Antimicrobial resistance (AMR) is both a natural evolutionary phenomenon and a modern public health crisis. Ancient microbial genomes reveal that resistance mechanisms long predate human medicine, underscoring the inevitability of microbial adaptation. However, contemporary human activities, including the widespread use of antibiotics in healthcare, agriculture, and industry, have dramatically accelerated the scale and impact of resistance. This editorial integrates genomic evidence from ancient isolates with current trends to highlight how human behavior amplifies an otherwise natural process into a global threat. By framing AMR as both historically rooted and socially driven, we emphasize the urgent need for coordinated stewardship, innovation in therapeutics, and global policy interventions to mitigate its escalating burden.
Antimicrobial resistance (AMR) is often portrayed as a modern crisis, a consequence of the antibiotic era that began with the discovery of penicillin in 1928. Yet recent findings challenge this narrative. The study of Psychrobacter SC65A.3, a strain isolated from the perennial ice block of Scarisoara Ice Cave, Romania, provides critical insights into the genetic reservoir of AMR and virulence determinants preserved in ancient cryoenvironments 1. Whole-genome sequencing revealed a complex repertoire of resistance genes, underscoring the evolutionary persistence of multidrug resistance (MDR) traits in extreme ecological niches. MDR is the ability of microorganisms (like bacteria) to resist multiple antimicrobial drugs. A total of 107 AMR-associated genes were identified, of which 44 were directly linked to the observed MDR phenotype. Among these, beta (β)-lactam resistance genes (ampC, ftsI, ampD, ampG) were prominent, conferring hydrolytic activity against penicillins and cephalosporins. Resistance to fluoroquinolones was mediated by mutations in gyrA, gyrB, parC, and parE, which encode deoxyribonucleic acid (DNA) gyrase and topoisomerase subunits. Efflux-mediated resistance was widespread, with genes such as mexA, mexB, oprM, emrK, mdtA, mdtK, macB, mepA, msbA, macA, bcr, and emrE, enabling broad-spectrum tolerance to aminoglycosides, tetracyclines, macrolides, and other drug classes. Additional resistance determinants included tetA and tetC (tetracycline efflux), rpoB (rifampin resistance), dfrA and folP (trimethoprim / sulfonamide resistance), and notably mcr1 (mobilized colistin resistance-1), which confers resistance to colistin, a last-resort antibiotic. Heavy metal resistance genes (arsA, arsB, arsC for arsenic; merA, merP, merR for mercury) further highlighted the strain’s adaptive potential in hostile environments.
Beyond resistance, the genome encoded a diverse set of virulence and antimicrobial activity genes, suggesting dual ecological roles as both competitor and survivor. Genes such as sunS (sublancin biosynthesis), pikAII (pikromycin), btrK (butirosin), rebO (rebeccamycin), dpgD (glycopeptide biosynthesis), bacC (bacitracin), bpoA2 (haloperoxidase), cetB (cetoniacytone A), rdmC (anthracycline tailoring enzyme), and sdhE (succinate dehydrogenase assembly factor) were identified, many of which are associated with the production of bioactive secondary metabolites. These genetic features were corroborated phenotypically: Psychrobacter SC65A.3 inhibited the growth of 14 clinically relevant pathogens, including methicillin-resistant Staphylococcus aureus (MRSA), Enterococcus faecium, Enterobacter, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Escherichia coli. Such activity underscores the strain’s potential as a source of novel antimicrobial compounds.
The genome of Psychrobacter SC65A.3 from cryoenvironments highlights the dual nature of microbial survival, encoding both MDR genes such as mcr1 and biosynthetic pathways for antimicrobial compounds. This demonstrates that AMR is an ancient evolutionary trait shaped by ecological competition, not a modern invention. However, the present global AMR crisis is largely humandriven, with excessive antibiotic use in medicine, agriculture, and industry intensifying selective pressures and escalating a natural process into a public health emergency. Cryoenvironments therefore act as reservoirs of both resistance genes and novel bioactive molecules, offering insights into resistance evolution and opportunities for drug discovery. While resistance is inevitable, its scale and impact are strongly influenced by human behavior 2, 3.
Microbial communities have long engaged in chemical competition, producing antimicrobials and evolving mechanisms to withstand them. This ancient "resistome", that refers to the entire collection of AMR genes present in microbial communities, including those expressed, silent, or latent, confirms that resistance is an inherent and enduring feature of microbial life, existing long before clinical antibiotic use 2. Despite its ancient origins, modern AMR is unprecedented in scale. Widespread and often inappropriate antibiotic use has accelerated the emergence and spread of resistant pathogens, including carbapenemresistant bacteria that pose serious threats in healthcare settings due to high mortality and limited treatment options 3, 4. Unlike slow natural evolution, modern practices expose microbes to intense and widespread antimicrobial pressure. The contrast between ancient and contemporary AMR underscores that resistance itself is unavoidable, but its amplification is not. In natural ecosystems, resistance was diffuse and ecologically balanced, whereas today it is concentrated, clinically significant, and rapidly disseminated through human activity. Misuse of antimicrobials, agricultural practices, global travel, and weak regulatory oversight have transformed resistance into a global health challenge 3, 5. As shown in Figure 1, the genomic analysis of Psychrobacter SC65A.3 reveals a diverse resistome comprising 107 AMR-associated genes. These include efflux pumps and β-lactamases, which are widespread across bacterial taxa, as well as the mcr1 gene, a determinant of colistin resistance that is of particular clinical concern. The spatial distribution and diversity of these genes emphasize that AMR is not a modern phenomenon but an ancient evolutionary trait. This figure visually reinforces the manuscript’s central argument: while resistance is inevitable, its amplification into a global crisis is driven by human activity.

This image has been created by the authors from references 2, 3, 4, 5.
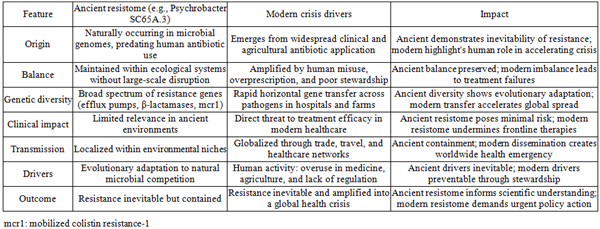
Table 1. expands the comparative framework by including the impact of ancient versus modern AMR. While ancient resistomes illustrate the inevitability of resistance as an evolutionary trait, modern drivers transform this inevitability into a global health crisis.
This table has been created by the authors from references 1, 2, 3, 4, 5.
Beyond clinical misuse, socioeconomic and behavioral factors play a pivotal role in accelerating AMR. In many community settings, antibiotics are frequently obtained without prescription, leading to inappropriate use for viral infections or incomplete treatment courses. This misuse fosters selective pressure that accelerates resistance development. Pharmaceutical industry practices, including aggressive marketing and insufficient investment in novel antimicrobials, further exacerbate the crisis. Additionally, disparities in healthcare access drive self-medication and reliance on informal drug markets, particularly in low- and middle-income countries (LMICs). Behavioral factors such as patient demand for antibiotics, physician overprescription to satisfy expectations, and lack of public awareness campaigns contribute to widespread misuse. Collectively, these socioeconomic and behavioral drivers transform a natural evolutionary phenomenon into a global public health emergency 6, 7, 8.
Effective regulatory oversight must be tailored to the realities of diverse healthcare systems and agricultural practices. In high-income countries, robust prescription monitoring, electronic health records, and centralized reporting can enforce stewardship programs. In contrast, LMICs often face challenges such as limited infrastructure, informal drug markets, and uneven access to healthcare. Here, scalable interventions, such as community-based education, stricter controls on over the counter (OTC) antibiotic sales, and partnerships with local health workers, are more feasible. In agriculture, oversight should balance productivity with public health by restricting non-therapeutic antibiotic use, incentivizing alternatives such as vaccines and probiotics, and ensuring compliance through transparent supply-chain audits. These efforts must be supported by robust international collaboration, encompassing surveillance, data sharing, and coordinated action plans that transcend national boundaries. Public awareness campaigns are vital to educate communities about responsible antibiotic use and the risks of misuse, thereby fostering behavioral change at the societal level. Finally, stronger regulatory oversight is required to enforce policies governing antibiotic distribution, sales, and industrial applications, ensuring that human activity does not continue to accelerate an otherwise inevitable biological process 9, 10, 11.
Looking ahead, the fight against AMR will increasingly rely on forwardthinking strategies that integrate technology, policy, and innovation. Artificial intelligence (AI) offers powerful tools for surveillance, enabling realtime analysis of resistance patterns and predictive modeling to guide interventions before crises emerge. Strengthened global cooperation frameworks are equally vital, ensuring that surveillance data, regulatory standards, and best practices are shared across borders to create a unified response. At the therapeutic level, investment in novel antimicrobials, vaccines, and alternative approaches such as bacteriophage therapy or microbiome modulation will be essential to outpace evolving pathogens. By embracing these futureoriented strategies, the global community can move beyond reactive measures and toward proactive, sustainable management of resistance 12.
In conclusion, AMR is not a modern anomaly but an intrinsic feature of microbial evolution. Genomic evidence from ancient isolates demonstrates that resistance mechanisms have existed for millennia, underscoring the inevitability of microbial adaptation. What transforms this natural process into a global health crisis, however, is the scale and intensity of human activity, particularly the misuse and overuse of antibiotics in medicine, agriculture, and industry. By accelerating the spread and persistence of resistant strains, human behavior has amplified a biological inevitability into a societal emergency. Addressing this challenge requires a dual recognition: resistance cannot be eradicated, but its impact can be mitigated. Coordinated stewardship, investment in novel therapeutics, and global policy frameworks are essential to slow the amplification of resistance and preserve the effectiveness of existing treatments. Ultimately, the crisis of AMR is not solely a scientific problem but a reflection of human choices, and its resolution depends on collective responsibility and sustained action.
| [1] | Paun VI, Itcus C, Lavin P, Chifiriuc MC and Purcarea C: First genome sequence and functional profiling of Psychrobacter SC65A.3 preserved in 5,000-year-old cave ice: insights into ancient resistome, antimicrobial potential, and enzymatic activities. Front Microbiol. 2026, 16:1713017. 10.3389/fmicb.2025.1713017. | ||
| In article | View Article PubMed | ||
| [2] | Davies J, Davies D: Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev. 2010, 74:417-33. 10.1128/mmbr.00016-10. | ||
| In article | View Article PubMed | ||
| [3] | Ventola CL: The antibiotic resistance crisis: part 1: causes and threats. P T. 2015, 40:277-283. | ||
| In article | |||
| [4] | Yuan P-B, Dai L-T, Zhang Q-K, Zhong Y-X, Liu W-T, Yang L, Chen D-Q: Global emergence of double and multi-carbapenemase producing organisms: epidemiology, clinical significance, and evolutionary benefits on antimicrobial resistance and virulence. Microbiol Spectr. 2024, 12:e0000824. 10.1128/spectrum.00008-24. | ||
| In article | View Article PubMed | ||
| [5] | Monitoring and evaluation of the global action plan on antimicrobial resistance. (2019). Accessed: March 10, 2026: https:// iris.who.int/ server/ api/core/bitstreams/c608fc14-d5a9-44f2-9537-4fdad60f9852/content. | ||
| In article | |||
| [6] | Nammi J, Pasala R, Andhe N, Vasam R, Poruri AD, Sherikar RR: Antibiotic misuse: an in-depth examination of Its global consequences and public health challenges. Cureus. 2025, 17:e85941. 10.7759/cureus.85941 | ||
| In article | View Article PubMed | ||
| [7] | Eke SM, Cua A: Invisible engines of resistance: how global inequities drive antimicrobial failure. Antibiotics (Basel). 2025, 14:659. 10.3390/antibiotics14070659. | ||
| In article | View Article PubMed | ||
| [8] | Nohri AR, Siddiqui MI, Usman G, Sarang S, Memon HQ, Singh D, Kumar S: Antibiotic dispensation without prescription by community pharmacies in Pakistan. J Med Surg Public Health. 2024, 2:100065. 10.1016/j.glmedi.2024.100065. | ||
| In article | View Article | ||
| [9] | Allel K, Labarca J, Carvajal C, et al.: Trends and socioeconomic, demographic, and environmental factors associated with antimicrobial resistance: a longitudinal analysis in 39 hospitals in Chile 2008-2017. Lancet Reg Health Am. 2023, 21:100484. 10.1016/j.lana.2023.100484. | ||
| In article | View Article PubMed | ||
| [10] | Pokharel S, Raut S, Adhikari B: Tackling antimicrobial resistance in low-income and middle-income countries. BMJ Glob Health. 2019, 4:e002104. 10.1136/bmjgh-2019-002104. | ||
| In article | View Article PubMed | ||
| [11] | Mukonzo JK, Ndagije HB, Sabblah GT, Mathenge W, Price DA, Grasela TH: Expanding regulatory science: Regulatory complementarity and reliance. Clin Transl Sci. 2024, 17:13683. 10.1111/cts.13683. | ||
| In article | View Article PubMed | ||
| [12] | Salama RA, Abdel Kader RG, Wadid NA: Artificial intelligence in combating challenges in antimicrobial resistance: a narrative review. Infect Prev Pract. 2026, 8:100522. 10.1016 / j.infpip.2026.100522. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2026 Venkataramana Kandi
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Paun VI, Itcus C, Lavin P, Chifiriuc MC and Purcarea C: First genome sequence and functional profiling of Psychrobacter SC65A.3 preserved in 5,000-year-old cave ice: insights into ancient resistome, antimicrobial potential, and enzymatic activities. Front Microbiol. 2026, 16:1713017. 10.3389/fmicb.2025.1713017. | ||
| In article | View Article PubMed | ||
| [2] | Davies J, Davies D: Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev. 2010, 74:417-33. 10.1128/mmbr.00016-10. | ||
| In article | View Article PubMed | ||
| [3] | Ventola CL: The antibiotic resistance crisis: part 1: causes and threats. P T. 2015, 40:277-283. | ||
| In article | |||
| [4] | Yuan P-B, Dai L-T, Zhang Q-K, Zhong Y-X, Liu W-T, Yang L, Chen D-Q: Global emergence of double and multi-carbapenemase producing organisms: epidemiology, clinical significance, and evolutionary benefits on antimicrobial resistance and virulence. Microbiol Spectr. 2024, 12:e0000824. 10.1128/spectrum.00008-24. | ||
| In article | View Article PubMed | ||
| [5] | Monitoring and evaluation of the global action plan on antimicrobial resistance. (2019). Accessed: March 10, 2026: https:// iris.who.int/ server/ api/core/bitstreams/c608fc14-d5a9-44f2-9537-4fdad60f9852/content. | ||
| In article | |||
| [6] | Nammi J, Pasala R, Andhe N, Vasam R, Poruri AD, Sherikar RR: Antibiotic misuse: an in-depth examination of Its global consequences and public health challenges. Cureus. 2025, 17:e85941. 10.7759/cureus.85941 | ||
| In article | View Article PubMed | ||
| [7] | Eke SM, Cua A: Invisible engines of resistance: how global inequities drive antimicrobial failure. Antibiotics (Basel). 2025, 14:659. 10.3390/antibiotics14070659. | ||
| In article | View Article PubMed | ||
| [8] | Nohri AR, Siddiqui MI, Usman G, Sarang S, Memon HQ, Singh D, Kumar S: Antibiotic dispensation without prescription by community pharmacies in Pakistan. J Med Surg Public Health. 2024, 2:100065. 10.1016/j.glmedi.2024.100065. | ||
| In article | View Article | ||
| [9] | Allel K, Labarca J, Carvajal C, et al.: Trends and socioeconomic, demographic, and environmental factors associated with antimicrobial resistance: a longitudinal analysis in 39 hospitals in Chile 2008-2017. Lancet Reg Health Am. 2023, 21:100484. 10.1016/j.lana.2023.100484. | ||
| In article | View Article PubMed | ||
| [10] | Pokharel S, Raut S, Adhikari B: Tackling antimicrobial resistance in low-income and middle-income countries. BMJ Glob Health. 2019, 4:e002104. 10.1136/bmjgh-2019-002104. | ||
| In article | View Article PubMed | ||
| [11] | Mukonzo JK, Ndagije HB, Sabblah GT, Mathenge W, Price DA, Grasela TH: Expanding regulatory science: Regulatory complementarity and reliance. Clin Transl Sci. 2024, 17:13683. 10.1111/cts.13683. | ||
| In article | View Article PubMed | ||
| [12] | Salama RA, Abdel Kader RG, Wadid NA: Artificial intelligence in combating challenges in antimicrobial resistance: a narrative review. Infect Prev Pract. 2026, 8:100522. 10.1016 / j.infpip.2026.100522. | ||
| In article | View Article PubMed | ||



{kind=link}