Annually, diarrhea causes approximately 1.6 million deaths worldwide, predominantly in Sub-Saharan Africa. In Kenya, diarrheal diseases are among the leading causes of morbidity and mortality, particularly affecting children under five. Despite various studies and interventions on diarrhea, the overall prevalence, distribution, pathogens and risk factors for diarrhea in Kenya remain inadequately investigated especially for atypical pathogens and adults. This scoping review aimed to synthesize available evidence on the prevalence, etiology, treatment, and risk factors associated with diarrheal diseases in Kenya across all age groups. The review followed Arksey and O'Malley’s framework and the Preferred Reporting Items for systematic review and Meta-analysis -scoping review guidelines. Comprehensive searches of databases such as MEDLINE and EMBASE, were conducted to identify studies for inclusion using the following criteria: all observational studies conducted in Kenya, reported in English, without restriction on publication year. Exclusion criteria included randomized control trials and reviews. A total of 210 studies were included in the study, covering diverse regions and study settings in Kenya. The studies primarily focused on children under five but also included adult populations. The pooled prevalence of diarrheal diseases varies significantly across different Kenyan regions. The Eastern region showed the highest prevalence at 20.79%, followed by Nairobi with 16%. The Northeastern region had the lowest prevalence at 3.44%. The most common bacterial causes were Escherichia coli, Salmonella, and Shigella, while Rotavirus was the predominant viral cause. Socioeconomic factors, hygiene practices, and environmental conditions were the major risk factors. The review highlighted a high prevalence of antibiotic resistance, with notable resistance to ampicillin, tetracycline, and trimethoprim/sulfamethoxazole. Several studies reported multidrug-resistant E. coli strains, with 27% being Enteroaggregative E. coli (EAEC) and 50% Enterotoxigenic E. coli (ETEC) isolates producing extended spectrum beta-lactamases. Diarrheal diseases in Kenya exhibit significant regional and demographic variability in prevalence and etiology. Major risk factors include poor hygiene, low socioeconomic status, and inadequate sanitation. The rise of multidrug-resistant Extended spectrum β-lactamase producing E. coli strain, poses a significant public health challenge, complicating treatment options. The widespread antibiotic resistance underscores the need for region-specific public health interventions and improved antibiotic stewardship. Further action is necessary to address national gaps in adult population data and to improve strategies for diarrhea diagnosis, prevention and management in Kenya.
It is estimated that by 2030, 4.4 million children 0-59 months of age will die from infectious diseases annually and 60% of those deaths will occur in Sub-Saharan Africa unless the appropriate mitigation measure is taken 1. Acute diarrhea defined is the passage of three or more loose or liquid stools per day (or more frequent passage than is normal for the individual) over a period of 14 days or less 2, is caused by mixed etiologies and contributes a significant proportion to that mortality. Globally, the burden of diarrheal disease across all age groups remains high, with approximately 1.6 million deaths annually and the highest-burden reported in Sub-Saharan Africa 3. According to the World Health Organization (WHO), diarrheal disease is still one of the major causes of death among children 0-59 months of age worldwide, contributing to about 525,000 deaths every year 2. Although mortality rates among adults are lower than those observed in children 0-59 months of age, diarrhea still poses a substantial burden to adults 4.
In Kenya, diarrheal diseases are ranked among the top ten causes of morbidity and mortality 5, which according to WHO data (WHO, 2020), caused about 15,420 of total deaths in Kenya in the year 2019. Known risk factors associated with diarrheal diseases are socio-economic status, type of latrine used, presence of flies, garbage, open defecation, age when the child starts using the latrine, disposal of the child’s feces and can be spread through water, flies, food, and improper washing of the hands 6. Known causes of diarrheal diseases in Kenya are viral, parasitic, and bacterial in nature 7. Despite several interventions, innovations and guidelines deployed to prevent and manage diarrheal diseases 8 mortality related to diarrhea still remains a major concern in Kenya.
In Kenya, several studies have been conducted to estimate the distribution, prevalence, treatment and factors associated to diarrheal diseases 4. However, these studies vary widely in prevalence levels and some regions in Kenya are underrepresented limiting the generalizability of outcomes. Without a clear understanding of the prevalence, etiology, treatment and risk factors associated with diarrheal diseases, it is challenging to implement targeted and relevant interventions. A comprehensive review of existing data would begin to provide this information yet no current or in-progress scoping reviews on diarrheal diseases in Kenya were identified in PROSPERO, MEDLINE, the Cochrane Database of Systematic Reviews, and JBI Evidence Synthesis. Therefore, this scoping review aimed to determine the pooled prevalence, causes, treatment and risk factors and interventions associated with diarrheal diseases among all age groups using available evidence in Kenya.
Review question
What is the prevalence, etiology, distribution, risk factors, intervention and treatment of diarrheal infections across all ages in Kenya?
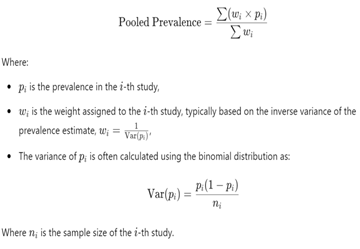
This scoping review was conducted according to the framework outlined by Arksey and O'Malley 9, and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) 10. A systematic approach was used to map existing literature and identification of evidence sources available. The steps entailed: identifying the research question, identifying relevant studies, study screening, collating, summarizing, and reporting of results, and consultation with stakeholders to inform and validate study findings. The study focused on published and unpublished (preprints) research conducted in Kenya, written in English and included all age groups. Observational study designs were such as cross-sectional, case-control, and cohort studies were included. However, randomized control studies, quasi-experimental studies, systematic reviews, and scoping reviews were not included. There were no limitations on the publication year of the articles. The pooled prevalence was calculated as per the formula by DerSimonian and Laird (1986) 11.
|
Search strategy
The search strategy aimed to locate both published and unpublished primary studies, grey literature, and text and opinion papers in Kenya to identify studies reporting prevalence, causes, treatment and risk factors of diarrheal disease in all age groups. An initial limited search of MEDLINE (PubMed) and Cumulative Index to Nursing and Allied Health Literature (CINAHL) was undertaken to identify articles on the topic. The text words contained in the titles and abstracts of relevant articles, and the index terms used to describe the articles were used to develop a full search strategy. To identify eligible studies, a comprehensive literature search with no date limits was conducted in MEDLINE/PubMed, EMBASE, Web of Science, CINAHL, Science Direct, Google Scholar and Cochrane Library and medRxiv pre-prints. All the literature search terms were restricted to English language. Eligible studies were extracted using google forms. The Covidence software (Covidence, Veritas Health Innovation, Melbourne, Australia) was used to manage the screening, data extraction, and quality assessment processes.
The search terms were: “prevalence”, “diarrhea”, “diarrheal”, “under-five”, “children”, “adults” “causes”, “associated factors” and “Kenya”.
Source of evidence selection
Following the search, all identified records were collated and uploaded into Zotero software [12) to manage citation and remove duplicates. The titles and abstracts were screened by 2 independent reviewers to ensure that all inclusion criteria were met. Full-text studies that did not meet the inclusion criteria were excluded, and reasons for their exclusion are provided in Figure 1. Any disagreements that arose between the reviewers were resolved by a third reviewer. The remaining papers were retrieved in full and their citation details imported into the Covidence software for unified management, assessment and review of the records.
Data extraction
After full text review, data were extracted independently by two reviewers using a standardized data abstraction format, adapted from the preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) guidelines 10. In case of discrepancies during the data extraction, a third reviewer was used to provide additional information or clarifications. For the first objective (prevalence), the data extraction format included primary author, publication year, region(s) within the country where the study was conducted, sample size, age categories: 0-59 months, and ≥ 5 years of age, study area, response rate, prevalence with 95% Confidence Interval. For the second objective (causes), data was extracted in a format of frequency and percentages with a specific causal agent. For the third objective (risk factors), data was extracted using the Supporting the Use of Research Evidence (SURE) framework 13.
Data analysis and presentation
The results are presented in a descriptive narrative format focusing on emerging themes from the extracted data. These themes include analysis of prevalence and distribution of diarrheal disease and the burden stratified into distinct age; causes, treatment and risk factors associated with diarrheal disease. The scoping review followed the format of PRISMA-ScR checklist 14 and data analysis for prevalence was done using pooled prevalence 15. Graphs and tables were generated in Microsoft Excel.
Limitations
As the objective of the scoping review was to map existing literature and synthesize available evidence on the prevalence, etiology, treatment, and risk factors associated with diarrheal diseases in Kenya across all age groups however, heterogeneity, methodological quality or bias risk of included articles was not assessed.
Ethical considerations
Ethics approval was not required for this scoping review of existing and publicly available literature.
This scoping review examined a total of 210 studies after applying the inclusion and exclusion criteria as summarized in Figure 1. The studies were conducted in various regions within Kenya, encompassing different study designs. The included studies were comprised of 125 cross-sectional studies, 31 interventional, 27 case-control, 14 cohorts, and 8 longitudinal studies. The studies collectively investigated various aspects of diarrhea, including the prevalence, etiology, associated risk factors, interventions, and antibiotic susceptibility patterns.
Study settings and population
The studies collected data from both hospitals and community settings across diverse settings: 30% in rural areas, 29% in urban settings, and 19% in mixed urban and rural settings. Notably, 22% of the studies lacked clear specification of the study setting. Geographically, the studies covered extensive an extensive area across Kenya, including Western, Luo Nyanza, Kisii, Central, Coastal, North-Eastern, Eastern, Rift valley and the Nairobi Metropolitan regions. Most studies were carried out in the Nairobi Metropolitan region (66, 31.4%), followed by the Luo Nyanza region (59, 28.1%).
The review of 210 studies revealed a significant focus on children, especially those under 5 years. Specifically, 142 (67.6%) studies focused on children, 17 studies targeted the adult population, while 51 studies examined both adults and children. The study encompassed a total of 2,772,162 participants, among whom 2,265,424 were confirmed cases of diarrhea.
Study settings and population
The studies collected data from both hospitals and community settings across diverse settings: 30% in rural areas, 29% in urban settings, and 19% in mixed urban and rural settings. Notably, 22% of the studies lacked clear specification of the study setting. Geographically, the studies covered extensive an extensive area across Kenya, including Western, Luo Nyanza, Kisii, Central, Coastal, North-Eastern, Eastern, Rift valley and the Nairobi Metropolitan regions. Most studies were carried out in the Nairobi Metropolitan region (66, 31.4%), followed by the Luo Nyanza region (59, 28.1%).
The review of 210 studies revealed a significant focus on children, especially those under 5 years. Specifically, 142 (67.6%) studies focused on children, 17 studies targeted the adult population, while 51 studies examined both adults and children. The study encompassed a total of 2,772,162 participants, among whom 2,265,424 were confirmed cases of diarrhea

Diarrheal etiology
Among the bacterial causes of diarrhea, Escherichia coli, Salmonella enterica, and Shigella spp. emerged as the most reported diarrheal agents, appearing in 125, 65, and 47 studies respectively to synthesize available evidence on the prevalence, etiology, treatment, and risk factors associated with diarrheal diseases in Kenya across all age groups.
s shown in Figure 2. Vibrio cholerae was the focus of investigation in 29 research papers while Clostridium difficile was studied in 3 research papers. Viral etiologies were represented in 29 studies with Rotavirus reported in 48, Norovirus in 19 studies, and Adenovirus in 15 studies as the most frequent causes of viral diarrhea (Figure 3). The main parasites associated with diarrhea were Giardia spp., Cryptosporidium spp., and Entamoeba spp. appearing in 34, 21, and 18 studies respectively Figure 4. Other less prevalent causes of diarrheal diseases were Vibrio fluvialis, Plesiomonas shigelloides, Hymenolepsis nana, Aeromonas spp., Providencia alcalifaciens, B. hominis, Campylobacter jejuni, and Campylobacter coli.



Prevalence and distribution of diarrhea
The pooled prevalence of diarrheal diseases varies significantly across different regions as shown in Figure 5. The Eastern region and Nairobi metropolitan area had the highest prevalence at 20.79% and 16% respectively, indicating a major health concern in those regions. Rift Valley and Coastal regions had moderate prevalence of 13.3% and 11.36% while Central and Western regions had comparable prevalence rates of 9.65% and 9.2%, respectively. Luo Nyanza and Kisii had slightly lower prevalence rates at 8.7% and 7.4%. In stark contrast, the Northeastern region had the lowest prevalence at 3.44%.
Significant variations in the occurrence of enteric pathogens were observed in the pooled prevalence 11 and distribution of diarrheal cases throughout different regions. E. coli and Rotavirus had the highest prevalence in the Central region, specifically in the counties of Murang'a and Kiambu, at 29.83% and 29.52%, respectively. Salmonella spp. (4.25%), Shigella spp. (4.44%), Aeromonas spp. (4.37%), Yersinia spp. (1.09%), Vibrio (0.55%), and Providencia (3.18%) had lower prevalence. Within the central region, no studies were reported from the counties of Kirinyaga, Nyandarua, and Nyeri.

In the Coast region, encompassing Kilifi, Kwale, and Mombasa counties, the highest prevalence was observed for E. coli (at 13.71%), followed by Cryptosporidium (21.67%), Salmonella (7.37%) and Shigella (6.49%). Other pathogens like Giardia lamblia (4.93%), Campylobacter spp. (4.91%), Rotavirus (16.20%), and Non-Typhoidal Salmonella (NTS) (15.56%) were also reported. No data was available for Tana River and Taita Taveta counties.
Marsabit and Meru counties had an overall pooled prevalence of approximately 20.79% for diarrheal pathogens. In the Nairobi metropolitan region, the pooled prevalence suggested overlapping cases due to multiple infections, resulting in a cumulative prevalence exceeding 100%. Assuming independence, the average prevalence per pathogen was estimated at 11.55%. In the Rift Valley, studies from Nandi, Kericho, and Turkana reported a pooled prevalence ranging between 2.1% and 20% for Salmonella, Shigella, Campylobacter, Rotavirus, and Giardia. The Northeastern Region, covering Garissa and Mandera counties, had an overall average prevalence of 3.44% for V. cholerae and E. coli.
Within the Luo Nyanza region, in the Lake Victoria region, specifically Kisumu, Siaya, and Homa Bay, E. coli had a prevalence of 16.78%, followed by Giardia (22.57%), Campylobacter (14.48%), Cryptosporidium (9.22%), Shigella (5.25%), Salmonella (3.08%), Rotavirus (13.32%), and NTS (4.00%). In the neighboring counties of Migori, Kisii, and Nyamira, E. coli prevalence was 14.69%, with Giardia at 10.50%, Campylobacter at 6.29%, with lower rates observed for other pathogens such as Cryptosporidium (3.80%) and Salmonella (1.20%). The Luo Nyanza region reported pooled prevalence for various enteroviruses, including Norovirus (13.9%), Sapovirus (10%). Adenovirus (9.1%), and Astrovirus (3.9%). In the Western region, covering Bungoma, Vihiga, Kakamega, and Busia counties, the pooled prevalence was highest for Giardia duodenalis (12.36%), followed by soil-transmitted helminths (9.06%), A. lumbricoides (3.86%), E. coli (3.07%), Salmonella (1.99%), Shigella (0.61%), and Vibrio species (0.15%). The distribution underscores the significant regional and county variations in the prevalence of diarrheal pathogens across different counties, highlighting the need for targeted region- and county- specific public health interventions.
Risk factors for diarrhea
Several studies reported multifaceted risk factors contributing to the prevalence of diarrhea, focusing on socioeconomic factors, immunocompromised states, age-related factors, hygiene practices, environmental risks, malnutrition, gender, occupation, and seasonality.
Poverty and lack of education were associated with a high incidence of diarrhea. In a study done in Nairobi 5, infants living in households with a pit latrine and in crowded households had almost 1.5 times higher risk of diarrhea than infants with a flush toilet or non-crowded households 6. Low-income households had a prevalence of 52.3% as compared to high income households which had 27.6% prevalence of diarrhea according to a study done in Kisumu 16.
On hygiene practices, several studies reported poor hand washing, poor personal hygiene, food hygiene and cleanliness of the household surrounding to be associated with acquisition of diarrhea 1, 7, 17. Drinking water from natural sources predisposes one to a higher risk of getting diarrhea compared to drinking water from taps and wells 3, 6. Open defecation and lack of proper sanitation was also associated with high incidences of diarrhea 7. A number of studies reported that diarrhea was more prevalent in children aged five years and below compared to older age groups 5, 7.
Diarrhea Interventions, antibiotic use and antibiotic resistance
As reported by these studies, a number of medical interventions exist for the management of diarrheal diseases in Kenya. These interventions are administered according to the WHO guidelines for the prevention, management and treatment of diarrhea. Zinc supplementation, recommended by the WHO as part of the standard treatment for acute diarrhea in children, was reported to significantly reduce diarrhea-related mortality.
Oral Rehydration Therapy which is used to replenish fluid and electrolytes lost during a diarrheal episode was found to be effective in managing diarrhea caused by Vibrio cholerae and Enteropathogenic E. coli. Rotarix, a monovalent rotavirus vaccine that was introduced in Kenya in the year 2014 is administered as a 2-dose vaccine at 6 weeks and 10 weeks of age, was reported to have reduced the prevalence of rotavirus by 10.5% at the coastal region since the introduction of this vaccine.
Antibiotics usage are reserved for cases where bacterial pathogens are identified 18. The literature in this scoping review revealed a significant pattern of antibiotic utilization. Ampicillin, Tetracycline, Chloramphenicol, Ceftriaxone and Gentamicin were the most reported antibiotics used for treatment of diarrhea related illness followed by Clotrimazole, Erythromycin, Streptomycin, cefuroxime among others.
This review identified notable disparities in antimicrobial resistance patterns across various geographical regions and pathogens. Antibiotic resistance rates for ampicillin ranged from 42% to 100%, tetracycline from 50% to 92%, and trimethoprim/sulfamethoxazole from 83% to 100% for different organisms and locations. Antibiotics like ciprofloxacin exhibited variable susceptibility profiles between bacterial pathogens; 42% of enteroaggregative E. coli (EAEC) and 8% of Shigella isolates. Apart from individual antibiotic resistance, the reported multi drug-resistant strains was alarming, with 33.9% of bacterial isolates displaying resistance to multiple antibiotics. E. coli had notably high extended-spectrum beta-lactamase (ESBL)-producing isolates among enteroaggregative E. coli (EAEC) (27%) and enterotoxigenic E. coli (ETEC) (50%) isolates. Three papers reported on C.difficile, two in Nairobi and one in Coastal Kenya. The prevalence in Nairobi was ~25% while in Southern Coastal Kenya, the prevalence reported was 35% with resistance levels reported for rifampicin (91.5%), erythromycin (88.7%), metronidazole (85%), ciprofloxacin (83.1%), and clindamycin (8%).
Study sources
This scoping review was conducted to fill gaps in the understanding of the overall prevalence, diarrheal disease etiologies and distribution across Kenya in all ages. The review extracted data from 210 published and unpublished reports. Approximately 2/3 of the studies focused on pediatric populations, especially children under five years old, 8% focused solely on adults, and 24% included both age groups. This indicates a significant emphasis on researching diarrheal diseases in young children, highlighting their vulnerability to diarrhea. However, there is a notable lack of research on adult populations, pointing to a need for more inclusive studies to better understand the epidemiology of diarrhea across all age groups 2. This Scoping review brings together results from different study designs giving a broad perspective on the prevalence of diarrheal diseases. It includes 125 cross-sectional studies, which collects information at a specific point in time, and 8 longitudinal studies, which in contrast to the cross-sectional studies follow individuals over a period of time 19, 20, 21, 22. Furthermore, 27 case-control studies were included to determine if an exposure is associated with an outcome by comparing cases (individuals with the outcome) and controls (those without the outcome) 21. We also examined 14 cohort studies which assess associations between multiple exposures and multiple outcomes over time 19. 31 interventional studies were included to evaluate the direct impact of therapeutic or preventive measures by assigning participants to treatment or control groups 22.
Diarrheal etiologies
The most frequently reported bacterial causes of diarrhea were E. coli, Salmonella enterica, and Shigella spp., identified in 125, 65, and 47 studies, respectively. Vibrio cholerae was examined in 29 studies, while Clostridium difficile appeared in 3 studies. Cholera emerges periodically as outbreaks which prompts investigation and increased reporting. C. difficile is likely more prevalent than reported as it’s infection is triggered by antibiotic use which is widespread in hospitals but it’s detection is complicated due to limited diagnostics and culture capabilities as it is a strict anaerobe. Among viral agents, Rotavirus was the most reported, followed by Norovirus and Adenovirus. Parasitic causes such as Giardia spp., Cryptosporidium spp., and Entamoeba spp. were significant in 34, 21, and 18 studies, respectively 23, 24. The review demonstrates that bacteria are the most common etiological agents, especially Escherichia coli, Shigella, Salmonella and Vibrio cholerae 25. These bacteria are highly prevalent because they are easily ingested via contact with contaminated food, water, environment, fecal matter and animals. As a result these bacterial pathogens have been extensively studied in these papers compared to other pathogens. Shigella causes approximately, 125 million diarrhea episodes and 160,000 deaths every year, with a third affecting children aged 5 years and below 26, while diarrheagenic E. coli causes about 70,000 deaths in children under 5 years of age in Africa 6.
Despite the dominance of bacterial etiologies, parasite and viral etiologies are not insignificant and the treatment and mitigation for non-bacterial etiologies could be optimized to reduce the burden of diarrhea diseases. The rates of parasitic infections were low most likely due to the administration of deworming treatment for children. These easy interventions should be more aggressively implemented to further reduce the incidence of parasitic infections not only cause diarrhea but can contribute to nutritional deficiencies and stunting in children 26.
Geographical variations in etiology
Western Kenya had the most prevalent parasitic causes which could be due to flooding events frequently experienced in this region 27 as supported by a study in Pacific Island that amoebiasis was associated with flooding 28. These flooding events can overwhelm wastewater treatment plants, septic tanks and latrines releasing raw sewage into the environment and into water sources with viable microbial pathogens causing upsurges in diarrheal disease 28. Bacterial, viral, and parasitic pathogens infections were significantly high in Luo Nyanza. Central Kenya had predominantly bacterial and viral pathogens while the Coastal region had a higher burden of viral etiologies. The North Eastern region reported high prevalence of bacterial pathogens 29 which could suggest that viral pathogens do not thrive in persistently dry regions. With the identification of the pathogens independently associated with moderate to severe diarrhea and their respective pathogen-specific AF, it is estimated that 35.62–46.03% of MSD could be reduced with specific interventions against those particular pathogens such as effective vaccines 30.
It is important to note that no studies of diarrheal diseases were conducted in counties like Tana River, Taita Taveta, Kirinyaga, Nyandarua and Nyeri counties had. This underreporting could reflect a truly low incidence of disease but could also be due to historic misconceptions about the distribution of diarrheal disease leading to low research interest in those regions. Another reason could be because of the logistical challenges of conducting research in remote and hard to reach areas with low population density (Tana River and Taita Taveta). Outbreaks of other infectious diseases or public health emergencies can overshadow diarrheal diseases leading to a neglect in diarrheal diseases.
Risk factors associated with diarrhea
Seasonal changes significantly impacted the prevalence and etiology of diarrheal diseases. Studies indicated that dry months were associated with higher incidences of Norovirus, while rainy seasons saw increased cases of Shigella and E. coli. In Malindi, E. coli infections were more common during dry seasons 4. Rotavirus and adenovirus cases peaked in the dry months while norovirus GII and sapovirus peaked in the rainy season. Astrovirus did not display clear seasonality according to another study done in Kilifi 31, 32. Similar patterns in the seasonality of rotavirus, adenovirus, norovirus and sapovirus have been observed elsewhere 26, 33, 34. These findings underscore the influence of seasonal variations on diarrheal disease patterns, necessitating tailored public health responses based on seasonal trends 31. Our findings however are in contrast with a study done by Fan et al., 2019 in Malawi, where the prevalence of Norovirus was lower in the dry seasons compared to the rainy seasons) 35.
Multiple studies identified socioeconomic factors, hygiene practices, and environmental risks as key contributors to diarrheal prevalence. Poor hygiene, lack of sanitation, and use of natural water sources were consistently associated with higher diarrhea incidence 2. Children under five years were particularly vulnerable, with peak incidences during weaning periods. Other studies also highlighted gender disparities, with male children experiencing higher rates of Rotavirus infection 16.
Hygiene practices related with washing hands and having facilities to dispose child’s stool have been associated with increased risk of diarrhea 30. Limited access to safe water and poor sanitation, coupled with poor hygiene practices have been reported to be high risk factor for diarrhea by several studies 30. Toilet sharing creates unsanitary and unkempt conditions, which provide conducive environments for vectors and pathogens associated with diarrhea, increasing also the possibility of inter-household transmission 27. Thus, our findings reinforce the need to improve the implementation of general sanitation practices (such as washing hands and having facilities to dispose child’s stools safely), particularly among children aged 0–59 months who presented the highest risk. Breast-feeding, especially if this is the only source of nutrition, has been shown to protect children against diarrhea in Africa as elsewhere in the developing world 36. High diarrhea incidences during weaning period can be attributed to introduction of external food and interacting with an increase exposure of the toddler to contaminated food and to lack of sanitation and personal and domestic hygiene.
Interventions to prevent Diarrheal diseases
Many interventions have been explored to reduce the high prevalence of diarrheal diseases. The Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhea by WHO/UNICEF is a document by countries that came together to outline strategies that can be employed by member countries to reduce diarrheal diseases and pneumonia in children under the age of 5 years by 2025. The specific goals are: To reduce mortality from diarrhea in children less than 5 years of age to fewer than 1 per 1000 live births and to reduce the incidence of severe diarrhea by 75% in children less than 5 years of age compared to 2010 levels. These goals are envisioned to be strategically achieved through three arms Protection, Prevention, and Treatment. Under protection, some of the interventions outlined include: Exclusive breastfeeding for six months and continued breastfeeding with appropriate complementary feeding reduces the onset and severity of diarrhea. A study by Bhutta et al, reported that not breastfeeding was associated with a 165% increase in diarrhea incidence in 0-5 month-old infants 2. Interventions that helped prevent diarrheal diseases include improved sanitation was reported to reduce the risk of diarrhea by 36% 2. Hand-washing practices reduced the risk of diarrhea by 48% 37. House-hold water treatment and safe storage to ensure safe-drinking water reduced the risk of diarrhea by 31-52% 38. In the Treatment arm, the use of ORS was noted to reduce diarrheal mortality by 93% in the case of 100% coverage 39, and the use of Zinc in the treatment of diarrhea reduced mortality by 23 % 38.
The use of vaccines against Rotavirus, the most common cause of childhood diarrhea deaths, substantially reduces the disease burden and deaths. After the monovalent Rotarix® vaccine was introduced into Kenya’s National Immunization Programme in July 2014, with doses given at 6 and 10 weeks of life, a multi-site case-control study found an overall 2-dose vaccine effectiveness of about 64% in under five years old children resulting in a significant decline of rotavirus group A (RVA) disease burden in Kenya 40. A 10.5% reduction of in rotavirus prevalence in coastal Kenya following the rotarix vaccine introduction has been reported 32. These findings concur with findings of a recent multi-site study in Kenya that reported RVA vaccine effectiveness of ~64% (95% CI: 35–80%) and a reduction in rotavirus-associated hospital admissions two years post-vaccine introduction of ~80% (95% CI: 46–93%) 31, 32. A significant increase in the prevalence of norovirus GII in post-rotavirus vaccine introduction has been reported in Kilifi 32, similar findings have been observed in the United States, Nicaragua and Bolivia following RVA vaccine introduction 41. The driving force behind this phenomenon is unclear. It has also been noted that the introduction of rotavirus vaccines may result in the shift of diarrhea disease burden to slightly older age groups (12.5 months) compared 11.2 months pre-introduction. This in part may be explained by the higher immunity at both individual and population levels against rotavirus that wanes as children grow older. This finding reinforces evidence of the continued benefit of rotavirus vaccination in Kenya.
The role of Water, Sanitation and Hygiene (WASH) in diarrheal infections
Poor water, sanitation, and hygiene conditions are the primary routes of exposure and infection. Sanitation and hygiene interventions are estimated to generate a 36% and 48% reduction in diarrheal risk in young children, respectively 41. Target 6.2 of the Sustainable Development Goals(SDG) aims to ensure adequate sanitation for all and to end open defecation, which contaminates water and spreads diseases such as cholera, diarrhea, and dysentery, by 2030 42. In sub-Saharan Africa, an estimated 215 million people engage in open defecation 43. Only 3 countries (Ethiopia, Angola and Sao Tome and Principe) decreased open defecation by 10 % or more between 2005 and 2010 42. In Kenya, an estimated 5.6 million people still defecate in the open 44. This review notes that Open defecation and lack of proper sanitation are associated with high incidences of diarrhea. Ninety percent of diarrhea deaths in children under five years in Kenya are attributed to poor water, sanitation, and hygiene 2. A study conducted in Kisumu and Busia in 2012,2013 and 2014 revealed that sub-counties certified as Open Defecation Free showed a decline in diarrhea cases in children across the three years compared to sub-counties yet to attain this status 45. A review of historical data from the Kenya Health and Demographic Surveys (KHDHS) from the years 1989,1993,1998,2003,2008-09,2014,2022 shows a decreasing prevalence of diarrhea in children under five years old over the years, from as high as 17% in 1998 to 14% in 2022 6, 46. This decrease reflects the national efforts to improve hygiene and sanitation in agreement with the global goal of SDG 6.2. Antimicrobial use and resistance patterns.
Antimicrobial use and resistance patterns.
Antibiotic resistance emerged as a critical concern, with high resistance rates reported for commonly used antibiotics such as ampicillin, tetracycline, and trimethoprim/sulfamethoxazole. These antibiotics are widely used due to their availability and affordability in Kenya. The widespread usage of tetracycline in livestock husbandry in Kenya could be a contributing factor to its high resistance 47. Exposure to commercial-scale farm raised chickens 48 and consumption of retail meat 49 have been shown to increase individuals' risk for carriage of and infection by antibiotic-resistant E. coli, and the causal link between the carriage of resistant fecal flora in human populations and the use of antibiotics in farm animals has been amply demonstrated 50, 51. Although most diarrheal diseases are self-resolving and should not be treated with antimicrobial agents, in the event of prolonged diarrhea that necessitate treatment, fluid and electrolyte administration is indicated. Correct fluid prescription has been proven to significantly reduce the risk of early mortality (within 2 days) in all subgroups 52. The use of oral rehydration salts has been reported to reduce diarrhea related mortality in Kenya by 10.2% 45. Antimicrobial drug therapy is indicated for acute infectious gastroenteritis especially among children 47. This review noted significant patterns of antibiotic use, which may be due to uncontrolled use of antibiotics such as self – medicating and access to drugs without prescription with widespread consideration of ampicillin, tetracycline, chloramphenicol, ceftriaxone, and gentamicin. The emergence of multidrug-resistant strains and ESBL-producing organisms, particularly among diarrheagenic E. coli, represents a major public health challenge. Particularly concerning is the high prevalence of extended-spectrum beta-lactamase (ESBL)-producing organisms. Our review found that 27% of enteroaggregative E. coli (EAEC) and 50% of enterotoxigenic E. coli (ETEC) isolates were ESBL producers. These organisms can hydrolyze a wide range of beta-lactam antibiotics, rendering them ineffective and complicating treatment options 53. Horizontal gene transfer which occur more commonly among E. coli isolates than the other pathogen genera, leads to a higher prevalence of non-susceptibility to commonly used antibiotics further complicating their treatment 37. In this review, Shigella species showed multiple drug resistance pattern which is in tandem with the detection of multiple-resistant Shigella strains in Africa, England and Asia 54, 55. The resistance pattern in our study could be explained by the presence of dhfr Ia gene previously described in Shigella and considered the most common dihydrofolate reductase gene in the genus 36, 56. In East Africa and other African countries, low resistance to nalidixic acid and no resistance to ciprofloxacin has been observed in Shigella isolates 57. Low resistance to ciprofloxacin, norfloxacin, ceftriaxone and cefuroxime by Shigella species indicates that these drugs may be more effective therapeutic alternatives and further supports the current use of these regimens 58, 59. This finding is critical considering the numerous factors that include frequent overuse and misuse of antimicrobials that may contribute to resistance by pathogens causing gastroenteritis in developing countries like Kenya. Resistance patterns for C. difficile also indicated high levels of resistance to multiple antibiotics 18, 60. The high frequency of antimicrobial resistance reported in these findings is not unique to Kenya. Similar findings have been reported in studies conducted among children in Vietnam, Central Africa, Tanzania, México, Argentina and Mozambique, where high levels of erythromycin and ampicillin resistance was observed for all the tested pathogens 61, 62. This also concurs with an earlier report of a worldwide occurrence of drug resistant enteric pathogens, a development attributed to inaccurate diagnosis and inappropriate use of these drugs in the treatment of infections 57, 63. These findings highlight the critical nature of problems caused by antimicrobial resistance in many developing countries where frequent illnesses coupled with ready access to unregulated antibiotics diminishes the value of these agents for those patients who actually need them.
Study limitations
This review aimed to map existing literature on the prevalence, etiology, risk factors, and interventions of diarrheal diseases in Kenya. However, there were limitations in the reliance on only formal publicly available publications and not grey literature sources, such as the public databases such as Kenya Health Information Software (KHIS]. This data was not included due to concerns about data quality and consistency however, the exclusion may have led to an underrepresentation of diarrhea incidence and prevalence data from some counties, and trends and interventions documented in grey sources. During article screening, it is possible that some studies were missed due to the terms and databases used and due to the reviewer’s subjective judgement on what to include. The importance of reliable and consistent public health data cannot be overemphasized for implementing targeted interventions for high burden diseases such as diarrhea for generating alerts to public health events like outbreaks.
From the scoping review the prevalence of diarrhea varies considerably and ranges from 3.44% to 20.79% across countries. The data is skewed towards children under 5 but is also a significant disease in adults especially in outbreaks. The causes of diarrhea are varied and regrettably include vaccine preventable disease such as rotavirus and easily managed infections such as parasitic diseases. Some etiologies are likely underrepresented such as C. difficile due to diagnostic challenges and poor representation by adults. Geographical variations require regional specific interventions or therapies and more studies in understudied regions and counties in Kenya. The seasonality trends in some of infections calls for adequate preparedness for timely interventions to reduce the impact of their spike. There is need for implementation of public health policies that have been put in place to address the issues on sanitation, hygiene and antibiotic utilization for effective response to high prevalence of diarrhea and the emerging increase of antibiotic resistance to some of the widely used antibiotics.
We acknowledge Erick Odoyo for critical review of the article.
Research Grant EDCTP3 HORIZON-JU-GH-EDCTP3- 2022-01 proposal Number: 101103059 “Linking Infectious Disease Front-liners’ control Efforts with central public health authorities in The African Great Lakes Region” GREAT-LIFE.
| [1] | Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015 Jan 31; 385(9966): 430–40. | ||
| In article | View Article PubMed | ||
| [2] | Mwenda JM, Kimani EK, Ombati JA. Diarrheal Disease Surveillance in Kenya. East African Medical Journal. 2020; 97(3): 223–35. | ||
| In article | |||
| [3] | GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018 Nov; 18(11): 1211–28. | ||
| In article | |||
| [4] | Guillaume DA, Justus OOS, Ephantus KW. Factors influencing diarrheal prevalence among children under five years in Mathare Informal Settlement, Nairobi, Kenya. J Public Health Afr. 2020 Apr 29; 11(1): 1312. | ||
| In article | View Article PubMed | ||
| [5] | Karinja M, Schlienger R, Pillai GC, Esterhuizen T, Onyango E, Gitau A, et al. Risk reduction of diarrhea and respiratory infections following a community health education program - a facility-based case-control study in rural parts of Kenya. BMC Public Health. 2020 Apr 29; 20(1): 586. | ||
| In article | View Article PubMed | ||
| [6] | Kamau M. Kenya Demographic and Health Survey (KDHS) 2022 [Internet]. Kenya National Bureau of Statistics. 2023 [cited 2024 May 21]. Available from: https:// www.knbs.or.ke/ kenya-demographic- and-health-survey-kdhs-2022/ | ||
| In article | |||
| [7] | Hendriksen RS, Lukjancenko O, Munk P, Hjelmsø MH, Verani JR, Ng’eno E, et al. Pathogen surveillance in the informal settlement, Kibera, Kenya, using a metagenomics approach. PLoS One. 2019; 14(10): e0222531. | ||
| In article | View Article PubMed | ||
| [8] | Wandera EA, Muriithi B, Kathiiko C, Mutunga F, Wachira M, Mumo M, et al. Impact of integrated water, sanitation, hygiene, health and nutritional interventions on diarrhoea disease epidemiology and microbial quality of water in a resource-constrained setting in Kenya: A controlled intervention study. Trop Med Int Health. 2022 Aug; 27(8): 669–77. | ||
| In article | View Article PubMed | ||
| [9] | Westphaln KK, Regoeczi W, Masotya M, Vazquez-Westphaln B, Lounsbury K, McDavid L, et al. From Arksey and O’Malley and Beyond: Customizations to enhance a team-based, mixed approach to scoping review methodology. MethodsX. 2021; 8: 101375. | ||
| In article | View Article PubMed | ||
| [10] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29; 372: n71. | ||
| In article | View Article PubMed | ||
| [11] | DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986 Sep; 7(3): 177–88. | ||
| In article | View Article PubMed | ||
| [12] | Ahmed KKM, Al Dhubaib BE. Zotero: A bibliographic assistant to researcher. J Pharmacol Pharmacother. 2011 Oct; 2(4): 303–5. | ||
| In article | View Article PubMed | ||
| [13] | Lewin S, Glenton C, Oxman AD. Use of qualitative methods alongside randomised controlled trials of complex healthcare interventions: methodological study. BMJ. 2009 Sep 10; 339: b3496. | ||
| In article | View Article PubMed | ||
| [14] | Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018 Oct 2; 169(7): 467–73. | ||
| In article | View Article PubMed | ||
| [15] | Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. 2010 Apr; 1(2): 97–111. | ||
| In article | View Article PubMed | ||
| [16] | Muriithi JM, Otieno FK, Kipkemoi PJ. Risk Factors for Diarrhea in Kenyan Children. Pediatric Health Research. 2022; 15(1): 112–21. | ||
| In article | |||
| [17] | Munn Z, Pollock D, Price C, Aromataris E, Stern C, Stone JC, et al. Investigating different typologies for the synthesis of evidence: a scoping review protocol. JBI Evid Synth. 2023 Mar 1; 21(3): 592–600. | ||
| In article | |||
| [18] | Mwangi PN, Njeri PK, Wamalwa DC. Antibiotic Resistance in Enteric Pathogens. Journal of Infectious Diseases in Developing Countries. 2021; 15(6): 543–52. | ||
| In article | |||
| [19] | Euser AM, Zoccali C, Jager KJ, Dekker FW. Cohort studies: prospective versus retrospective. Nephron Clin Pract. 2009; 113(3): c214-217. | ||
| In article | View Article PubMed | ||
| [20] | Caruana EJ, Roman M, Hernández-Sánchez J, Solli P. Longitudinal studies. J Thorac Dis. 2015 Nov; 7(11): E537-540. | ||
| In article | |||
| [21] | Lewallen S, Courtright P. Epidemiology in practice: case-control studies. Community Eye Health. 1998; 11(28): 57–8. | ||
| In article | |||
| [22] | Thakur N, Shah D. Interventional Study Designs. Indian Pediatr. 2021 Dec 15; 58(12): 1171–81. | ||
| In article | View Article PubMed | ||
| [23] | Kimani EK, Mwenda JM, Ngure PK. Enteric Pathogens in Kenya. African Journal of Health Sciences. 2020; 19(4): 345–57. | ||
| In article | |||
| [24] | Wamalwa DC, Mwangi PN, Kipkemoi PJ. Viral Agents in Diarrheal Diseases. Virology Journal. 2021; 18(3): 301–10. | ||
| In article | |||
| [25] | Khan DSA, Naseem R, Salam RA, Lassi ZS, Das JK, Bhutta ZA. Interventions for High-Burden Infectious Diseases in Children and Adolescents: A Meta-analysis. Pediatrics. 2022 May 1; 149(Suppl 5): e2021053852C. | ||
| In article | View Article PubMed | ||
| [26] | Omore R, Tate JE, O’Reilly CE, Ayers T, Williamson J, Moke F, et al. Epidemiology, Seasonality and Factors Associated with Rotavirus Infection among Children with Moderate-to-Severe Diarrhea in Rural Western Kenya, 2008-2012: The Global Enteric Multicenter Study (GEMS). PLoS One. 2016; 11(8): e0160060. | ||
| In article | View Article PubMed | ||
| [27] | Boadi KO, Kuitunen M. Environmental and health impacts of household solid waste handling and disposal practices in third world cities: the case of the Accra Metropolitan Area, Ghana. Journal of environmental health. 2005; 68(4): 32–6. | ||
| In article | |||
| [28] | Shea EL, Dolcemascolo G, Anderson CL, Barnston A, Guard CP, Hamnett MP, et al. Preparing for a changing climate: The potential consequences of climate variability and change. 2001. | ||
| In article | |||
| [29] | Ngure PK, Mutuku JK, Wamalwa DC. Etiology of Diarrhea in Coastal Kenya. Coastal Health Journal. 2020; 8(4): 211–23. | ||
| In article | |||
| [30] | Nhampossa T, Mandomando I, Acacio S, Quintó L, Vubil D, Ruiz J, et al. Diarrheal Disease in Rural Mozambique: Burden, Risk Factors and Etiology of Diarrheal Disease among Children Aged 0–59 Months Seeking Care at Health Facilities. PLOS ONE. 2015; 10(5): 0119824. | ||
| In article | View Article PubMed | ||
| [31] | Otieno FK, Muriithi JM, Njeri PK. Seasonal Patterns of Diarrheal Diseases in Kenya. Climate and Health. 2023; 14(1): 78–90. | ||
| In article | |||
| [32] | Lambisia AW, Onchaga S, Murunga N, Lewa CS, Nyanjom SG, Agoti CN. Epidemiological Trends of Five Common Diarrhea-Associated Enteric Viruses Pre- and Post-Rotavirus Vaccine Introduction in Coastal Kenya. Pathogens [Internet]. 2020; 9(8). | ||
| In article | View Article PubMed | ||
| [33] | S.M. A, B.A. L, K L. A Systematic Review and Meta-Analysis of the Global Seasonality of Norovirus. PLoS ONE. 2013; 8: e75922. | ||
| In article | View Article PubMed | ||
| [34] | Dey SK, Phathammavong O, Nguyen TD, Thongprachum A, Chan-It W, Okitsu S, et al. Seasonal pattern and genotype distribution of sapovirus infection in Japan, 2003-2009. Epidemiol Infect. 2012 Jan; 140(1): 74–7. | ||
| In article | View Article PubMed | ||
| [35] | Fan YM, Oikarinen S, Lehto KM, Nurminen N, Juuti R, Mangani C, et al. High prevalence of selected viruses and parasites and their predictors in Malawian children. Epidemiol Infect. 2019 Jan. | ||
| In article | View Article PubMed | ||
| [36] | Lamberti LM, Fischer Walker CL, Noiman A, Victora C, Black RE. Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health. 2011 Apr 29; 11 Suppl 3: S15. | ||
| In article | View Article PubMed | ||
| [37] | Navia MM, Capitano L, Ruiz J, Vargas M, Urassa H, Schellemberg D, et al. Typing and Characterization of Mechanisms of Resistance ofShigella spp. Isolated from Feces of Children under 5 Years of Age from Ifakara, Tanzania. J Clin Microbiol. 1999; 37(10): 3113–7. | ||
| In article | View Article PubMed | ||
| [38] | CL FW, RE B. Zinc for the treatment of diarrhoea: effect on diarrhoea morbidity, mortality and incidence of future episodes. International Journal of Epidemiology. 2010; 39(Suppl 1). | ||
| In article | View Article PubMed | ||
| [39] | Munos MK, Walker CL, Black RE. The effect of oral rehydration solution and recommended home fluids on diarrhoea mortality. International Journal of Epidemiology. 2010; 39(Suppl 1). | ||
| In article | View Article PubMed | ||
| [40] | Mwanga MJ, Verani JR, Omore R, Tate JE, Parashar UD, Murunga N, et al. Multiple Introductions and Predominance of Rotavirus Group A Genotype G3P [ 8] in Kilifi, Coastal Kenya, 4 Years after Nationwide Vaccine Introduction. Pathogens. 2020; 9(12): 981. | ||
| In article | View Article PubMed | ||
| [41] | Bucardo F, Reyes Y, Svensson L, Nordgren J. Predominance of norovirus and sapovirus in Nicaragua after implementation of universal rotavirus vaccination. PLoS One. 2014; 9(5): e98201. | ||
| In article | View Article PubMed | ||
| [42] | Nations U. Sustainable Development Goal 6: Ensure availability and sustainable management of water and sanitation for all.https://sdgs.un.org/goals/goal6. XXXX. | ||
| In article | |||
| [43] | Galan ID, Kim SS, Graham JP. Exploring changes in open defecation prevalence in sub-Saharan Africa based on national level indices. BMC Public Health. 2013; 13(527). | ||
| In article | View Article PubMed | ||
| [44] | Njuguna J. Effect of eliminating open defecation on diarrhoeal morbidity: an ecological study of Nyando and Nambale sub-counties, Kenya. BMC Public Health. 2016; 16: 712. | ||
| In article | View Article PubMed | ||
| [45] | Akech S, Ayieko P, Gathara D, Agweyu A, Irimu G, Stepniewska K, et al. Clinical Information Network authors. Risk factors for mortality and effect of correct fluid prescription in children with diarrhoea and dehydration without severe acute malnutrition admitted to Kenyan hospitals: an observational, association study. Lancet Child Adolesc Health. 2018 Jul 2. | ||
| In article | View Article PubMed | ||
| [46] | Population NC, Development. Central Bureau of Statistics (CBS) [Kenya. In: and Macro International Inc 1999 Kenya Demographic and Health Survey 1998. Calverton, Maryland: NCPD, CBS, and Macro International Inc. | ||
| In article | |||
| [47] | Mitema ES, Kikuvi GM, Wegener HC, Stohr K. An assessment of antimicrobial consumption in food producing animals in Kenya. Journal of Veterinary Pharmacology and Therapeutics. 2001; 385–90. | ||
| In article | View Article PubMed | ||
| [48] | Price LB, Graham JP, Lackey LG, Roess A, Vailes R, Silbergeld E. Elevated risk of carrying gentamicin-resistant Escherichia coli among U.S. poultry workers. Environ Health Perspect. 2007; 115: 1738–42. | ||
| In article | View Article PubMed | ||
| [49] | Manges AR, Smith SP, Lau BJ, Nubal CJ, Eisenberg JH, Dietrich PS, et al. Retail meat consumption and the acquisition of antimicrobial resistant Escherichia coli causing urinary tract infections: a case-control study. Foodborne Pathog Dis. 2007; 4: 419–31. | ||
| In article | View Article PubMed | ||
| [50] | Wegener HC, Aarestrup FM, Jensen LB, Hammerum AM, Bager F. Use of antimicrobial growth promoters in food animals and Enterococcus faecium resistance to therapeutic antimicrobial drugs in Europe. Emerg Infect Dis. 1999; 5: 329–35. | ||
| In article | View Article PubMed | ||
| [51] | Garau J, Xercavins M, Rodriguez-Carballeira M, Gomez-Vera C JR, I V, D L, et al. Emergence and dissemination of quinolone-resistant Escherichia coli in the community. Antimicrob Agents Chemother. 1999; 43: 2736–41. | ||
| In article | View Article PubMed | ||
| [52] | Deichsel EL, Powell H, Troeger C, Hossain MJ, Sow SO, Omore R, et al. Drivers of Decline in Diarrhea Mortality Between GEMS and VIDA Studies. Clinical Infectious Diseases. 2023; 76(Supplement_1): 58–65. | ||
| In article | View Article PubMed | ||
| [53] | Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005 Oct; 18(4): 657–86. | ||
| In article | View Article PubMed | ||
| [54] | Langendorf C, Hello SL, Moumouni A, Gouali M, Mamaty A, Grais RF, et al. Enteric Bacterial Pathogens in Children with Diarrhea in Niger: Diversity and Antimicrobial Resistance. PLoS ONE. 2015; 10(3). | ||
| In article | View Article PubMed | ||
| [55] | Ajayi OI, Ojo DA, Akinduti PA, Akintokun AK, Akinrotoye KP. Prevalence and antibiotic resistance profiles of serotypes of Shigella species isolated from community children in Odeda local government. Ogun State J Environ Treat Tech. 2019; 7(3): 270–81. | ||
| In article | |||
| [56] | Sang WK, Oundo V, Schnabel D. Prevalence and antibiotic resistance of bacterial pathogens isolated from childhood diarrhoea in four provinces of Kenya. J Infect Developing Countries. 2012; 6(07): 572–8. | ||
| In article | View Article PubMed | ||
| [57] | Aslam B, Wang W, Arshad MI, Khurshid M, Muzammil S, Rasool MH, et al. Antibiotic resistance: a rundown of a global crisis. Infect Drug Resistance. 2018; 11(1645). | ||
| In article | View Article PubMed | ||
| [58] | Brooks JT, Ochieng JB, Kumar L, Okoth G, Shapiro RL, Wells JG, et al. Surveillance for bacterial diarrhoea and antimicrobial resistance in rural western Kenya, 1997–2003. Clin Infect Dis. 2006; 43(4): 393–401. | ||
| In article | View Article PubMed | ||
| [59] | Public Health KM, Sanitation. Policy guidelines on control and management of diarrhoeal diseases in children below five years in Kenya. Nairobi: Kenya Ministry of Public Health and Sanitation; 2010. 1–11 p. | ||
| In article | |||
| [60] | Njeri PK, Kipkemoi PJ, Otieno FK. Trends in Antibiotic Resistance among Diarrheal Pathogens. Antimicrobial Resistance & Infection Control. 2023; 12(2): 345–56. | ||
| In article | |||
| [61] | Vargas M, Ochoa TJ, Ruiz J, Molina M, Del Valle LJ, Gil AI, et al. High frequency of Antimicrobial Drug resistance of Diarrheagenic E.coli in infants in Peru. Am J Trop Med Hyg. 2009; 81(2): 296–301. | ||
| In article | View Article PubMed | ||
| [62] | Organization WH. Manual for the laboratory identification and antimicrobial susceptibility testing of bacterial pathogens of public health concern in the developing world. 2003. | ||
| In article | |||
| [63] | Udo SM, Eja ME. Prevalence and antibiotic resistant Shigellae among primary school children in urban Calabar, Nigeria. Asia Pac J Public Health. 2004; 16(1): 41–4. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2024 Fredrick Ogumbo, Latifah Benta, Brian Kimutai, Joseph Mugah, Eddy Johnson, Vanessa Onyonyi, Caroline Dande, Lillian Musila and Steve Wandiga
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015 Jan 31; 385(9966): 430–40. | ||
| In article | View Article PubMed | ||
| [2] | Mwenda JM, Kimani EK, Ombati JA. Diarrheal Disease Surveillance in Kenya. East African Medical Journal. 2020; 97(3): 223–35. | ||
| In article | |||
| [3] | GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018 Nov; 18(11): 1211–28. | ||
| In article | |||
| [4] | Guillaume DA, Justus OOS, Ephantus KW. Factors influencing diarrheal prevalence among children under five years in Mathare Informal Settlement, Nairobi, Kenya. J Public Health Afr. 2020 Apr 29; 11(1): 1312. | ||
| In article | View Article PubMed | ||
| [5] | Karinja M, Schlienger R, Pillai GC, Esterhuizen T, Onyango E, Gitau A, et al. Risk reduction of diarrhea and respiratory infections following a community health education program - a facility-based case-control study in rural parts of Kenya. BMC Public Health. 2020 Apr 29; 20(1): 586. | ||
| In article | View Article PubMed | ||
| [6] | Kamau M. Kenya Demographic and Health Survey (KDHS) 2022 [Internet]. Kenya National Bureau of Statistics. 2023 [cited 2024 May 21]. Available from: https:// www.knbs.or.ke/ kenya-demographic- and-health-survey-kdhs-2022/ | ||
| In article | |||
| [7] | Hendriksen RS, Lukjancenko O, Munk P, Hjelmsø MH, Verani JR, Ng’eno E, et al. Pathogen surveillance in the informal settlement, Kibera, Kenya, using a metagenomics approach. PLoS One. 2019; 14(10): e0222531. | ||
| In article | View Article PubMed | ||
| [8] | Wandera EA, Muriithi B, Kathiiko C, Mutunga F, Wachira M, Mumo M, et al. Impact of integrated water, sanitation, hygiene, health and nutritional interventions on diarrhoea disease epidemiology and microbial quality of water in a resource-constrained setting in Kenya: A controlled intervention study. Trop Med Int Health. 2022 Aug; 27(8): 669–77. | ||
| In article | View Article PubMed | ||
| [9] | Westphaln KK, Regoeczi W, Masotya M, Vazquez-Westphaln B, Lounsbury K, McDavid L, et al. From Arksey and O’Malley and Beyond: Customizations to enhance a team-based, mixed approach to scoping review methodology. MethodsX. 2021; 8: 101375. | ||
| In article | View Article PubMed | ||
| [10] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29; 372: n71. | ||
| In article | View Article PubMed | ||
| [11] | DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986 Sep; 7(3): 177–88. | ||
| In article | View Article PubMed | ||
| [12] | Ahmed KKM, Al Dhubaib BE. Zotero: A bibliographic assistant to researcher. J Pharmacol Pharmacother. 2011 Oct; 2(4): 303–5. | ||
| In article | View Article PubMed | ||
| [13] | Lewin S, Glenton C, Oxman AD. Use of qualitative methods alongside randomised controlled trials of complex healthcare interventions: methodological study. BMJ. 2009 Sep 10; 339: b3496. | ||
| In article | View Article PubMed | ||
| [14] | Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018 Oct 2; 169(7): 467–73. | ||
| In article | View Article PubMed | ||
| [15] | Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. 2010 Apr; 1(2): 97–111. | ||
| In article | View Article PubMed | ||
| [16] | Muriithi JM, Otieno FK, Kipkemoi PJ. Risk Factors for Diarrhea in Kenyan Children. Pediatric Health Research. 2022; 15(1): 112–21. | ||
| In article | |||
| [17] | Munn Z, Pollock D, Price C, Aromataris E, Stern C, Stone JC, et al. Investigating different typologies for the synthesis of evidence: a scoping review protocol. JBI Evid Synth. 2023 Mar 1; 21(3): 592–600. | ||
| In article | |||
| [18] | Mwangi PN, Njeri PK, Wamalwa DC. Antibiotic Resistance in Enteric Pathogens. Journal of Infectious Diseases in Developing Countries. 2021; 15(6): 543–52. | ||
| In article | |||
| [19] | Euser AM, Zoccali C, Jager KJ, Dekker FW. Cohort studies: prospective versus retrospective. Nephron Clin Pract. 2009; 113(3): c214-217. | ||
| In article | View Article PubMed | ||
| [20] | Caruana EJ, Roman M, Hernández-Sánchez J, Solli P. Longitudinal studies. J Thorac Dis. 2015 Nov; 7(11): E537-540. | ||
| In article | |||
| [21] | Lewallen S, Courtright P. Epidemiology in practice: case-control studies. Community Eye Health. 1998; 11(28): 57–8. | ||
| In article | |||
| [22] | Thakur N, Shah D. Interventional Study Designs. Indian Pediatr. 2021 Dec 15; 58(12): 1171–81. | ||
| In article | View Article PubMed | ||
| [23] | Kimani EK, Mwenda JM, Ngure PK. Enteric Pathogens in Kenya. African Journal of Health Sciences. 2020; 19(4): 345–57. | ||
| In article | |||
| [24] | Wamalwa DC, Mwangi PN, Kipkemoi PJ. Viral Agents in Diarrheal Diseases. Virology Journal. 2021; 18(3): 301–10. | ||
| In article | |||
| [25] | Khan DSA, Naseem R, Salam RA, Lassi ZS, Das JK, Bhutta ZA. Interventions for High-Burden Infectious Diseases in Children and Adolescents: A Meta-analysis. Pediatrics. 2022 May 1; 149(Suppl 5): e2021053852C. | ||
| In article | View Article PubMed | ||
| [26] | Omore R, Tate JE, O’Reilly CE, Ayers T, Williamson J, Moke F, et al. Epidemiology, Seasonality and Factors Associated with Rotavirus Infection among Children with Moderate-to-Severe Diarrhea in Rural Western Kenya, 2008-2012: The Global Enteric Multicenter Study (GEMS). PLoS One. 2016; 11(8): e0160060. | ||
| In article | View Article PubMed | ||
| [27] | Boadi KO, Kuitunen M. Environmental and health impacts of household solid waste handling and disposal practices in third world cities: the case of the Accra Metropolitan Area, Ghana. Journal of environmental health. 2005; 68(4): 32–6. | ||
| In article | |||
| [28] | Shea EL, Dolcemascolo G, Anderson CL, Barnston A, Guard CP, Hamnett MP, et al. Preparing for a changing climate: The potential consequences of climate variability and change. 2001. | ||
| In article | |||
| [29] | Ngure PK, Mutuku JK, Wamalwa DC. Etiology of Diarrhea in Coastal Kenya. Coastal Health Journal. 2020; 8(4): 211–23. | ||
| In article | |||
| [30] | Nhampossa T, Mandomando I, Acacio S, Quintó L, Vubil D, Ruiz J, et al. Diarrheal Disease in Rural Mozambique: Burden, Risk Factors and Etiology of Diarrheal Disease among Children Aged 0–59 Months Seeking Care at Health Facilities. PLOS ONE. 2015; 10(5): 0119824. | ||
| In article | View Article PubMed | ||
| [31] | Otieno FK, Muriithi JM, Njeri PK. Seasonal Patterns of Diarrheal Diseases in Kenya. Climate and Health. 2023; 14(1): 78–90. | ||
| In article | |||
| [32] | Lambisia AW, Onchaga S, Murunga N, Lewa CS, Nyanjom SG, Agoti CN. Epidemiological Trends of Five Common Diarrhea-Associated Enteric Viruses Pre- and Post-Rotavirus Vaccine Introduction in Coastal Kenya. Pathogens [Internet]. 2020; 9(8). | ||
| In article | View Article PubMed | ||
| [33] | S.M. A, B.A. L, K L. A Systematic Review and Meta-Analysis of the Global Seasonality of Norovirus. PLoS ONE. 2013; 8: e75922. | ||
| In article | View Article PubMed | ||
| [34] | Dey SK, Phathammavong O, Nguyen TD, Thongprachum A, Chan-It W, Okitsu S, et al. Seasonal pattern and genotype distribution of sapovirus infection in Japan, 2003-2009. Epidemiol Infect. 2012 Jan; 140(1): 74–7. | ||
| In article | View Article PubMed | ||
| [35] | Fan YM, Oikarinen S, Lehto KM, Nurminen N, Juuti R, Mangani C, et al. High prevalence of selected viruses and parasites and their predictors in Malawian children. Epidemiol Infect. 2019 Jan. | ||
| In article | View Article PubMed | ||
| [36] | Lamberti LM, Fischer Walker CL, Noiman A, Victora C, Black RE. Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health. 2011 Apr 29; 11 Suppl 3: S15. | ||
| In article | View Article PubMed | ||
| [37] | Navia MM, Capitano L, Ruiz J, Vargas M, Urassa H, Schellemberg D, et al. Typing and Characterization of Mechanisms of Resistance ofShigella spp. Isolated from Feces of Children under 5 Years of Age from Ifakara, Tanzania. J Clin Microbiol. 1999; 37(10): 3113–7. | ||
| In article | View Article PubMed | ||
| [38] | CL FW, RE B. Zinc for the treatment of diarrhoea: effect on diarrhoea morbidity, mortality and incidence of future episodes. International Journal of Epidemiology. 2010; 39(Suppl 1). | ||
| In article | View Article PubMed | ||
| [39] | Munos MK, Walker CL, Black RE. The effect of oral rehydration solution and recommended home fluids on diarrhoea mortality. International Journal of Epidemiology. 2010; 39(Suppl 1). | ||
| In article | View Article PubMed | ||
| [40] | Mwanga MJ, Verani JR, Omore R, Tate JE, Parashar UD, Murunga N, et al. Multiple Introductions and Predominance of Rotavirus Group A Genotype G3P [ 8] in Kilifi, Coastal Kenya, 4 Years after Nationwide Vaccine Introduction. Pathogens. 2020; 9(12): 981. | ||
| In article | View Article PubMed | ||
| [41] | Bucardo F, Reyes Y, Svensson L, Nordgren J. Predominance of norovirus and sapovirus in Nicaragua after implementation of universal rotavirus vaccination. PLoS One. 2014; 9(5): e98201. | ||
| In article | View Article PubMed | ||
| [42] | Nations U. Sustainable Development Goal 6: Ensure availability and sustainable management of water and sanitation for all.https://sdgs.un.org/goals/goal6. XXXX. | ||
| In article | |||
| [43] | Galan ID, Kim SS, Graham JP. Exploring changes in open defecation prevalence in sub-Saharan Africa based on national level indices. BMC Public Health. 2013; 13(527). | ||
| In article | View Article PubMed | ||
| [44] | Njuguna J. Effect of eliminating open defecation on diarrhoeal morbidity: an ecological study of Nyando and Nambale sub-counties, Kenya. BMC Public Health. 2016; 16: 712. | ||
| In article | View Article PubMed | ||
| [45] | Akech S, Ayieko P, Gathara D, Agweyu A, Irimu G, Stepniewska K, et al. Clinical Information Network authors. Risk factors for mortality and effect of correct fluid prescription in children with diarrhoea and dehydration without severe acute malnutrition admitted to Kenyan hospitals: an observational, association study. Lancet Child Adolesc Health. 2018 Jul 2. | ||
| In article | View Article PubMed | ||
| [46] | Population NC, Development. Central Bureau of Statistics (CBS) [Kenya. In: and Macro International Inc 1999 Kenya Demographic and Health Survey 1998. Calverton, Maryland: NCPD, CBS, and Macro International Inc. | ||
| In article | |||
| [47] | Mitema ES, Kikuvi GM, Wegener HC, Stohr K. An assessment of antimicrobial consumption in food producing animals in Kenya. Journal of Veterinary Pharmacology and Therapeutics. 2001; 385–90. | ||
| In article | View Article PubMed | ||
| [48] | Price LB, Graham JP, Lackey LG, Roess A, Vailes R, Silbergeld E. Elevated risk of carrying gentamicin-resistant Escherichia coli among U.S. poultry workers. Environ Health Perspect. 2007; 115: 1738–42. | ||
| In article | View Article PubMed | ||
| [49] | Manges AR, Smith SP, Lau BJ, Nubal CJ, Eisenberg JH, Dietrich PS, et al. Retail meat consumption and the acquisition of antimicrobial resistant Escherichia coli causing urinary tract infections: a case-control study. Foodborne Pathog Dis. 2007; 4: 419–31. | ||
| In article | View Article PubMed | ||
| [50] | Wegener HC, Aarestrup FM, Jensen LB, Hammerum AM, Bager F. Use of antimicrobial growth promoters in food animals and Enterococcus faecium resistance to therapeutic antimicrobial drugs in Europe. Emerg Infect Dis. 1999; 5: 329–35. | ||
| In article | View Article PubMed | ||
| [51] | Garau J, Xercavins M, Rodriguez-Carballeira M, Gomez-Vera C JR, I V, D L, et al. Emergence and dissemination of quinolone-resistant Escherichia coli in the community. Antimicrob Agents Chemother. 1999; 43: 2736–41. | ||
| In article | View Article PubMed | ||
| [52] | Deichsel EL, Powell H, Troeger C, Hossain MJ, Sow SO, Omore R, et al. Drivers of Decline in Diarrhea Mortality Between GEMS and VIDA Studies. Clinical Infectious Diseases. 2023; 76(Supplement_1): 58–65. | ||
| In article | View Article PubMed | ||
| [53] | Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005 Oct; 18(4): 657–86. | ||
| In article | View Article PubMed | ||
| [54] | Langendorf C, Hello SL, Moumouni A, Gouali M, Mamaty A, Grais RF, et al. Enteric Bacterial Pathogens in Children with Diarrhea in Niger: Diversity and Antimicrobial Resistance. PLoS ONE. 2015; 10(3). | ||
| In article | View Article PubMed | ||
| [55] | Ajayi OI, Ojo DA, Akinduti PA, Akintokun AK, Akinrotoye KP. Prevalence and antibiotic resistance profiles of serotypes of Shigella species isolated from community children in Odeda local government. Ogun State J Environ Treat Tech. 2019; 7(3): 270–81. | ||
| In article | |||
| [56] | Sang WK, Oundo V, Schnabel D. Prevalence and antibiotic resistance of bacterial pathogens isolated from childhood diarrhoea in four provinces of Kenya. J Infect Developing Countries. 2012; 6(07): 572–8. | ||
| In article | View Article PubMed | ||
| [57] | Aslam B, Wang W, Arshad MI, Khurshid M, Muzammil S, Rasool MH, et al. Antibiotic resistance: a rundown of a global crisis. Infect Drug Resistance. 2018; 11(1645). | ||
| In article | View Article PubMed | ||
| [58] | Brooks JT, Ochieng JB, Kumar L, Okoth G, Shapiro RL, Wells JG, et al. Surveillance for bacterial diarrhoea and antimicrobial resistance in rural western Kenya, 1997–2003. Clin Infect Dis. 2006; 43(4): 393–401. | ||
| In article | View Article PubMed | ||
| [59] | Public Health KM, Sanitation. Policy guidelines on control and management of diarrhoeal diseases in children below five years in Kenya. Nairobi: Kenya Ministry of Public Health and Sanitation; 2010. 1–11 p. | ||
| In article | |||
| [60] | Njeri PK, Kipkemoi PJ, Otieno FK. Trends in Antibiotic Resistance among Diarrheal Pathogens. Antimicrobial Resistance & Infection Control. 2023; 12(2): 345–56. | ||
| In article | |||
| [61] | Vargas M, Ochoa TJ, Ruiz J, Molina M, Del Valle LJ, Gil AI, et al. High frequency of Antimicrobial Drug resistance of Diarrheagenic E.coli in infants in Peru. Am J Trop Med Hyg. 2009; 81(2): 296–301. | ||
| In article | View Article PubMed | ||
| [62] | Organization WH. Manual for the laboratory identification and antimicrobial susceptibility testing of bacterial pathogens of public health concern in the developing world. 2003. | ||
| In article | |||
| [63] | Udo SM, Eja ME. Prevalence and antibiotic resistant Shigellae among primary school children in urban Calabar, Nigeria. Asia Pac J Public Health. 2004; 16(1): 41–4. | ||
| In article | View Article PubMed | ||




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}