Vaccines against the Coronavirus Disease-19 (COVID-19) may be effective in reducing hospital stay rates, severe illnesses, and fatalities. Being hospitalized, prognostic variables and immunization effects on inflammatory indicators must be assessed. Our research evaluated whether vaccinations affect indicators of inflammation. In this cross-sectional study, 55 hospitalized COVID-19 patients were documented together with their demographics, comorbidities, and inflammatory markers from November 1, 2021, to December 31, 2021. The patients were divided into three groups according to their COVID-19 vaccination status: 28 were unvaccinated, 7 were partially vaccinated, and 20 individuals were fully vaccinated. Out of 55 participants, the mean age ( ± SD) was 59.8 ( ± 15.5) years and 56.4% of the total patients were females. 94.5% of the patients had comorbidity (78.2% diabetic, 74.5% hypertensive). A significantly higher (p = 0.03) number of patients with Diabetes Mellitus (DM) were unvaccinated. Among 55 patients, 24 were admitted to the ICU and 31 were in general beds that were isolated for COVID-19 patients. No significant association was found between the patient’s vaccination status and hospital admission site (p = 0.9). The median values of CRP, D-dimer & LDH were statistically significant among the groups (p < 0.05). The unvaccinated patient group had significantly higher CRP (p = 0.017) & LDH (p = 0.023) levels than the partially vaccinated group. Moreover, the D-dimer levels of unvaccinated patients were significantly higher than both the fully vaccinated (p = 0.024) as well as the partially vaccinated group (p = 0.035). No significant differences were observed in serum Ferritin levels among the groups (p = 0.34). Though COVID-19 immunization can’t remove the possibility of infection, it reduces illness severity and inflammatory responses, improving clinical outcomes and perhaps decreasing hospitalization and death.
The World Health Organization (WHO) declared Coronavirus Disease-19 (COVID-19), as a pandemic in March 2020, which led to global health emergencies and high fatalities in the twenty-first century. 1 To reduce the mortality, the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) vaccines were introduced and very swiftly authorized for use and commercialization. By March 2022, an estimated approximately 10 billion vaccination doses had been given globally, with 63.1% on at least one dosage coverage. 2 The Bangladeshi government first launched an immunization campaign in early, 2021 and gradually authorized the use of around seven types of vaccines in Bangladesh. 3
COVID-19 infection still affects persons who received the vaccine due to its very distinct host immune responses and uncertain effects on novel mutations, although the rate of hospital stays, death outcomes, and severe infections has been substantially lowered through immunization. 4
The geographical diversity of human responses and some environmental factors interrupt the assessment of the effectiveness of vaccines in preventing severe and critical illness, the requirement of hospitalization, and the impact of COVID-19 infection. 2 The WHO research found the inactivated coronavirus vaccine used in some countries like China, Brazil, Turkey, Chile and Indonesia etc was successful in reducing the hospitalization rate and preventing symptomatic disease, ranging from 84-50% to 100-85%. 5 Most of those studies have focused on the effectiveness of vaccination in preventing hospital stays and illness but evaluating the in-hospital laboratory data differences between vaccinated and unvaccinated patients, is also essential for infected patients. 2
The levels of many biomarkers such as C-reactive protein (CRP), Ferritin, Erythrocyte Sedimentation Rate (ESR), Acute Phase Proteins (APP) such as procalcitonin and lymphocyte, Lactate Dehydrogenase (LDH), D-dimer, and others are consistently higher in respiratory viral infections including COVID-19. 5. Acute-phase proteins serve as a valuable indicator for evaluating an individual's immune response.
Our study was carried out at one of the biggest tertiary care facilities in Bangladesh to evaluate the in-hospital differences between some clinical and laboratory parameters of patients, e.g- CRP, Ferritin, LDH, and D- dimer levels among vaccinated and unvaccinated COVID-19 patients as well as to evaluate the contribution of immunization in reducing infection severity.
This cross-sectional research was carried out at the tertiary care hospital, Bangladesh Institute of Research and Rehabilitation in Diabetes, Endocrine, and Metabolic Disorders (BIRDEM). The research comprised individuals aged 18 years and above who were admitted to the hospital and tested positive for SARS-CoV-2 using the reverse transcription polymerase chain reaction (RT-PCR) method on nasopharyngeal swabs in between the time period of 1st November, 2021, and 31st December 2021. During this time, 65 individuals were hospitalized with a confirmed infection of COVID-19. Following the exclusion of patients with incomplete data, a total of 55 confirmed cases who were admitted to both the Intensive Care Unit (ICU) and general wards that were isolated for COVID-19 patients were enrolled in the study.
Based on vaccination status, patients were classified into three groups: fully vaccinated, partially vaccinated, and unvaccinated. The patients were defined as "fully vaccinated" who became symptomatic 14 days after receiving the second dose of the vaccine. However, "partially vaccinated" patients were those who became symptomatic two weeks or more after the first dose or who did not receive the second dose. Patients who became symptomatic less than 2 weeks after receiving the second dose were also classified as partially vaccinated. "People unvaccinated" were defined as those who did not get any dose of vaccine. 5
After obtaining approval from the BIRDEM Academy's ethical review board, a pre-designed questionnaire was used to collect patient history, followed by informed written consent while ensuring confidentiality and anonymity. Medical records, including the patient’s demographic characteristics and laboratory data (CRP, Ferritin, LDH, D-dimer) were obtained from the hospital database. The above laboratory markers were measured in blood drawn at the time of hospital admission.
According to the study objectives, the statistical analysis was done by SPSS version 23 and Microsoft Excel was used to generate figures. A Chi-Square test was done to compare categorical variables among the groups. The results of the comparison of continuous variables (inflammatory markers) among these groups were analyzed by Kruskal-Wallis test. Results were interpreted based on p-values, a two-sided p-value of 0.05 was considered as statistically significant among the groups. Bonferroni Post-hoc pair-wise test were done to see the association between two groups, where p-values < 0.05 were considered significant.
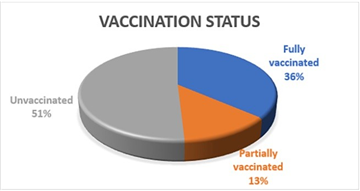
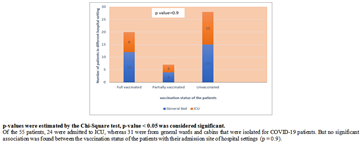
Out of 55 participants, the mean age ( ± SD) was 59.8 ( ± 15.5) years, and 56.4% of the patients were females. Approximately 94.5% of the patients had co-morbid illnesses, among them 78.2% were diabetic, and 74.5% were hypertensive. Of the 55 patients, 24 were admitted to ICU, whereas 31 were from general wards and cabins. Among 55 patients, 20 (36.4%) and 7 (12.7%) individuals were fully and partially vaccinated, respectively, with the highest being 28 (50.9%) of the unvaccinated individuals (Figure 2).
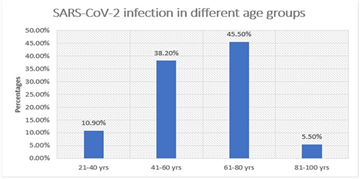
The presented study investigated the prevalence of SARS-CoV-2 infection in different age groups of patients. Notably, individuals aged 61-80 years and 41- 60 years exhibited the highest proportion of COVID-19 patients (Figure 1).
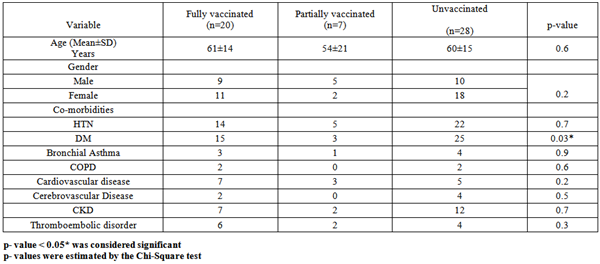
The Mean±SD age of the fully vaccinated COVID-19 patients was (61 ± 14) years, the unvaccinated group (60 ± 15) years and the partially vaccinated patients (54 ± 21) years. No significant association was found between the vaccination status of the patients with age (p = 0.6) as well as with sex (p = 0.2). A significantly higher number (p = 0.03*) of the patients with Diabetes Mellitus (DM) were unvaccinated as compared to partially and fully vaccinated individuals (Table 1).
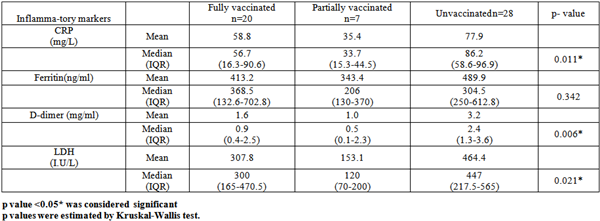
The mean and median values of CRP, D-dimer, & LDH levels were substantially higher in the unvaccinated group. Significant associations were found in the CRP (p = 0.011), D-dimer (p = 0.006) and LDH (p = 0.021) levels among the three groups. However, no significant differences were observed in the serum Ferritin level-based vaccination status (p = 0.342) (Table 2).


Box-plot represents significantly higher inflammatory markers- CRP, LDH & D-dimer levels in the unvaccinated group than the partially vaccinated group (Figure 4, Figure 5). The D-dimer level of the unvaccinated group was significantly higher than the fully vaccinated group also (Figure 5). Ferritin level was not significant in any group (Figure 4).
By rendering an immune system resistant to viruses, vaccines play a role as an immunomodulator in the pathogenesis of disease. The aim of a vaccine against any virus is to either reduce disease severity, eradicate it entirely, or decrease both morbidity and mortality. 2 The effect of vaccinations on laboratory tests such as CRP, D- dimer, Ferritin, and LDH, which are made at the onset of the disease, is mostly unknown. While assessing the severity of COVID-19 disease, the APPs—which represent the individual immune response—are crucial indicators as they indicate organ damage as well as the mortality of the patients. The evaluation of the functions of acute phase proteins like Ferritin, Erythrocyte sedimentation rate, Fibrinogen, D-dimer, and CRP should be done. 2, 7 Studying the frequency and impact of COVID-19 infection outbreaks in vaccinated individuals in Bangladesh is important, especially for those who need to be hospitalized.
The incidence of severe COVID-19 in this study was higher in middle-aged (41–60 y) and elderly (61–80 y) individuals, and this finding is similar to another study. 8 The body's immunological components gradually decline at this age 9, with fewer B and T cells overall than in younger individuals. Due to a combination of lowered immunity, ongoing antigen exposure, and elevated proinflammatory cytokines, older persons typically have low-level chronic inflammations.
In this study, comorbidities in the vaccinated group were not significantly different from the unvaccinated group except for Diabetes Mellitus (p = 0.03). The most important associated comorbidities in confirmed severe cases and mortality were similar to the national data as a whole (e.g., Diabetes Mellitus and Hypertension). 8 Type 2 diabetes and hypertension were the most common comorbidities among elderly patients with COVID-19 in a multicenter study from China. 10 A retrospective analysis of COVID-19 patients showed that the number of ACE-2 receptors in individuals with hypertension andtype 2 diabetes was higher than in individuals without hypertension and type 2 diabetes. A pro-inflammatory condition characterized by an excessive cytokine response to infection makes COVID-19 patients fall to a severe or even critical degree and may even cause death.
Only 8.1% of hospitalized COVID-19 patients had received all recommended vaccines, according to research on Israil by Haas et al. 11. This result was closer to a comparable study conducted in India by Sagiraju 12, which revealed only a 3% vaccination rate. Compared to this study's findings, these immunization rates were substantially lower. Among the hospitalized COVID-19 patients in this study, the complete vaccination rate was 36.4%. The results of another surveillance study of over 61,800 COVID-19 patients in Australia were 36.9% 8 and the results of Fatima et al. 2022 2 were 37.7%. These results were more similar to this one.
CRP level is used routinely as a marker in clinical practice to assess disease progression and response to treatment of both non-infectious and some infectious diseases. 13 A study by Liu et al. reported that COVID- 19 disease progressed severely in cases with a CRP > 41.8 mg/L. 14 Yormaz et al. emphasized that 67.47% of cases with COVID-19 disease had high CRP levels. 15 It is not clear how CRP levels develop in people with the disease, even if they are vaccinated. No significant difference in CRP levels was observed considering non- vaccinated, one-dose vaccinated, and two-dose vaccinated patients in a study. 8 CRP was higher in the unvaccinated group than in the vaccinated groups, and the differences were statistically significant (p < 0.05); this finding is similar to this study.
In COVID-19, D-dimer level is an excellent APP linked to inflammation and fibrin breakdown leading to activation of the fibrinolytic system and reflecting coagulation activity. 8, 16 It was found that the D-dimer level in COVID-19 illness was linked to inflammation in research by Yu et al. that compared the D-dimer level in bacterial pneumonia and COVID-19 pneumonia. 17 Higher D-dimer levels were positively correlated with death in COVID-19 cases, according to Tang et al. 18 In contrast to fully vaccinated COVID-19 patients, unvaccinated patients showed greater levels of D-dimer in some studies. 2, 5, 19 Özdemir et al. 5 found that unvaccinated COVID- 19 patients had D-dimer levels that were around two to 4.4 times higher than those of vaccinated patients. However, this study showed different results. This study found significantly higher D-dimer levels in unvaccinated COVID-19 patients than the fully vaccinated (p = 0.024) and partially vaccinated (p = 0.035) groups.
Lactate dehydrogenase (LDH) is an intracellular enzyme involved in anaerobic glycolysis that converts pyruvate to lactate. 20 Studies currently suggest that blood LDH levels are a non-specific indicator of cellular death in a variety of disorders, such as inflammation and cancer, and most of the information on the dynamic change in LDH in COVID-19 pneumonia is yet unclear. 21, 22 There was no appreciable difference in LDH levels based on vaccination status. 2, 7 The results of these investigations were different from the study by Al- Qahani, where a significant association was found. 19 In this study, significantly higher LDH levels were found than in the partially vaccinated group, who got a very recent vaccination dose.
Ferritin is another APP that may increase in response to viral infections and is commonly measured to detect iron deficiency anemia. 23 In some studies, ferritin level was a distinct predictor of COVID-19, ARDS, and mortality. [24] Ferritin levels in two-dose vaccinated patients were found to be significantly lower than those in one- dose vaccinated and unvaccinated patients. 5, 19 However, in this study, no noticeable differences were observed in the ferritin levels of COVID-19 patients based on immunization.
Our limitations were having a limited number of patients and evaluating the data retrospectively. The effect of different types of vaccines on laboratory figures could not be evaluated.
This research compares clinical and laboratory findings in Bangladeshi COVID-19 patients vaccinated and unvaccinated. Due to the data proving a reduction in multiple pro-inflammatory markers and hence potentially milder course of illness with immunization. Those patients had higher inflammatory markers (CRP, Ferritin, D-dimer, LDH levels), which indicated severe inflammatory response and worse outcomes than the unvaccinated group. Vaccination appears to mitigate the severity of COVID-19, leading to lower healthcare costs and better patient outcomes. Nonetheless, there have been some groups of people with other diseases who were found to respond relatively low to vaccination, and this underscores the importance of immunization in controlling the COVID-19 pandemic, reminding us of the necessity of public health efforts for increasing the vaccine’s coverage.
This research received no funding from external sources.
The authors thereby declare no conflict of interest exists.
We are very grateful to the Laboratory Director of the Immunology and Laboratory Medicine Department of BIRDEM General Hospital for providing access to the laboratory data of the hospitalized COVID-19 patients. We are also thankful to the laboratory staffs for their contribution in doing the laboratory tests efficiently.
Study Design: Ritu Saha, Hasiba Mahmuda, Shamoli Saha.
Data acquisition: Hasiba Mahmuda
Formal analysis: Hasiba Mahmuda, Shamoli Saha, Ritu Saha
Methodology: Hasiba Mahmuda
Supervision: Ritu Saha
Writing: original draft: Hasiba Mahmuda
Writing: review & editing: Ritu Saha, Shamoli Saha
| [1] | Islam MdR, Hasan M, Nasreen W, et al. The COVID-19 vaccination experience in Bangladesh: Findings from a cross- sectional study. Int J Immunopathol Pharmacol, 35. 1-13. December 2021. | ||
| In article | View Article PubMed | ||
| [2] | Fatima S, Zafar A, Afzal H, et al. COVID-19 infection among vaccinated and unvaccinated: Does it make any difference? PLOS ONE, 17(7). e0270485. July 2022. | ||
| In article | View Article PubMed | ||
| [3] | Amanatidou E, Gkiouliava A, Pella E, et al. Breakthrough infections after COVID-19 vaccination: Insights, perspectives and challenges. Metab Open, 14. 100180. June 2022. | ||
| In article | View Article PubMed | ||
| [4] | Mohsin M, Mahmud S, Uddin Mian A, et al. Side effects of COVID-19 vaccines and perceptions about COVID-19 and its vaccines in Bangladesh: A Cross-sectional study. Vaccine X, 12. 100207. December 2022. | ||
| In article | View Article PubMed | ||
| [5] | Özdemir B, Özdemir L, Akgunduz B. The Comparison of the Laboratory Parameters of Inactivated Coronavirus Vaccinated and Non-Vaccinated COVID-19 Patients Applied Hospital. Ank Med J, 23(3). 357–365. January 2023. | ||
| In article | View Article | ||
| [6] | Soleimanpour S, Yaghoubi A. COVID-19 vaccine: where are we now and where should we go? Expert Rev Vaccines, 20(1). 23–44. January 2021. | ||
| In article | View Article PubMed | ||
| [7] | Lee JE, Hwang M, Kim Y-H, et al. Imaging and Clinical Features of COVID-19 Breakthrough Infections: A Multicenter Study. Radiology 2022, 303(3). 682–692. June 2022. | ||
| In article | View Article PubMed | ||
| [8] | Pramana KA, Sudjud RW, Zulfariansyah A. Comparison of total lymphocytes, neutrophils to lymphocytes ratio, and C-reactive protein in vaccinated and non-vaccinated severe COVID-19 patients. Anaesth Pain Intensive Care, 26(5). 656–662. October 2022. | ||
| In article | View Article | ||
| [9] | Diao B, Wang C, Tan Y, et al. Reduction and functional exhaustion of T cells in patients with coronavirus disease 2019 (COVID-19). Front Immunol, 11. 827. May 2022. | ||
| In article | View Article PubMed | ||
| [10] | Haas EJ, Angulo FJ, McLaughlin JM, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. The Lancet, 397(10287). 1819–1829. May 2021. | ||
| In article | |||
| [11] | Sagiraju HKR, Elavarasi A, Gupta N, et al. The Effectiveness of SARS-CoV-2 Vaccination in Preventing Severe Illness and Death – Real-world Data from a Cohort of Patients Hospitalized with COVID-19. Indian J Community Med, 47(4). 510. October- December 2022. | ||
| In article | |||
| [12] | Del Valle DM, Kim-Schulze S, Huang H-H, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med, 26. 1636–1643. August 2020. | ||
| In article | |||
| [13] | Liu F, Li L, Xu M, et al. Prognostic value of interleukin-6, C- reactive protein, and procalcitonin in patients with COVID-19. J Clin Virol, 127.104370. June 2020. | ||
| In article | |||
| [14] | Yormaz B, Ergun D, Tulek B, et al. The evaluation of prognostic value of acute phase reactants in the COVID-19. Bratisl Lek Listy, 121. 628–633. Jan.2020. | ||
| In article | View Article PubMed | ||
| [15] | Sathe PM, Patwa UD. D Dimer in acute care. Int J Crit Illn Inj Sci, 4(3). 229–232. July-September 2014. | ||
| In article | View Article PubMed | ||
| [16] | Yu B, Li X, Chen J, et al. Evaluation of variation in D-dimer levels among COVID-19 and bacterial pneumonia: a retrospective analysis. J Thromb Thrombolysis, 50(3). 548–557. January 2020. | ||
| In article | View Article PubMed | ||
| [17] | Tang N, Bai H, Chen X, et al. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost, 18(5): 1094– 1099. May 2020. | ||
| In article | View Article PubMed | ||
| [18] | AlQahtani SY, Alabdulqader AA, Mashhour WAA, et al. Clinical Characteristics and Outcomes of Vaccinated VS Non-Vaccinated Critically Ill COVID-19 Patients: Retrospective Observation Study. Infect Drug Resist, 16. 3329–3338. December 2023. | ||
| In article | View Article PubMed | ||
| [19] | Rogatzki MJ, Ferguson BS, Goodwin ML, et al. Lactate is always the end product of glycolysis. Front Neurosci, 9. 3338. February 2015. | ||
| In article | View Article PubMed | ||
| [20] | Wu M-Y, Lu J-H. Autophagy and Macrophage Functions: Inflammatory Response and Phagocytosis. Cells, 9(1). 70. January 2020. | ||
| In article | View Article PubMed | ||
| [21] | Van Wilpe S, Koornstra R, Den Brok M, et al. Lactate dehydrogenase: a marker of diminished antitumor immunity. OncoImmunology, 9(1). 1731942. January 2020. | ||
| In article | View Article PubMed | ||
| [22] | Branco RG, Garcia PCR. Ferritin and C-Reactive Protein as Markers of Systemic Inflammation in Sepsis*. Pediatr Crit Care Med 2017, 18(2). 194. February 2017. | ||
| In article | View Article PubMed | ||
| [23] | Tan C, Huang Y, Shi F, et al. C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. J Med Virol, 92(7). 856–862. July 2020. | ||
| In article | View Article PubMed | ||
| [24] | Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med, 8(5). 475–481. January 2020. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2024 Hasiba Mahmuda, Shamoli Saha and Ritu Saha
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Islam MdR, Hasan M, Nasreen W, et al. The COVID-19 vaccination experience in Bangladesh: Findings from a cross- sectional study. Int J Immunopathol Pharmacol, 35. 1-13. December 2021. | ||
| In article | View Article PubMed | ||
| [2] | Fatima S, Zafar A, Afzal H, et al. COVID-19 infection among vaccinated and unvaccinated: Does it make any difference? PLOS ONE, 17(7). e0270485. July 2022. | ||
| In article | View Article PubMed | ||
| [3] | Amanatidou E, Gkiouliava A, Pella E, et al. Breakthrough infections after COVID-19 vaccination: Insights, perspectives and challenges. Metab Open, 14. 100180. June 2022. | ||
| In article | View Article PubMed | ||
| [4] | Mohsin M, Mahmud S, Uddin Mian A, et al. Side effects of COVID-19 vaccines and perceptions about COVID-19 and its vaccines in Bangladesh: A Cross-sectional study. Vaccine X, 12. 100207. December 2022. | ||
| In article | View Article PubMed | ||
| [5] | Özdemir B, Özdemir L, Akgunduz B. The Comparison of the Laboratory Parameters of Inactivated Coronavirus Vaccinated and Non-Vaccinated COVID-19 Patients Applied Hospital. Ank Med J, 23(3). 357–365. January 2023. | ||
| In article | View Article | ||
| [6] | Soleimanpour S, Yaghoubi A. COVID-19 vaccine: where are we now and where should we go? Expert Rev Vaccines, 20(1). 23–44. January 2021. | ||
| In article | View Article PubMed | ||
| [7] | Lee JE, Hwang M, Kim Y-H, et al. Imaging and Clinical Features of COVID-19 Breakthrough Infections: A Multicenter Study. Radiology 2022, 303(3). 682–692. June 2022. | ||
| In article | View Article PubMed | ||
| [8] | Pramana KA, Sudjud RW, Zulfariansyah A. Comparison of total lymphocytes, neutrophils to lymphocytes ratio, and C-reactive protein in vaccinated and non-vaccinated severe COVID-19 patients. Anaesth Pain Intensive Care, 26(5). 656–662. October 2022. | ||
| In article | View Article | ||
| [9] | Diao B, Wang C, Tan Y, et al. Reduction and functional exhaustion of T cells in patients with coronavirus disease 2019 (COVID-19). Front Immunol, 11. 827. May 2022. | ||
| In article | View Article PubMed | ||
| [10] | Haas EJ, Angulo FJ, McLaughlin JM, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. The Lancet, 397(10287). 1819–1829. May 2021. | ||
| In article | |||
| [11] | Sagiraju HKR, Elavarasi A, Gupta N, et al. The Effectiveness of SARS-CoV-2 Vaccination in Preventing Severe Illness and Death – Real-world Data from a Cohort of Patients Hospitalized with COVID-19. Indian J Community Med, 47(4). 510. October- December 2022. | ||
| In article | |||
| [12] | Del Valle DM, Kim-Schulze S, Huang H-H, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med, 26. 1636–1643. August 2020. | ||
| In article | |||
| [13] | Liu F, Li L, Xu M, et al. Prognostic value of interleukin-6, C- reactive protein, and procalcitonin in patients with COVID-19. J Clin Virol, 127.104370. June 2020. | ||
| In article | |||
| [14] | Yormaz B, Ergun D, Tulek B, et al. The evaluation of prognostic value of acute phase reactants in the COVID-19. Bratisl Lek Listy, 121. 628–633. Jan.2020. | ||
| In article | View Article PubMed | ||
| [15] | Sathe PM, Patwa UD. D Dimer in acute care. Int J Crit Illn Inj Sci, 4(3). 229–232. July-September 2014. | ||
| In article | View Article PubMed | ||
| [16] | Yu B, Li X, Chen J, et al. Evaluation of variation in D-dimer levels among COVID-19 and bacterial pneumonia: a retrospective analysis. J Thromb Thrombolysis, 50(3). 548–557. January 2020. | ||
| In article | View Article PubMed | ||
| [17] | Tang N, Bai H, Chen X, et al. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost, 18(5): 1094– 1099. May 2020. | ||
| In article | View Article PubMed | ||
| [18] | AlQahtani SY, Alabdulqader AA, Mashhour WAA, et al. Clinical Characteristics and Outcomes of Vaccinated VS Non-Vaccinated Critically Ill COVID-19 Patients: Retrospective Observation Study. Infect Drug Resist, 16. 3329–3338. December 2023. | ||
| In article | View Article PubMed | ||
| [19] | Rogatzki MJ, Ferguson BS, Goodwin ML, et al. Lactate is always the end product of glycolysis. Front Neurosci, 9. 3338. February 2015. | ||
| In article | View Article PubMed | ||
| [20] | Wu M-Y, Lu J-H. Autophagy and Macrophage Functions: Inflammatory Response and Phagocytosis. Cells, 9(1). 70. January 2020. | ||
| In article | View Article PubMed | ||
| [21] | Van Wilpe S, Koornstra R, Den Brok M, et al. Lactate dehydrogenase: a marker of diminished antitumor immunity. OncoImmunology, 9(1). 1731942. January 2020. | ||
| In article | View Article PubMed | ||
| [22] | Branco RG, Garcia PCR. Ferritin and C-Reactive Protein as Markers of Systemic Inflammation in Sepsis*. Pediatr Crit Care Med 2017, 18(2). 194. February 2017. | ||
| In article | View Article PubMed | ||
| [23] | Tan C, Huang Y, Shi F, et al. C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. J Med Virol, 92(7). 856–862. July 2020. | ||
| In article | View Article PubMed | ||
| [24] | Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med, 8(5). 475–481. January 2020. | ||
| In article | View Article PubMed | ||



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}