recovery outcomes, ranging from full resolution of symptoms to persistent weakness or partial recovery. The variability in prognosis may reflect differences in host factors, underlying comorbidities, and genotype-specific pathogenic mechanisms. Furthermore, genotype 3 has been associated with less severe hepatic involvement but a higher propensity for neurological sequelae in elderly populations 36. Collectively, these findings underscore the importance of considering both geographical origin and HEV genotype when assessing clinical presentation, management strategies, and recovery outcomes in HEV-associated GBS. Further multicentre studies are warranted to clarify the mechanisms underlying these regional and genotype-related disparities and to inform tailored therapeutic approaches.
4.6. Pathophysiological Mechanisms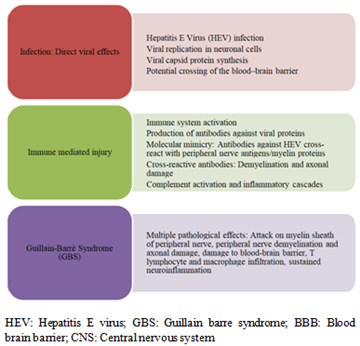
The interplay between HEV infection and GBS illustrates a complex pathogenic mechanism that warrants deeper clinical attention. Evidence suggests HEV may exert direct neurotropic effects, replicating within neuronal cells and potentially breaching the blood–brain barrier. More prominently, immune-mediated pathways drive neurological injury: molecular mimicry between HEV antigens and host neural structures induces cross-reactive antibodies, leading to demyelination and axonal damage characteristic of GBS. Complement activation and inflammatory cascades amplify this process, while T lymphocytes and macrophages contribute to sustained neuroinflammation. These findings highlight that HEV-associated GBS is not a singular phenomenon but rather the result of converging viral replication, antibody cross-reactivity, and immune dysregulation. Recognizing this multifactorial pathogenesis is essential for refining diagnostic strategies, guiding therapeutic interventions, and prioritizing genotype-specific research. Ultimately, integrating HEV into broader discussions of post-infectious neuropathies underscores the importance of vigilance in identifying emerging viral triggers of GBS within global neurology and infectious disease frameworks 31, 37, 38, 39, 40. (Figure 2)
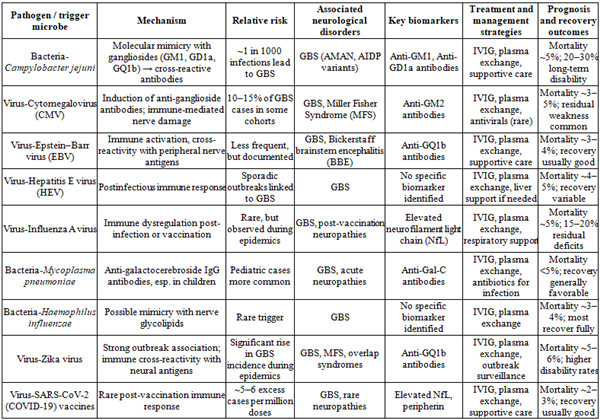
GBS is the most common cause of acute neuromuscular paralysis worldwide and is frequently postinfectious in origin. Approximately two-thirds of patients report a preceding respiratory or gastrointestinal illness. Campylobacter jejuni is the most strongly associated pathogen, with an estimated incidence of one GBS case per 1000 infections. The mechanism involves molecular mimicry, whereby bacterial lipo-oligosaccharides resemble host gangliosides including monosialotetrahexosylganglioside (GM1), disialotetrahexosylganglioside (GD1a), tetrasialotetrahexosylganglioside (GQ1b), leading to cross-reactive antibodies that damage peripheral nerves. Other infectious agents implicated include CMV, EBV, HEV, Influenza A virus (IAV), Mycoplasma pneumoniae, Haemophilus influenzae, and Zika virus. In particular, Mycoplasma pneumoniae infection has been linked to anti-galactocerebroside IgG antibodies, especially in pediatric cases. Viral outbreaks, such as Zika epidemics, have been associated with sharp increases in GBS incidence, underscoring the role of emerging pathogens. The clinical presentation typically involves rapidly progressive symmetrical weakness, areflexia, and potential respiratory compromise. These findings highlight the importance of infection-related immune responses in the pathogenesis of GBS and the need for vigilance during outbreaks of implicated pathogens. Understanding the etiological spectrum of infection-related GBS is critical for timely diagnosis, appropriate management, and the development of preventive strategies 41, 42, 43, 44, 45, 46, 47, 48. (Table 2)
GBS-Guillain-Barré Syndrome, AMAN-Acute Motor Axonal Neuropathy, AIDP-Acute Inflammatory Demyelinating Polyradiculoneuropathy, CMV-Cytomegalovirus, MFS-Miller Fisher Syndrome, GM1-Monosialotetrahexosylganglioside, GM2-Disialotetrahexosylganglioside, GD1a-Disialotetrahexosylganglioside, GQ1b-Tetrasialotetrahexosylganglioside, EBV-Epstein–Barr Virus, BBE-Bickerstaff Brainstem Encephalitis, HEV-Hepatitis E Virus, IAV-Influenza A Virus, NfL-Neurofilament Light Chain, IgG – Immunoglobulin G, IgM-Immunoglobulin M, Gal-C-Galactocerebroside, IVIG-Intravenous Immunoglobulin, SARS-CoV-2-Severe Acute Respiratory Syndrome Coronavirus 2, CNS-Central Nervous System, BBB-Blood–Brain Barrier
Study Limitations
This review has several limitations that should be acknowledged. First, the search strategy may not have been exhaustive, as it relied on a limited number of databases and may have missed relevant studies published elsewhere. Second, the inclusion and exclusion criteria were not always applied with the rigor expected in systematic reviews, which raises the possibility of selection bias. Third, the heterogeneity of the included studies, spanning different populations, diagnostic methods, and reporting standards, limits the ability to synthesize findings into a unified conclusion. Fourth, quality assessment of the included studies was not consistently performed using validated tools, making it difficult to evaluate the strength of the evidence. Fifth, the review is descriptive rather than quantitative; no metaanalysis was conducted, which restricts the ability to estimate pooled effect sizes or assess statistical significance. Finally, the review is contextspecific and may not reflect broader epidemiological patterns across different regions or healthcare systems. These limitations mean that the findings should be interpreted cautiously and viewed as preliminary rather than definitive.
Future Recommendations
Future studies should adopt more rigorous and standardized methodologies to strengthen the evidence base on the association between HEV infection and GBS. Large, multicenter, prospective studies are needed to establish causality and to better define the epidemiological burden across different regions. Researchers should employ comprehensive diagnostic protocols, including molecular assays and serological confirmation, to ensure accurate case identification. Comparative studies examining HEVassociated GBS versus GBS triggered by other viral infections would help clarify unique clinical features and outcomes. In addition, systematic reviews in this area should follow exhaustive database searches, and formal riskofbias assessments. Finally, future work should explore therapeutic responses and longterm neurological outcomes in HEVassociated GBS patients, which could inform clinical management and public health strategies.
In summary, the evidence presented substantiates HEV as a significant infectious trigger for GBS, with clinical onset typically occurring within days to weeks of acute infection. The syndrome most frequently manifests as ascending weakness, areflexia, and cranial nerve involvement, often accompanied by hepatic dysfunction such as jaundice and raised liver enzymes. Diagnosis is supported by HEV serology and RNA detection, with CSF analysis demonstrating albuminocytologic dissociation and nerve conduction studies confirming demyelinating or axonal neuropathy. IVIG remains the principal therapeutic approach, with adjunctive use of plasmapheresis, corticosteroids, or antivirals guided by the extent of hepatic involvement. Prognosis is generally favourable, though a subset of patients may experience persistent deficits. Notably, genotypic variation appears to influence geographic distribution and possibly neurotropism, underscoring the importance of genotype-specific research. The underlying pathogenesis is likely driven by molecular mimicry, mirroring mechanisms seen in GBS triggered by other pathogens. These findings highlight the necessity for clinicians to include HEV in the differential diagnosis of GBS, particularly in endemic areas or when hepatic symptoms are present. Further prospective studies are warranted to elucidate incidence rates, genotype correlations, and long-term outcomes in this context.
Funding
None
Acknowledgments
None
Conflict of interest
None
Ethical considerations
Approval of the research protocol
No human participant was involved in this study
Informed Consent
Not applicable
Registry and the Registration No. of the study/trial
Not applicable
Animal Studies
Not applicable
| [1] | Dalton, H. R., Saunders, M., & Woolson, K. L. (2015). Hepatitis E virus in developed countries: one of the most successful zoonotic viral diseases in human history?. Journal of virus eradication, 1(1), 23–29. | ||
| In article | View Article PubMed | ||
| [2] | Cheung, M. C., Maguire, J., Carey, I., Wendon, J., & Agarwal, K. (2012). Review of the neurological manifestations of hepatitis E infection. Annals of Hepatology, 11(5), 618-622. | ||
| In article | View Article PubMed | ||
| [3] | Sharma S, Virk A, Bharti B, Viswanathan VT, Grover S. Guillain-Barré Syndrome Outbreak in Pune, India: Epidemiological Insights and Public Health Implications. Int J Appl Basic Med Res. 2025 Jul-Sep; 15(3): 139-142. | ||
| In article | View Article PubMed | ||
| [4] | Finsterer, J. (2022). Triggers of Guillain–Barré syndrome: Campylobacter jejuni predominates. International journal of molecular sciences, 23(22), 14222. | ||
| In article | View Article PubMed | ||
| [5] | Kandi V. Guillain-Barré Syndrome Outbreak in Pune, India, Calls for Heightened Awareness and Preparedness. Cureus. 2025 Feb 6; 17(2): e78609. | ||
| In article | View Article | ||
| [6] | Noushad, M. A., Limnatitou, D., Bhattacharjee, S., & Mohd Nor, A. (2021). Diaphragmatic paralysis resulting in respiratory failure as a feature of hepatitis E virus-associated neuralgic amyotrophy. BMJ case reports, 14(4), e242113. | ||
| In article | View Article PubMed | ||
| [7] | Premkumar, M., Rangegowda, D., Vashishtha, C., Bhatia, V., Khumuckham, J. S., & Kumar, B. (2015). Acute viral hepatitis e is associated with the development of myocarditis. Case reports in hepatology, 2015, 458056. | ||
| In article | View Article PubMed | ||
| [8] | Ripellino, P., Pasi, E., Melli, G., Staedler, C., Fraga, M., Moradpour, D., Sahli, R., Aubert, V., Martinetti, G., Bihl, F., Bernasconi, E., Terziroli Beretta-Piccoli, B., Cerny, A., Dalton, H. R., Zehnder, C., Mathis, B., Zecca, C., Disanto, G., Kaelin-Lang, A., & Gobbi, C. (2019). Neurologic complications of acute hepatitis E virus infection. Neurology(R) neuroimmunology & neuroinflammation, 7(1), e643. | ||
| In article | View Article PubMed | ||
| [9] | Lhomme, S., Abravanel, F., Cintas, P., & Izopet, J. (2021). Hepatitis E Virus Infection: Neurological Manifestations and Pathophysiology. Pathogens (Basel, Switzerland), 10(12), 1582. | ||
| In article | View Article PubMed | ||
| [10] | Bandyopadhyay, D., Ganesan, V., Choudhury, C., Kar, S. S., Karmakar, P., Choudhary, V., Banerjee, P., Bhar, D., Hajra, A., Layek, M., & Mukhopadhyay, S. (2015). Two Uncommon Causes of Guillain-Barré Syndrome: Hepatitis E and Japanese Encephalitis. Case reports in neurological medicine, 2015, 759495. | ||
| In article | View Article PubMed | ||
| [11] | Fokke C, van den Berg B, Drenthen J, Walgaard C, van Doorn PA, Jacobs BC. Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria. Brain. 2014; 137(1): 33–43. | ||
| In article | View Article PubMed | ||
| [12] | Ghazanfar H, Qazi R, Ghazanfar A, Iftekhar S. Significance of Brighton Criteria in the Early Diagnosis and Management of Guillain-Barré Syndrome. Cureus. 2020; 12(5): e8318. | ||
| In article | View Article | ||
| [13] | Zhou, X., Peng, A., Li, C., Li, L., Yao, D., Hao, Y., Zhao, C., Yan, Q., Li, Y., Liu, J., Liu, S., Zhu, W., Du, Y., & Zhang, W. (2024). Combined central and peripheral demyelination: a case report resembling encephalomyeloradiculoneuropathy. Frontiers in neurology, 14, 1288546. | ||
| In article | View Article PubMed | ||
| [14] | Ahmed, A., El-Sadig, S. M., & Siddig, E. E. (2023). Guillain-Barre syndrome associated with hepatitis E virus infection: A case report. Clinical case reports, 11(9), e7863. | ||
| In article | View Article PubMed | ||
| [15] | Rodrigues, R. A., Sequeira, M., Barros, F., Alves, T., & Gonçalves, J. (2023). Acute Hepatitis E-Associated Guillain-Barré Syndrome. Cureus, 15(11), e48778. | ||
| In article | View Article PubMed | ||
| [16] | Choudhary, M. C., Bajpai, V., Anand, L., & Gupta, E. (2019). Guillain-Barré syndrome in a patient of acute Hepatitis E virus infection associated with genotype 1: Case report and literature review. Intractable & rare diseases research, 8(1), 43–47. | ||
| In article | View Article PubMed | ||
| [17] | Samadi, A., Mansour-Ghanaei, F., Joukar, F., Mavaddati, S., & Sufi Afshar, I. (2019). A 30-Year-Old Man with Acute Motor Axonal Neuropathy Subtype of Guillain-Barré Syndrome Having Hepatitis A Virus Infection. Middle East journal of digestive diseases, 11(2), 110–115. | ||
| In article | View Article PubMed | ||
| [18] | Zheng, X., Yu, L., Xu, Q., Gu, S., & Tang, L. (2018). Guillain-Barre syndrome caused by hepatitis E infection: case report and literature review. BMC infectious diseases, 18(1), 50. | ||
| In article | View Article PubMed | ||
| [19] | Al-Saffar, A., & Al-Fatly, B. (2018). Acute Motor Axonal Neuropathy in Association with Hepatitis E. Frontiers in neurology, 9, 62. | ||
| In article | View Article PubMed | ||
| [20] | Salim, O. J., Davidson, A., Li, K., Leach, J. P., & Heath, C. (2017). Brainstem encephalitis and acute polyneuropathy associated with hepatitis E infection. BMJ case reports, 2017, bcr2017220799. https: //pmc.ncbi.nlm.nih.gov/articles/PMC5623255/. | ||
| In article | View Article PubMed | ||
| [21] | Ji, S. B., Lee, S. S., Jung, H. C., Kim, H. J., Kim, H. J., Kim, T. H., Jung, W. T., Lee, O. J., & Song, D. H. (2016). A Korean patient with Guillain-Barré syndrome following acute hepatitis E whose cholestasis resolved with steroid therapy. Clinical and molecular hepatology, 22(3), 396–399. | ||
| In article | View Article PubMed | ||
| [22] | Bandyopadhyay, D., Ganesan, V., Choudhury, C., Kar, S. S., Karmakar, P., Choudhary, V., ... & Mukhopadhyay, S. (2015). Two uncommon causes of Guillain‐Barré syndrome: Hepatitis E and Japanese encephalitis. Case Reports in Neurological Medicine, 2015(1), 759495. | ||
| In article | View Article PubMed | ||
| [23] | Higuchi, M. A., Fukae, J., Tsugawa, J., Ouma, S., Takahashi, K., Mishiro, S., & Tsuboi, Y. (2015). Dysgeusia in a patient with Guillain-Barre syndrome associated with acute hepatitis E: a case report and literature review. Internal Medicine, 54(12), 1543-1546. | ||
| In article | View Article PubMed | ||
| [24] | Citation style for this article: Santos L, Mesquita J R, Rocha Pereira N, Lima-Alves C, Serrão R, Figueiredo P, Reis J, Simões J, Nascimento M S, Sarmento A. Acute hepatitis E complicated by Guillain-Barré syndrome in Portugal, December 2012 – a case report. Euro Surveill. 2013; 18(34): pii=20563. | ||
| In article | View Article PubMed | ||
| [25] | Kamar, N., Bendall, R. P., Peron, J. M., Cintas, P., Prudhomme, L., Mansuy, J. M., Rostaing, L., Keane, F., Ijaz, S., Izopet, J., & Dalton, H. R. (2011). Hepatitis E virus and neurologic disorders. Emerging infectious diseases, 17(2), 173–179. | ||
| In article | View Article PubMed | ||
| [26] | Loly, J. P., Rikir, E., Seivert, M., Legros, E., Defrance, P., Belaiche, J., ... & Delwaide, J. (2009). Guillain-Barre syndrome following hepatitis E. World journal of gastroenterology: WJG, 15(13), 1645. | ||
| In article | View Article PubMed | ||
| [27] | Khanam, R. A., Faruq, M. O., Basunia, R. A., & Ahsan, A. A. (2009). Guillain-Barré Syndrome Associated with Acute HEV Hepatitis. Ibrahim Medical College Journal, 2(1), 32–34. | ||
| In article | View Article | ||
| [28] | Rath, J., Zulehner, G., Schober, B., Grisold, A., Krenn, M., Cetin, H., & Zimprich, F. (2021). Cerebrospinal fluid analysis in Guillain-Barré syndrome: value of albumin quotients. Journal of neurology, 268(9), 3294–3300. | ||
| In article | View Article PubMed | ||
| [29] | Primadharsini PP, Nagashima S, Okamoto H. Genetic Variability and Evolution of Hepatitis E Virus. Viruses. 2019 May 18; 11(5): 456. | ||
| In article | View Article PubMed | ||
| [30] | Sidow NO, Hassan MS. Intravenous immunoglobulin treatment with prognosis for the first six months of Guillain-Barré Syndrome in Somalia: Case series. Ann Med Surg (Lond). 2022 Nov 5; 84: 104816. | ||
| In article | View Article | ||
| [31] | Lhomme S, Abravanel F, Cintas P, Izopet J. Hepatitis E Virus Infection: Neurological Manifestations and Pathophysiology. Pathogens. 2021 Dec 3; 10(12): 1582. | ||
| In article | View Article PubMed | ||
| [32] | Trojaborg, W. (1998). Acute and chronic neuropathies: new aspects of Guillain–Barré syndrome and chronic inflammatory demyelinating polyneuropathy, an overview and an update. Electroencephalography and clinical neurophysiology, 107(5), 303-316. | ||
| In article | View Article PubMed | ||
| [33] | Al-Hakem, H., Doets, A. Y., Stino, A. M., Zivkovic, S. A., Andersen, H., Willison, H. J., Cornblath, D. R., Gorson, K. C., Islam, Z., Mohammad, Q. D., Sindrup, S. H., Kusunoki, S., Davidson, A., Casasnovas, C., Bateman, K., Miller, J. A. L., van den Berg, B., Verboon, C., Roodbol, J., Leonhard, S. E., … IGOS Consortium (2023). CSF Findings in Relation to Clinical Characteristics, Subtype, and Disease Course in Patients with Guillain-Barré Syndrome. Neurology, 100(23), e2386–e2397. | ||
| In article | View Article PubMed | ||
| [34] | van Doorn, P. A., Van den Bergh, P. Y. K., Hadden, R. D. M., Avau, B., Vankrunkelsven, P., Attarian, S., Blomkwist-Markens, P. H., Cornblath, D. R., Goedee, H. S., Harbo, T., Jacobs, B. C., Kusunoki, S., Lehmann, H. C., Lewis, R. A., Lunn, M. P., Nobile-Orazio, E., Querol, L., Rajabally, Y. A., Umapathi, T., Topaloglu, H. A., … Willison, H. J. (2023). European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of Guillain-Barré syndrome. European journal of neurology, 30(12), 3646–3674. | ||
| In article | View Article PubMed | ||
| [35] | Songtanin B, Molehin AJ, Brittan K, Manatsathit W, Nugent K. Hepatitis E Virus Infections: Epidemiology, Genetic Diversity, and Clinical Considerations. Viruses. 2023 Jun 17; 15(6): 1389. | ||
| In article | View Article PubMed | ||
| [36] | Smith DB, Ijaz S, Tedder RS, Hogema B, Zaaijer HL, Izopet J, Bradley-Stewart A, Gunson R, Harvala H, Kokki I, Simmonds P. Variability and pathogenicity of hepatitis E virus genotype 3 variants. J Gen Virol. 2015 Nov; 96(11): 3255-3264. | ||
| In article | View Article PubMed | ||
| [37] | Liu, H., & Ma, Y. (2020). Hepatitis E virus-associated Guillain-Barre syndrome: Revision of the literature. Brain and behavior, 10(1), e01496. | ||
| In article | View Article PubMed | ||
| [38] | Lhomme, S., Abravanel, F., Cintas, P., & Izopet, J. (2021). Hepatitis E Virus Infection: Neurological Manifestations and Pathophysiology. Pathogens (Basel, Switzerland), 10(12), 1582. | ||
| In article | View Article PubMed | ||
| [39] | Drave, S. A., Debing, Y., Walter, S., Todt, D., Engelmann, M., Friesland, M., Wedemeyer, H., Neyts, J., Behrendt, P., & Steinmann, E. (2016). Extra-hepatic replication and infection of hepatitis E virus in neuronal-derived cells. Journal of viral hepatitis, 23(7), 512–521. | ||
| In article | View Article PubMed | ||
| [40] | Kamar N, Dalton HR, Abravanel F, et al. Hepatitis E virus infection. Clin Microbiol Rev. 2014; 27(1): 116-138. | ||
| In article | View Article PubMed | ||
| [41] | Naik GS, Meena AK, Reddy BAK, Mridula RK, Jabeen SA, Borgohain R. Anti-ganglioside antibodies profile in Guillain-Barré syndrome: Correlation with clinical features, electrophysiological pattern, and outcome. Neurol India. 2017 Sep-Oct; 65(5): 1001-1005. | ||
| In article | View Article PubMed | ||
| [42] | Yuki N. Guillain-Barré syndrome and anti-ganglioside antibodies: a clinician-scientist's journey. Proc Jpn Acad Ser B Phys Biol Sci. 2012; 88(7): 299-326. | ||
| In article | View Article PubMed | ||
| [43] | Bellanti R, Rinaldi S. Guillain-Barré syndrome: a comprehensive review. Eur J Neurol. 2024 Aug; 31(8): e16365. | ||
| In article | View Article PubMed | ||
| [44] | Willison HJ, Jacobs BC, van Doorn PA. Guillain‑Barré syndrome. Lancet. 2016; 388(10045): 717‑727. | ||
| In article | View Article PubMed | ||
| [45] | Islam Z, et al. Campylobacter jejuni infection and GBS in Bangladesh. Ann Neurol. 2010; 68(6): 961‑971. | ||
| In article | |||
| [46] | van den Berg B, Walgaard C, Drenthen J, et al. Guillain‑Barré syndrome: pathogenesis, diagnosis, treatment and prognosis. Nat Rev Neurol. 2014; 10(8): 469‑482. | ||
| In article | View Article PubMed | ||
| [47] | Dos Santos T, et al. Zika virus and GBS: case series from French Polynesia. Lancet. 2016; 387(10027): 1531‑1539. | ||
| In article | View Article PubMed | ||
| [48] | Kuwabara S, Yuki N. Axonal Guillain‑Barré syndrome: concepts and controversies. Lancet Neurol. 2013; 12(12): 1180‑1188. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2026 Deepthi Arvapally, Venkataramana Kandi, Sabitha Vadakedath and Sriguna Bannur
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Dalton, H. R., Saunders, M., & Woolson, K. L. (2015). Hepatitis E virus in developed countries: one of the most successful zoonotic viral diseases in human history?. Journal of virus eradication, 1(1), 23–29. | ||
| In article | View Article PubMed | ||
| [2] | Cheung, M. C., Maguire, J., Carey, I., Wendon, J., & Agarwal, K. (2012). Review of the neurological manifestations of hepatitis E infection. Annals of Hepatology, 11(5), 618-622. | ||
| In article | View Article PubMed | ||
| [3] | Sharma S, Virk A, Bharti B, Viswanathan VT, Grover S. Guillain-Barré Syndrome Outbreak in Pune, India: Epidemiological Insights and Public Health Implications. Int J Appl Basic Med Res. 2025 Jul-Sep; 15(3): 139-142. | ||
| In article | View Article PubMed | ||
| [4] | Finsterer, J. (2022). Triggers of Guillain–Barré syndrome: Campylobacter jejuni predominates. International journal of molecular sciences, 23(22), 14222. | ||
| In article | View Article PubMed | ||
| [5] | Kandi V. Guillain-Barré Syndrome Outbreak in Pune, India, Calls for Heightened Awareness and Preparedness. Cureus. 2025 Feb 6; 17(2): e78609. | ||
| In article | View Article | ||
| [6] | Noushad, M. A., Limnatitou, D., Bhattacharjee, S., & Mohd Nor, A. (2021). Diaphragmatic paralysis resulting in respiratory failure as a feature of hepatitis E virus-associated neuralgic amyotrophy. BMJ case reports, 14(4), e242113. | ||
| In article | View Article PubMed | ||
| [7] | Premkumar, M., Rangegowda, D., Vashishtha, C., Bhatia, V., Khumuckham, J. S., & Kumar, B. (2015). Acute viral hepatitis e is associated with the development of myocarditis. Case reports in hepatology, 2015, 458056. | ||
| In article | View Article PubMed | ||
| [8] | Ripellino, P., Pasi, E., Melli, G., Staedler, C., Fraga, M., Moradpour, D., Sahli, R., Aubert, V., Martinetti, G., Bihl, F., Bernasconi, E., Terziroli Beretta-Piccoli, B., Cerny, A., Dalton, H. R., Zehnder, C., Mathis, B., Zecca, C., Disanto, G., Kaelin-Lang, A., & Gobbi, C. (2019). Neurologic complications of acute hepatitis E virus infection. Neurology(R) neuroimmunology & neuroinflammation, 7(1), e643. | ||
| In article | View Article PubMed | ||
| [9] | Lhomme, S., Abravanel, F., Cintas, P., & Izopet, J. (2021). Hepatitis E Virus Infection: Neurological Manifestations and Pathophysiology. Pathogens (Basel, Switzerland), 10(12), 1582. | ||
| In article | View Article PubMed | ||
| [10] | Bandyopadhyay, D., Ganesan, V., Choudhury, C., Kar, S. S., Karmakar, P., Choudhary, V., Banerjee, P., Bhar, D., Hajra, A., Layek, M., & Mukhopadhyay, S. (2015). Two Uncommon Causes of Guillain-Barré Syndrome: Hepatitis E and Japanese Encephalitis. Case reports in neurological medicine, 2015, 759495. | ||
| In article | View Article PubMed | ||
| [11] | Fokke C, van den Berg B, Drenthen J, Walgaard C, van Doorn PA, Jacobs BC. Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria. Brain. 2014; 137(1): 33–43. | ||
| In article | View Article PubMed | ||
| [12] | Ghazanfar H, Qazi R, Ghazanfar A, Iftekhar S. Significance of Brighton Criteria in the Early Diagnosis and Management of Guillain-Barré Syndrome. Cureus. 2020; 12(5): e8318. | ||
| In article | View Article | ||
| [13] | Zhou, X., Peng, A., Li, C., Li, L., Yao, D., Hao, Y., Zhao, C., Yan, Q., Li, Y., Liu, J., Liu, S., Zhu, W., Du, Y., & Zhang, W. (2024). Combined central and peripheral demyelination: a case report resembling encephalomyeloradiculoneuropathy. Frontiers in neurology, 14, 1288546. | ||
| In article | View Article PubMed | ||
| [14] | Ahmed, A., El-Sadig, S. M., & Siddig, E. E. (2023). Guillain-Barre syndrome associated with hepatitis E virus infection: A case report. Clinical case reports, 11(9), e7863. | ||
| In article | View Article PubMed | ||
| [15] | Rodrigues, R. A., Sequeira, M., Barros, F., Alves, T., & Gonçalves, J. (2023). Acute Hepatitis E-Associated Guillain-Barré Syndrome. Cureus, 15(11), e48778. | ||
| In article | View Article PubMed | ||
| [16] | Choudhary, M. C., Bajpai, V., Anand, L., & Gupta, E. (2019). Guillain-Barré syndrome in a patient of acute Hepatitis E virus infection associated with genotype 1: Case report and literature review. Intractable & rare diseases research, 8(1), 43–47. | ||
| In article | View Article PubMed | ||
| [17] | Samadi, A., Mansour-Ghanaei, F., Joukar, F., Mavaddati, S., & Sufi Afshar, I. (2019). A 30-Year-Old Man with Acute Motor Axonal Neuropathy Subtype of Guillain-Barré Syndrome Having Hepatitis A Virus Infection. Middle East journal of digestive diseases, 11(2), 110–115. | ||
| In article | View Article PubMed | ||
| [18] | Zheng, X., Yu, L., Xu, Q., Gu, S., & Tang, L. (2018). Guillain-Barre syndrome caused by hepatitis E infection: case report and literature review. BMC infectious diseases, 18(1), 50. | ||
| In article | View Article PubMed | ||
| [19] | Al-Saffar, A., & Al-Fatly, B. (2018). Acute Motor Axonal Neuropathy in Association with Hepatitis E. Frontiers in neurology, 9, 62. | ||
| In article | View Article PubMed | ||
| [20] | Salim, O. J., Davidson, A., Li, K., Leach, J. P., & Heath, C. (2017). Brainstem encephalitis and acute polyneuropathy associated with hepatitis E infection. BMJ case reports, 2017, bcr2017220799. https: //pmc.ncbi.nlm.nih.gov/articles/PMC5623255/. | ||
| In article | View Article PubMed | ||
| [21] | Ji, S. B., Lee, S. S., Jung, H. C., Kim, H. J., Kim, H. J., Kim, T. H., Jung, W. T., Lee, O. J., & Song, D. H. (2016). A Korean patient with Guillain-Barré syndrome following acute hepatitis E whose cholestasis resolved with steroid therapy. Clinical and molecular hepatology, 22(3), 396–399. | ||
| In article | View Article PubMed | ||
| [22] | Bandyopadhyay, D., Ganesan, V., Choudhury, C., Kar, S. S., Karmakar, P., Choudhary, V., ... & Mukhopadhyay, S. (2015). Two uncommon causes of Guillain‐Barré syndrome: Hepatitis E and Japanese encephalitis. Case Reports in Neurological Medicine, 2015(1), 759495. | ||
| In article | View Article PubMed | ||
| [23] | Higuchi, M. A., Fukae, J., Tsugawa, J., Ouma, S., Takahashi, K., Mishiro, S., & Tsuboi, Y. (2015). Dysgeusia in a patient with Guillain-Barre syndrome associated with acute hepatitis E: a case report and literature review. Internal Medicine, 54(12), 1543-1546. | ||
| In article | View Article PubMed | ||
| [24] | Citation style for this article: Santos L, Mesquita J R, Rocha Pereira N, Lima-Alves C, Serrão R, Figueiredo P, Reis J, Simões J, Nascimento M S, Sarmento A. Acute hepatitis E complicated by Guillain-Barré syndrome in Portugal, December 2012 – a case report. Euro Surveill. 2013; 18(34): pii=20563. | ||
| In article | View Article PubMed | ||
| [25] | Kamar, N., Bendall, R. P., Peron, J. M., Cintas, P., Prudhomme, L., Mansuy, J. M., Rostaing, L., Keane, F., Ijaz, S., Izopet, J., & Dalton, H. R. (2011). Hepatitis E virus and neurologic disorders. Emerging infectious diseases, 17(2), 173–179. | ||
| In article | View Article PubMed | ||
| [26] | Loly, J. P., Rikir, E., Seivert, M., Legros, E., Defrance, P., Belaiche, J., ... & Delwaide, J. (2009). Guillain-Barre syndrome following hepatitis E. World journal of gastroenterology: WJG, 15(13), 1645. | ||
| In article | View Article PubMed | ||
| [27] | Khanam, R. A., Faruq, M. O., Basunia, R. A., & Ahsan, A. A. (2009). Guillain-Barré Syndrome Associated with Acute HEV Hepatitis. Ibrahim Medical College Journal, 2(1), 32–34. | ||
| In article | View Article | ||
| [28] | Rath, J., Zulehner, G., Schober, B., Grisold, A., Krenn, M., Cetin, H., & Zimprich, F. (2021). Cerebrospinal fluid analysis in Guillain-Barré syndrome: value of albumin quotients. Journal of neurology, 268(9), 3294–3300. | ||
| In article | View Article PubMed | ||
| [29] | Primadharsini PP, Nagashima S, Okamoto H. Genetic Variability and Evolution of Hepatitis E Virus. Viruses. 2019 May 18; 11(5): 456. | ||
| In article | View Article PubMed | ||
| [30] | Sidow NO, Hassan MS. Intravenous immunoglobulin treatment with prognosis for the first six months of Guillain-Barré Syndrome in Somalia: Case series. Ann Med Surg (Lond). 2022 Nov 5; 84: 104816. | ||
| In article | View Article | ||
| [31] | Lhomme S, Abravanel F, Cintas P, Izopet J. Hepatitis E Virus Infection: Neurological Manifestations and Pathophysiology. Pathogens. 2021 Dec 3; 10(12): 1582. | ||
| In article | View Article PubMed | ||
| [32] | Trojaborg, W. (1998). Acute and chronic neuropathies: new aspects of Guillain–Barré syndrome and chronic inflammatory demyelinating polyneuropathy, an overview and an update. Electroencephalography and clinical neurophysiology, 107(5), 303-316. | ||
| In article | View Article PubMed | ||
| [33] | Al-Hakem, H., Doets, A. Y., Stino, A. M., Zivkovic, S. A., Andersen, H., Willison, H. J., Cornblath, D. R., Gorson, K. C., Islam, Z., Mohammad, Q. D., Sindrup, S. H., Kusunoki, S., Davidson, A., Casasnovas, C., Bateman, K., Miller, J. A. L., van den Berg, B., Verboon, C., Roodbol, J., Leonhard, S. E., … IGOS Consortium (2023). CSF Findings in Relation to Clinical Characteristics, Subtype, and Disease Course in Patients with Guillain-Barré Syndrome. Neurology, 100(23), e2386–e2397. | ||
| In article | View Article PubMed | ||
| [34] | van Doorn, P. A., Van den Bergh, P. Y. K., Hadden, R. D. M., Avau, B., Vankrunkelsven, P., Attarian, S., Blomkwist-Markens, P. H., Cornblath, D. R., Goedee, H. S., Harbo, T., Jacobs, B. C., Kusunoki, S., Lehmann, H. C., Lewis, R. A., Lunn, M. P., Nobile-Orazio, E., Querol, L., Rajabally, Y. A., Umapathi, T., Topaloglu, H. A., … Willison, H. J. (2023). European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of Guillain-Barré syndrome. European journal of neurology, 30(12), 3646–3674. | ||
| In article | View Article PubMed | ||
| [35] | Songtanin B, Molehin AJ, Brittan K, Manatsathit W, Nugent K. Hepatitis E Virus Infections: Epidemiology, Genetic Diversity, and Clinical Considerations. Viruses. 2023 Jun 17; 15(6): 1389. | ||
| In article | View Article PubMed | ||
| [36] | Smith DB, Ijaz S, Tedder RS, Hogema B, Zaaijer HL, Izopet J, Bradley-Stewart A, Gunson R, Harvala H, Kokki I, Simmonds P. Variability and pathogenicity of hepatitis E virus genotype 3 variants. J Gen Virol. 2015 Nov; 96(11): 3255-3264. | ||
| In article | View Article PubMed | ||
| [37] | Liu, H., & Ma, Y. (2020). Hepatitis E virus-associated Guillain-Barre syndrome: Revision of the literature. Brain and behavior, 10(1), e01496. | ||
| In article | View Article PubMed | ||
| [38] | Lhomme, S., Abravanel, F., Cintas, P., & Izopet, J. (2021). Hepatitis E Virus Infection: Neurological Manifestations and Pathophysiology. Pathogens (Basel, Switzerland), 10(12), 1582. | ||
| In article | View Article PubMed | ||
| [39] | Drave, S. A., Debing, Y., Walter, S., Todt, D., Engelmann, M., Friesland, M., Wedemeyer, H., Neyts, J., Behrendt, P., & Steinmann, E. (2016). Extra-hepatic replication and infection of hepatitis E virus in neuronal-derived cells. Journal of viral hepatitis, 23(7), 512–521. | ||
| In article | View Article PubMed | ||
| [40] | Kamar N, Dalton HR, Abravanel F, et al. Hepatitis E virus infection. Clin Microbiol Rev. 2014; 27(1): 116-138. | ||
| In article | View Article PubMed | ||
| [41] | Naik GS, Meena AK, Reddy BAK, Mridula RK, Jabeen SA, Borgohain R. Anti-ganglioside antibodies profile in Guillain-Barré syndrome: Correlation with clinical features, electrophysiological pattern, and outcome. Neurol India. 2017 Sep-Oct; 65(5): 1001-1005. | ||
| In article | View Article PubMed | ||
| [42] | Yuki N. Guillain-Barré syndrome and anti-ganglioside antibodies: a clinician-scientist's journey. Proc Jpn Acad Ser B Phys Biol Sci. 2012; 88(7): 299-326. | ||
| In article | View Article PubMed | ||
| [43] | Bellanti R, Rinaldi S. Guillain-Barré syndrome: a comprehensive review. Eur J Neurol. 2024 Aug; 31(8): e16365. | ||
| In article | View Article PubMed | ||
| [44] | Willison HJ, Jacobs BC, van Doorn PA. Guillain‑Barré syndrome. Lancet. 2016; 388(10045): 717‑727. | ||
| In article | View Article PubMed | ||
| [45] | Islam Z, et al. Campylobacter jejuni infection and GBS in Bangladesh. Ann Neurol. 2010; 68(6): 961‑971. | ||
| In article | |||
| [46] | van den Berg B, Walgaard C, Drenthen J, et al. Guillain‑Barré syndrome: pathogenesis, diagnosis, treatment and prognosis. Nat Rev Neurol. 2014; 10(8): 469‑482. | ||
| In article | View Article PubMed | ||
| [47] | Dos Santos T, et al. Zika virus and GBS: case series from French Polynesia. Lancet. 2016; 387(10027): 1531‑1539. | ||
| In article | View Article PubMed | ||
| [48] | Kuwabara S, Yuki N. Axonal Guillain‑Barré syndrome: concepts and controversies. Lancet Neurol. 2013; 12(12): 1180‑1188. | ||
| In article | View Article PubMed | ||



{kind=link}
{kind=link}