Occupational hazards in dentistry represent a significant concern due to the diverse risks encountered in routine clinical practice. Dental professionals are exposed to multiple categories of hazards, including biological, physical, chemical, ergonomic, and psychosocial factors, which may adversely affect their health and professional longevity. This review aims to provide a comprehensive overview of these hazards, their prevalence, associated risk factors, and current prevention strategies within the U.S. context. Evidence from existing literature indicates that biological hazards, particularly exposure to bloodborne pathogens and aerosols, remain a persistent risk despite advancements in infection control practices. Ergonomic hazards, especially musculoskeletal disorders, are highly prevalent and affect a majority of dental professionals due to prolonged static postures and repetitive movements. Chemical exposures and physical risks, such as radiation and noise, continue to pose challenges, although they are relatively well-regulated. Additionally, psychosocial stressors, including workload pressure and burnout, are increasingly recognized as critical factors influencing both practitioner well-being and quality of care. The occurrence and severity of these hazards are influenced by individual, workplace, and procedural factors, with certain groups such as dental hygienists and assistants being at higher risk. Despite improvements in safety standards and regulatory guidelines, issues such as underreporting of occupational injuries, inconsistent compliance, and gaps in education and policy implementation persist. A comprehensive and integrated approach involving enhanced research, policy development, technological advancements, and continuous education is essential to mitigate these risks and promote a safer working environment in dentistry.
Dentistry is a highly skilled healthcare profession dedicated to the prevention, diagnosis, and treatment of oral diseases and conditions affecting the craniofacial complex. Dental professionals, including dentists, dental hygienists, and dental assistants, work in close proximity to patients’ oral cavities and are routinely exposed to biological fluids, sharp instruments, and a variety of chemical agents. The nature of dental practice requires precision, prolonged static postures, and repetitive hand movements, often performed in confined clinical environments. While advancements in technology and infection control have improved safety, the profession continues to pose significant occupational risks. 1
Occupational hazards are defined as risks or dangers that arise from workplace exposures and have the potential to cause injury, illness, or adverse health effects. In dentistry, these hazards are multifactorial and typically classified into biological, physical, chemical, ergonomic, and psychosocial categories. Biological hazards include exposure to bloodborne pathogens such as hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV), primarily through needlestick injuries or contact with contaminated fluids. Physical hazards encompass radiation exposure, noise, and eye injuries, while chemical hazards arise from dental materials such as mercury, disinfectants, and acrylic resins. Ergonomic hazards, particularly musculoskeletal disorders, are among the most prevalent due to poor posture and repetitive motions. Additionally, psychosocial stressors such as workload pressure and patient anxiety contribute to mental health challenges among dental professionals. 2, 3
Studying occupational hazards within the United States context is particularly important due to the country’s unique healthcare system, regulatory framework, and workforce dynamics. The prevalence and management of occupational risks may vary based on national policies, workplace standards, and access to protective resources. In the U.S., dental practices range from private clinics to large institutional settings, each with varying levels of compliance and safety infrastructure. Furthermore, the availability of surveillance data and reporting systems allows for a more detailed understanding of hazard trends and risk factors specific to the U.S. population. 4
Regulatory and advisory bodies play a critical role in mitigating occupational hazards in dentistry. The Occupational Safety and Health Administration (OSHA) establishes and enforces workplace safety standards, including regulations on bloodborne pathogens, hazard communication, and personal protective equipment. Similarly, the Centers for Disease Control (CDC) provides evidence-based guidelines for infection control in dental settings, including recommendations for sterilization, use of personal protective equipment, and management of occupational exposures. These organizations are instrumental in shaping policies and promoting safe practices across dental care environments. 5
The aim of this narrative review is to provide a comprehensive overview of occupational hazards in dentistry within the United States. Specifically, this review seeks to categorize the major types of occupational hazards encountered in dental practice, examine their prevalence and associated risk factors, and evaluate current prevention and control measures guided by national standards. By synthesizing existing literature, this review intends to highlight key challenges and inform strategies to enhance occupational safety among dental professionals.
This study is a narrative review aimed at summarizing and synthesizing existing literature on occupational hazards in dentistry within the United States. Unlike systematic or scoping reviews, which follow strict protocols for literature selection and quantitative synthesis, a narrative review allows for a broader discussion of multiple hazard categories, associated risk factors, and prevention strategies. The focus of this review is to provide a comprehensive overview, identify patterns, and highlight gaps in current research.
Relevant literature was identified using electronic databases including PubMed, Scopus, and Google Scholar. Searches were conducted using a combination of keywords and Medical Subject Headings (MeSH) terms, such as “occupational hazards,” “workplace hazards,” “dentists,” “dental hygienists,” “dental assistants,” “United States,” “USA,” “biological hazards,” “chemical hazards,” “ergonomic hazards,” “physical hazards,” and “psychosocial hazards.” Boolean operators (AND, OR) were applied to refine search results. Only articles published in English and focused on the U.S. context were included. Grey literature, including government reports and guidelines from the CDC and OSHA, was also reviewed to ensure incorporation of current regulatory standards and recommendations.
Inclusion criteria were studies that addressed occupational hazards among dental professionals practicing in the United States, published in peer-reviewed journals or official professional guidelines, and providing information on prevalence, risk factors, or preventive measures. Exclusion criteria included studies conducted outside the U.S., research not focused on dental professionals, and case reports, conference abstracts, or opinion pieces without supporting data.
Data from the selected studies were systematically extracted, focusing on hazard types (biological, chemical, physical, ergonomic, psychosocial), prevalence or incidence rates, contributing risk factors, and recommended preventive measures. Findings were synthesized narratively, highlighting trends, key insights, and gaps in the literature. Descriptive statistics were summarized where available; however, no meta-analysis was performed due to heterogeneity among study designs and reported outcomes. The narrative synthesis allowed integration of research findings with professional guidelines from OSHA and CDC, providing a practical perspective on occupational safety for dental professionals in the United States.
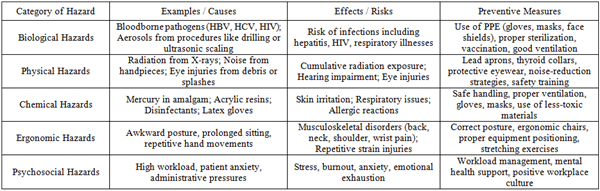
Dental professionals are exposed to various risks while performing their daily tasks. These occupational hazards can be grouped into five main categories: biological, physical, chemical, ergonomic, and psychosocial. Each type of hazard has unique causes and effects, and understanding them is essential for preventing injury or illness in dental practice.
3.1. Biological HazardsBiological hazards are caused by exposure to infectious agents. In dentistry, bloodborne pathogens such as hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) are common risks. Dental professionals can be exposed to these pathogens through needlestick injuries, cuts from sharp instruments, or contact with contaminated blood and saliva. 6
In addition, procedures like ultrasonic scaling or drilling generate aerosols, tiny droplets that may contain bacteria or viruses. These aerosols can transmit infections, including respiratory diseases. The COVID-19 pandemic highlighted how easily dental professionals could be exposed to airborne viruses if proper precautions are not followed. Using personal protective equipment (PPE), masks, gloves, and eye protection, along with good ventilation, is essential to reduce these risks. 7
3.2. Physical HazardsPhysical hazards in dentistry include radiation, noise, and eye injuries. Dental X-rays are an important diagnostic tool, but repeated exposure can harm dental staff if safety measures are not used. Protective equipment such as lead aprons and thyroid collars help limit radiation risks. High-speed handpieces and suction devices produce noise, which over time may cause hearing problems. Eye injuries can occur from splashes, flying debris, or accidental contact with instruments. Regular safety training and use of protective eyewear help prevent these hazards. 8
3.3. Chemical HazardsDental professionals frequently work with chemicals and materials that can be harmful if handled improperly. These include mercury in dental amalgam, acrylic resins, and disinfectants. Prolonged exposure can cause skin irritation, respiratory problems, or other toxic effects. Some chemicals and gloves may also cause allergic reactions, such as contact dermatitis. Using safer materials, proper handling procedures, and protective equipment like gloves and masks are essential for minimizing these risks. 9, 10
3.4. Ergonomic HazardsErgonomic hazards are related to the physical strain of dental work. Dentists, hygienists, and assistants often maintain awkward postures, lean forward for long periods, and perform repetitive hand movements. These activities can cause musculoskeletal disorders, affecting the back, neck, shoulders, and wrists, and repetitive strain injuries like carpal tunnel syndrome. Research shows that a majority of dental professionals in the United States experience musculoskeletal pain at some point in their careers. Ergonomic interventions such as proper chair height, correct posture, and stretching exercises are recommended to reduce these hazards. 11
3.5. Psychosocial HazardsPsychosocial hazards involve mental and emotional stress. Dentists and dental staff often face high workloads, tight schedules, patient anxiety, and administrative pressures. These factors can lead to stress, burnout, anxiety, and emotional exhaustion. Managing psychosocial hazards requires workload balance, mental health support, and a positive workplace environment. Addressing these risks is important not only for the well-being of dental professionals but also for maintaining the quality of patient care. 12 Table 1 Figure 1
In addition to traditional classification of occupational hazards, integrating these risks within the context of routine clinical procedures provides a more practical understanding of how exposures occur in dental settings. Several high-impact hazards frequently encountered in daily practice include needlestick injuries, aerosol exposure, and musculoskeletal strain associated with clinical and laboratory work.
Needlestick injuries commonly occur during administration of local anesthesia, instrument handling, or operatory cleanup. These incidents primarily affect dentists and dental assistants and pose a significant risk of exposure to bloodborne pathogens such as hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV). Adherence to Occupational Safety and Health Administration (OSHA) and Centers for Disease Control and Prevention (CDC) guidelines is essential, including proper sharps handling, disposal protocols, and post-exposure management. The use of safety-engineered devices, ongoing staff training, and appropriate personal protective equipment (PPE) significantly reduce the risk of injury. 12
Aerosol exposure is another critical hazard generated during procedures such as ultrasonic scaling, tooth preparation, and air polishing. These aerosols may contain bacteria, viruses, and other microorganisms, increasing the risk of respiratory infections among dental professionals. Infection control guidelines emphasize the use of PPE, high-volume evacuation systems, and adequate ventilation. Advanced mitigation strategies, including high-efficiency air filtration and enhanced suction systems, further reduce airborne contamination in clinical environments. 13
Musculoskeletal disorders, particularly in prosthodontic and laboratory settings, develop due to prolonged static postures, repetitive movements, and precision-based tasks. These conditions commonly affect the neck, back, shoulders, and wrists, contributing to chronic pain and reduced professional longevity. Ergonomic recommendations include proper operator positioning, optimal equipment layout, and incorporation of regular breaks. The use of ergonomically designed instruments and workflow modifications can substantially reduce physical strain and improve occupational health outcomes. 13
Occupational hazards are widely reported among dental professionals in the United States, with varying prevalence depending on the type of hazard. Biological exposures, particularly needlestick and sharps injuries, remain a significant concern. Studies indicate that approximately 20-30% of dental professionals experience at least one needlestick injury annually, placing them at risk for bloodborne infections such as hepatitis B, hepatitis C, and HIV. Despite vaccination programs and infection control guidelines from the Centers for Disease Control and Prevention, underreporting of such incidents remains an issue. 13
Ergonomic hazards are among the most prevalent occupational problems in dentistry. Research conducted in the U.S. shows that more than 60% of dentists and dental hygienists report musculoskeletal pain, particularly affecting the neck, back, and shoulders. These conditions often develop early in professional careers and may worsen over time if preventive measures are not implemented. 14
Chemical exposures, including contact with disinfectants, latex, and dental materials, have also been documented. Studies report that 10-15% of dental personnel experience work-related skin conditions, such as contact dermatitis. Physical hazards such as radiation exposure are generally well-controlled in the United States due to strict regulatory standards, although cumulative exposure remains a concern in poorly monitored settings. 15
Psychosocial hazards are increasingly recognized, with surveys indicating that a substantial proportion of U.S. dentists experience moderate to high levels of stress and burnout, particularly in private practice settings. These findings highlight the multifactorial nature of occupational risks in dentistry. 16
4.2. Trends over TimeOver the past few decades, there have been notable improvements in the management of occupational hazards in U.S. dentistry. The introduction of universal precautions and the enforcement of safety regulations by the OSHA have significantly reduced the incidence of bloodborne infections among healthcare workers. Vaccination against hepatitis B and the routine use of personal protective equipment (PPE) have also contributed to safer clinical environments. 17
However, while biological risks have decreased, ergonomic and psychosocial hazards have shown an increasing trend. The growing demand for dental services, longer working hours, and advancements in technology requiring precision work have contributed to higher rates of musculoskeletal disorders and occupational stress. Additionally, the COVID-19 pandemic brought renewed attention to aerosol-related risks and infection control practices, leading to stricter guidelines and enhanced awareness. 18
4.3. High-Risk GroupsCertain groups within the dental workforce are at higher risk of occupational hazards. Dentists, due to their leadership role in clinical procedures, face exposure to a wide range of hazards, including biological, ergonomic, and psychosocial risks. However, dental hygienists are particularly vulnerable to musculoskeletal disorders because of repetitive scaling procedures and prolonged static postures. 19
Dental assistants are another high-risk group, often experiencing frequent exposure to biological hazards and sharps injuries due to instrument handling and chairside assistance. Studies suggest that assistants may have higher rates of needlestick injuries compared to dentists, partly due to differences in training and task allocation. Younger professionals and those in early career stages may also be at increased risk due to limited experience and inadequate ergonomic practices. Additionally, professionals working in high-volume practices or underserved areas may face greater workload pressures, increasing their susceptibility to both physical and psychosocial hazards. 20
Occupational hazards in dentistry are influenced by multiple risk factors that can be broadly categorized into individual, workplace, and procedural factors. These factors often interact with each other, increasing the likelihood of exposure to physical, biological, chemical, ergonomic, and psychosocial risks among dental professionals in the United States.
5.1. Individual FactorsIndividual characteristics such as age, clinical experience, and posture play a significant role in determining susceptibility to occupational hazards. Age is an important factor, as older dental professionals are more likely to experience chronic conditions such as musculoskeletal disorders due to cumulative exposure over time. Conversely, younger or less experienced practitioners may be at higher risk of biological hazards, such as needlestick injuries, due to limited clinical skills and unfamiliarity with safety protocols. 21
Clinical experience also influences risk levels. Experienced professionals tend to develop better infection control practices and ergonomic techniques, reducing their exposure to hazards. However, long years of practice may also contribute to repetitive strain injuries and chronic pain. Posture is one of the most critical individual risk factors in dentistry. Poor working posture, such as prolonged bending, twisting, or leaning over patients, can lead to significant strain on the neck, back, and shoulders. Over time, this can result in musculoskeletal disorders, which are among the most commonly reported occupational health issues in dental professionals. Awareness and training in proper ergonomic posture are essential to minimize these risks. 22
5.2. Workplace FactorsWorkplace conditions, including clinic design, workload, and availability of appropriate equipment, significantly influence occupational risk. Poorly designed dental clinics that lack adequate space, lighting, or ventilation can increase the likelihood of both physical and biological hazards. For example, inadequate ventilation may contribute to the accumulation of aerosols, increasing the risk of airborne infections. 23
Workload is another critical factor. High patient volume, long working hours, and limited breaks can lead to fatigue, stress, and decreased attention to safety protocols. This increases the risk of errors, injuries, and burnout among dental professionals. The type and quality of equipment used in dental practice also play an important role. Outdated or poorly maintained equipment can increase exposure to physical hazards such as noise and vibration, as well as ergonomic strain. In contrast, modern ergonomic dental chairs, adjustable instruments, and advanced suction systems can significantly reduce occupational risks. Adherence to safety standards recommended by organizations such as OSHA is essential for maintaining a safe workplace environment. 24
5.3. Procedural FactorsThe nature, complexity, and duration of dental procedures are key determinants of occupational risk. Certain procedures, such as ultrasonic scaling, tooth preparation, and surgical interventions, generate aerosols and increase exposure to biological hazards. These procedures require strict adherence to infection control protocols to minimize risk.
The duration of procedures is also an important factor. Long or repetitive procedures can lead to prolonged static postures and repetitive hand movements, increasing the risk of musculoskeletal disorders and fatigue. Additionally, extended exposure to noise, vibration, or chemicals during lengthy procedures can contribute to cumulative health effects.
Complex procedures that require high precision and concentration may also contribute to psychological stress, particularly when performed under time constraints. This highlights the need for proper scheduling, adequate rest periods, and the use of advanced technologies to reduce physical and mental strain. 25
Despite significant advancements in occupational safety in dental practice, several persistent challenges and gaps in the United States limit the effectiveness of preventive strategies. These challenges span reporting, compliance, education, and policy adaptation.
6.1. Underreporting of Occupational HazardsOne of the most critical issues is the underreporting of occupational hazards, including needlestick injuries, minor exposures to infectious materials, and work-related musculoskeletal disorders. Many dental professionals do not report these events due to time constraints in fast-paced clinical environments, where patient care is prioritized over administrative tasks. Fear of professional consequences, such as legal liability, reputational damage, or disciplinary action, also discourages reporting. Additionally, the normalization of risk leads many practitioners to view minor injuries or discomfort as routine aspects of dental practice, resulting in them going unreported. This underreporting creates an incomplete understanding of occupational risks and limits the development of effective, evidence-based interventions. 26
6.2. Inconsistent Compliance with Safety GuidelinesAnother major challenge is inconsistent adherence to established safety protocols. Although regulatory bodies provide comprehensive standards for infection control, radiation safety, and ergonomics, implementation varies across dental settings. Resource limitations in smaller practices may restrict the ability to adopt all recommended measures. Training gaps and limited access to continuing education can further hinder proper implementation. In addition, the lack of systematic monitoring, auditing, and feedback mechanisms allows lapses in safety practices to persist. These inconsistencies contribute to preventable exposures and injuries, highlighting the need for stronger compliance support and oversight. 27
6.3. Need for Policy Updates and Continuous EducationRapid technological advancements, emerging infectious diseases, and evolving workforce dynamics require continuous updates to occupational safety policies. However, delays in policy revision often mean that guidelines do not reflect the latest scientific evidence or innovations. Access to ongoing training is not uniform, leaving some professionals without up-to-date knowledge of emerging risks and preventive strategies. Even when updated guidelines are available, integrating them into daily clinical workflows can be difficult without structured programs and incentives. Addressing these challenges requires systematic approaches to both policy updates and lifelong professional learning. 28
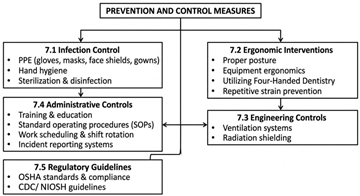
Mitigating occupational hazards in dentistry requires proactive and integrated strategies involving research, policy development, technological advancement, and education.
7.1. Strengthening Research and SurveillanceFurther research is necessary to better understand the prevalence, long-term effects, and emerging trends of occupational hazards among dental professionals in the United States. Longitudinal studies can provide valuable insights into chronic risks by tracking exposures and health outcomes over time. Standardized reporting systems are essential to improve data consistency and enable meaningful comparisons across different settings. Additionally, greater attention to psychosocial hazards such as stress and burnout can help reveal indirect impacts on safety and professional performance. Strengthening research and surveillance systems will support more effective and targeted interventions. 29
7.2. Policy Improvements and Regulatory OversightStrong and adaptive policies are essential for ensuring consistent implementation of safety measures. Enhancing enforcement of existing regulations can improve compliance with established standards. Standardizing reporting requirements can reduce variability and strengthen hazard tracking systems. Policies must also evolve to address emerging risks, including airborne disease transmission and ergonomic concerns. A forward-looking regulatory framework can help bridge current gaps and better protect dental professionals. 30
In addition to national and organizational policy improvements, effective implementation of occupational safety measures requires active engagement at the clinic level. Dental practices can strengthen compliance and awareness by conducting regular in-house training sessions, seminars, and workshops that keep staff updated on evolving safety guidelines and emerging risks. These sessions provide opportunities for open communication, allowing dental professionals and support staff to share experiences, discuss challenges, and identify gaps in current practices. Establishing routine safety meetings and feedback mechanisms can foster a culture of continuous improvement and accountability within clinical settings. Furthermore, integrating periodic refresher training and practical demonstrations into daily workflows ensures that safety protocols are not only understood but consistently applied. Such clinic-based initiatives complement broader policy frameworks and play a critical role in translating guidelines into effective day-to-day practice. 31
7.3. Technological Innovations for SafetyTechnological advancements provide practical solutions for reducing occupational hazards in dental practice. Ergonomically designed equipment can help minimize physical strain and prevent musculoskeletal injuries. Innovations in imaging technology, such as low-radiation systems, improve protection against ionizing radiation. Improved aerosol management through advanced suction, air filtration, and ventilation systems reduces exposure to airborne pathogens. Automation and artificial intelligence can streamline repetitive tasks, enhancing precision while reducing fatigue. These innovations complement traditional safety measures and contribute to a safer clinical environment. 32
7.4. Education and Awareness ProgramsEducation plays a crucial role in fostering a culture of safety within dental practice. Integrating occupational health and safety into dental curricula ensures that new professionals are well-prepared. Continuing professional development opportunities, including workshops and online learning, help practitioners stay informed about emerging risks. Promoting a strong institutional safety culture encourages reporting, regular audits, and peer support, reinforcing adherence to safety protocols. Sustained educational efforts are essential for improving awareness, compliance, and overall occupational safety. 33
This review highlights the diverse range of occupational hazards faced by dental professionals in the United States, including biological, physical, chemical, ergonomic, and psychosocial risks. These hazards are influenced by multiple factors such as individual characteristics, workplace conditions, and procedural demands, making them complex and interrelated.
The findings emphasize the critical importance of preventive strategies, including adherence to infection control guidelines, implementation of ergonomic practices, proper use of protective equipment, and attention to mental well-being. While significant progress has been made in reducing certain risks, particularly biological hazards, other concerns such as musculoskeletal disorders and occupational stress continue to pose substantial challenges.
In conclusion, improving occupational safety in dentistry requires a comprehensive and sustained effort involving research, policy development, technological innovation, and education. By addressing existing gaps and promoting a proactive approach to risk management, it is possible to enhance the health and well-being of dental professionals while ensuring high-quality patient care.
| [1] | Guven Y. Scientific basis of dentistry. J Istanb Univ Fac Dent. 2017 Oct 2; 51(3): 64-71. | ||
| In article | |||
| [2] | Ayatollahi J, Ayatollahi F, Ardekani AM, Bahrololoomi R, Ayatollahi J, Ayatollahi A, Owlia MB. Occupational hazards to dental staff. Dent Res J (Isfahan). 2012 Jan; 9(1): 2-7. | ||
| In article | View Article PubMed | ||
| [3] | National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Division of Behavioral and Social Sciences and Education; Committee on National Statistics; Division on Earth and Life Studies; Board on Agriculture and Natural Resources; Committee on Developing a Smarter National Surveillance System for Occupational Safety and Health in the 21st Century. A Smarter National Surveillance System for Occupational Safety and Health in the 21st Century. Washington (DC): National Academies Press (US); 2018 Oct 9. 4, Current Status of Federal and State Programs and Cross-cutting Issues. Available from: https: // www. ncbi.nlm.nih.gov/books/NBK493427/. | ||
| In article | |||
| [4] | Institute of Medicine (US) Committee to Assess Training Needs for Occupational Safety and Health Personnel in the United States. Safe Work in the 21st Century: Education and Training Needs for the Next Decade's Occupational Safety and Health Personnel. Washington (DC): National Academies Press (US); 2000. 2, Occupational Safety and Health Professionals. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK225528/. | ||
| In article | |||
| [5] | Denault D, Gardner H. OSHA Bloodborne Pathogen Standards. [Updated 2023 Jul 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK570561/. | ||
| In article | |||
| [6] | Săndulescu M, Nicolescu MI, Funieru C, Şahin GÖ, Săndulescu O; ESCMID Study Group for Viral Hepatitis (ESGVH). Exposure to Biological Fluids in Dental Practice-Narrative Review on Appropriate Risk Assessment to Guide Post-Exposure Management. Pathogens. 2023 Jul 24; 12(7): 968. | ||
| In article | View Article PubMed | ||
| [7] | U.S. Public Health Service. Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis. MMWR Recomm Rep. 2001 Jun 29; 50(RR-11): 1-52. PMID: 11442229. | ||
| In article | |||
| [8] | Alamri A, ElSharkawy MF, Alafandi D. Occupational Physical Hazards and Safety Practices at Dental Clinics. Eur J Dent. 2023 May; 17(2): 439-449. | ||
| In article | View Article PubMed | ||
| [9] | Leggat PA, Kedjarune U, Smith DR. Occupational health problems in modern dentistry: a review. Ind Health. 2007 Oct; 45(5): 611-21. | ||
| In article | View Article PubMed | ||
| [10] | Moodley R, Naidoo S, Wyk JV. The prevalence of occupational health-related problems in dentistry: A review of the literature. J Occup Health. 2018 Mar 27; 60(2): 111-125. | ||
| In article | View Article PubMed | ||
| [11] | Lietz J, Kozak A, Nienhaus A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS One. 2018 Dec 18; 13(12): e0208628. | ||
| In article | View Article PubMed | ||
| [12] | Maragha T, Atanackovic J, Adams T, Brondani M, Bourgeault I. Dentists' Mental Health: Challenges, Supports, and Promising Practices. JDR Clin Trans Res. 2025 Apr; 10(2): 100-111. | ||
| In article | View Article PubMed | ||
| [13] | Cleveland JL, Bonito AJ, Corley TJ, Foster M, Barker L, Brown GG, Lenfestey N, Lux L. Advancing infection control in dental care settings: factors associated with dentists' implementation of guidelines from the Centers for Disease Control and Prevention. J Am Dent Assoc. 2012 Oct; 143(10): 1127-38. | ||
| In article | View Article PubMed | ||
| [14] | Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009 Aug; 7(3): 159-65. | ||
| In article | View Article PubMed | ||
| [15] | Siew C, Gruninger SE, Miaw CL, Neidle EA. Percutaneous injuries in practicing dentists. A prospective study using a 20-day diary. J Am Dent Assoc. 1995 Sep; 126(9): 1227-34. | ||
| In article | View Article PubMed | ||
| [16] | Dobson M, Schnall P, Faghri P, Landsbergis P. The Healthy Work Survey: A Standardized Questionnaire for the Assessment of Workplace Psychosocial Hazards and Work Organization in the United States. J Occup Environ Med. 2023 May 1; 65(5): e330-e345. | ||
| In article | View Article PubMed | ||
| [17] | Estrich CG, Mikkelsen M, Morrissey R, Geisinger ML, Ioannidou E, Vujicic M, Araujo MWB. Estimating COVID-19 prevalence and infection control practices among US dentists. J Am Dent Assoc. 2020 Nov; 151(11): 815-824. | ||
| In article | View Article PubMed | ||
| [18] | AlDhaen E. Awareness of occupational health hazards and occupational stress among dental care professionals: Evidence from the GCC region. Front Public Health. 2022 Sep 8; 10: 922748. | ||
| In article | View Article PubMed | ||
| [19] | Saccucci M, Zumbo G, Mercuri P, Pranno N, Sotero S, Zara F, Vozza I. Musculoskeletal disorders related to dental hygienist profession. Int J Dent Hyg. 2022 Aug; 20(3): 571-579. | ||
| In article | View Article PubMed | ||
| [20] | Pantea Kaviandost, Sohail Vyas, Kiranprasad Chileveru, Sruthi Kalakota, Layal Touchan, Amit Malik, Sandeep Singh (2025). Posture, Precision, and Prevention: A Comprehensive Review of Dental Ergonomics. Saudi J Oral Dent Res, 10(5): 248-254. | ||
| In article | |||
| [21] | Kamal F, Anwari A, Ghazanfari F, Khairzad AA, Sharifi N, Omarzad F. Assessing Knowledge and Awareness of Occupational Hazards and Preventive Measures among Dentists and Final-year Students in Two Dentistry Hospitals, Kabul, Afghanistan. F1000Res. 2025 Sep 9; 14: 639. | ||
| In article | View Article PubMed | ||
| [22] | Sivakumar I, Arunachalam KS, Solomon E. Occupational health hazards in a prosthodontic practice: review of risk factors and management strategies. J Adv Prosthodont. 2012 Nov; 4(4): 259-65. | ||
| In article | View Article PubMed | ||
| [23] | Choosong T, Kaimook W, Tantisarasart R, Sooksamear P, Chayaphum S, Kongkamol C, Srisintorn W, Phakthongsuk P. Noise exposure assessment in a dental school. Saf Health Work. 2011 Dec; 2(4): 348-5. | ||
| In article | View Article PubMed | ||
| [24] | Xu J, Pan P, Song F, Gu Y, Xiong Q, Liu Z, Zhou Y. Analyzing the occupational exposure risks of dental healthcare workers from the perspective of repeated occupational exposure. BMC Health Serv Res. 2024 Nov 11; 24(1): 1377. | ||
| In article | View Article PubMed | ||
| [25] | Matys J, Grzech-Leśniak K. Dental Aerosol as a Hazard Risk for Dental Workers. Materials (Basel). 2020 Nov 12; 13(22): 5109. | ||
| In article | View Article PubMed | ||
| [26] | Institute of Medicine (US) Board on Health Care Services. The U.S. Oral Health Workforce in the Coming Decade: Workshop Summary. Washington (DC): National Academies Press (US); 2009. 7, Challenges of the Current System. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK219680/. | ||
| In article | |||
| [27] | Dr. Latifa Elbanna, Dr. Sri Valli Durga Bala Vinuthna Darisipudi, Dr. Deepthi Dandu, Dr. Sree Rekha Movva, Dr. Sameera A Khan, Dr. Anam fazal, and Dr. Sandeep Singh, “Infection Control in U.S. Dental Practice: Current Standards, Guidelines, and Emerging Challenges.” American Journal of Medical Case Reports, vol. 14, no. 3 (2026): 34-41. | ||
| In article | View Article | ||
| [28] | Houser SH, Crew D, Flite CA, Goethals C. Shaping the Future of the Health Information Profession: The Impact of Emerging Technologies on the Workforce. Adv Health Inf Sci Pract. 2025 Aug 11; 1(2): RBQG5825. | ||
| In article | View Article | ||
| [29] | Căminișteanu F, Vorovenci A, Perieanu VȘ, Petri SA, Burlibașa L, David M, Drăguș AC, Burlibașa M. Occupational diseases among dental personnel: a scoping review. J Med Life. 2025 Jun; 18(6): 526-535. | ||
| In article | |||
| [30] | Dunbar P, Keyes LM, Browne JP. Determinants of regulatory compliance in health and social care services: A systematic review using the Consolidated Framework for Implementation Research. PLoS One. 2023 Apr 13; 18(4): e0278007. | ||
| In article | View Article PubMed | ||
| [31] | Sakchhi S, Elbanna L, Chakor M, Nikferjam A Z, Saeedi N, Badve S, SinghS. Green Dentistry: Sustainable Practices and Materials for a Healthier Planet. Int J Dent Mater. 2025; 7(3): 84-92. | ||
| In article | View Article | ||
| [32] | Dodoo JE, Al-Samarraie H, Alzahrani AI, Lonsdale M, Alalwan N. Digital Innovations for Occupational Safety: Empowering Workers in Hazardous Environments. Workplace Health Saf. 2024 Mar; 72(3): 84-95. | ||
| In article | View Article PubMed | ||
| [33] | Cvijic A, Kvernenes M, Åstrøm A, Tsilingaridis G, Bletsa A. Approaches to Continuing Professional Development in Dental Traumatology-A Qualitative Study of General Dentists' Experiences. Dent Traumatol. 2026 Feb; 42(1): 32-41. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2026 Dr. Kiranprasad Chileveru, Dr. Latifa Elbanna, Dr. Robinpreet Kaur, Dr. Chandni Sodha, Dr. Vattaluri Ankannagari Dishitha, Dr. Riya Ashish Patel, Dr. Ridhi Bhola and Dr. Sandeep Singh
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Guven Y. Scientific basis of dentistry. J Istanb Univ Fac Dent. 2017 Oct 2; 51(3): 64-71. | ||
| In article | |||
| [2] | Ayatollahi J, Ayatollahi F, Ardekani AM, Bahrololoomi R, Ayatollahi J, Ayatollahi A, Owlia MB. Occupational hazards to dental staff. Dent Res J (Isfahan). 2012 Jan; 9(1): 2-7. | ||
| In article | View Article PubMed | ||
| [3] | National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Division of Behavioral and Social Sciences and Education; Committee on National Statistics; Division on Earth and Life Studies; Board on Agriculture and Natural Resources; Committee on Developing a Smarter National Surveillance System for Occupational Safety and Health in the 21st Century. A Smarter National Surveillance System for Occupational Safety and Health in the 21st Century. Washington (DC): National Academies Press (US); 2018 Oct 9. 4, Current Status of Federal and State Programs and Cross-cutting Issues. Available from: https: // www. ncbi.nlm.nih.gov/books/NBK493427/. | ||
| In article | |||
| [4] | Institute of Medicine (US) Committee to Assess Training Needs for Occupational Safety and Health Personnel in the United States. Safe Work in the 21st Century: Education and Training Needs for the Next Decade's Occupational Safety and Health Personnel. Washington (DC): National Academies Press (US); 2000. 2, Occupational Safety and Health Professionals. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK225528/. | ||
| In article | |||
| [5] | Denault D, Gardner H. OSHA Bloodborne Pathogen Standards. [Updated 2023 Jul 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK570561/. | ||
| In article | |||
| [6] | Săndulescu M, Nicolescu MI, Funieru C, Şahin GÖ, Săndulescu O; ESCMID Study Group for Viral Hepatitis (ESGVH). Exposure to Biological Fluids in Dental Practice-Narrative Review on Appropriate Risk Assessment to Guide Post-Exposure Management. Pathogens. 2023 Jul 24; 12(7): 968. | ||
| In article | View Article PubMed | ||
| [7] | U.S. Public Health Service. Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis. MMWR Recomm Rep. 2001 Jun 29; 50(RR-11): 1-52. PMID: 11442229. | ||
| In article | |||
| [8] | Alamri A, ElSharkawy MF, Alafandi D. Occupational Physical Hazards and Safety Practices at Dental Clinics. Eur J Dent. 2023 May; 17(2): 439-449. | ||
| In article | View Article PubMed | ||
| [9] | Leggat PA, Kedjarune U, Smith DR. Occupational health problems in modern dentistry: a review. Ind Health. 2007 Oct; 45(5): 611-21. | ||
| In article | View Article PubMed | ||
| [10] | Moodley R, Naidoo S, Wyk JV. The prevalence of occupational health-related problems in dentistry: A review of the literature. J Occup Health. 2018 Mar 27; 60(2): 111-125. | ||
| In article | View Article PubMed | ||
| [11] | Lietz J, Kozak A, Nienhaus A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS One. 2018 Dec 18; 13(12): e0208628. | ||
| In article | View Article PubMed | ||
| [12] | Maragha T, Atanackovic J, Adams T, Brondani M, Bourgeault I. Dentists' Mental Health: Challenges, Supports, and Promising Practices. JDR Clin Trans Res. 2025 Apr; 10(2): 100-111. | ||
| In article | View Article PubMed | ||
| [13] | Cleveland JL, Bonito AJ, Corley TJ, Foster M, Barker L, Brown GG, Lenfestey N, Lux L. Advancing infection control in dental care settings: factors associated with dentists' implementation of guidelines from the Centers for Disease Control and Prevention. J Am Dent Assoc. 2012 Oct; 143(10): 1127-38. | ||
| In article | View Article PubMed | ||
| [14] | Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009 Aug; 7(3): 159-65. | ||
| In article | View Article PubMed | ||
| [15] | Siew C, Gruninger SE, Miaw CL, Neidle EA. Percutaneous injuries in practicing dentists. A prospective study using a 20-day diary. J Am Dent Assoc. 1995 Sep; 126(9): 1227-34. | ||
| In article | View Article PubMed | ||
| [16] | Dobson M, Schnall P, Faghri P, Landsbergis P. The Healthy Work Survey: A Standardized Questionnaire for the Assessment of Workplace Psychosocial Hazards and Work Organization in the United States. J Occup Environ Med. 2023 May 1; 65(5): e330-e345. | ||
| In article | View Article PubMed | ||
| [17] | Estrich CG, Mikkelsen M, Morrissey R, Geisinger ML, Ioannidou E, Vujicic M, Araujo MWB. Estimating COVID-19 prevalence and infection control practices among US dentists. J Am Dent Assoc. 2020 Nov; 151(11): 815-824. | ||
| In article | View Article PubMed | ||
| [18] | AlDhaen E. Awareness of occupational health hazards and occupational stress among dental care professionals: Evidence from the GCC region. Front Public Health. 2022 Sep 8; 10: 922748. | ||
| In article | View Article PubMed | ||
| [19] | Saccucci M, Zumbo G, Mercuri P, Pranno N, Sotero S, Zara F, Vozza I. Musculoskeletal disorders related to dental hygienist profession. Int J Dent Hyg. 2022 Aug; 20(3): 571-579. | ||
| In article | View Article PubMed | ||
| [20] | Pantea Kaviandost, Sohail Vyas, Kiranprasad Chileveru, Sruthi Kalakota, Layal Touchan, Amit Malik, Sandeep Singh (2025). Posture, Precision, and Prevention: A Comprehensive Review of Dental Ergonomics. Saudi J Oral Dent Res, 10(5): 248-254. | ||
| In article | |||
| [21] | Kamal F, Anwari A, Ghazanfari F, Khairzad AA, Sharifi N, Omarzad F. Assessing Knowledge and Awareness of Occupational Hazards and Preventive Measures among Dentists and Final-year Students in Two Dentistry Hospitals, Kabul, Afghanistan. F1000Res. 2025 Sep 9; 14: 639. | ||
| In article | View Article PubMed | ||
| [22] | Sivakumar I, Arunachalam KS, Solomon E. Occupational health hazards in a prosthodontic practice: review of risk factors and management strategies. J Adv Prosthodont. 2012 Nov; 4(4): 259-65. | ||
| In article | View Article PubMed | ||
| [23] | Choosong T, Kaimook W, Tantisarasart R, Sooksamear P, Chayaphum S, Kongkamol C, Srisintorn W, Phakthongsuk P. Noise exposure assessment in a dental school. Saf Health Work. 2011 Dec; 2(4): 348-5. | ||
| In article | View Article PubMed | ||
| [24] | Xu J, Pan P, Song F, Gu Y, Xiong Q, Liu Z, Zhou Y. Analyzing the occupational exposure risks of dental healthcare workers from the perspective of repeated occupational exposure. BMC Health Serv Res. 2024 Nov 11; 24(1): 1377. | ||
| In article | View Article PubMed | ||
| [25] | Matys J, Grzech-Leśniak K. Dental Aerosol as a Hazard Risk for Dental Workers. Materials (Basel). 2020 Nov 12; 13(22): 5109. | ||
| In article | View Article PubMed | ||
| [26] | Institute of Medicine (US) Board on Health Care Services. The U.S. Oral Health Workforce in the Coming Decade: Workshop Summary. Washington (DC): National Academies Press (US); 2009. 7, Challenges of the Current System. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK219680/. | ||
| In article | |||
| [27] | Dr. Latifa Elbanna, Dr. Sri Valli Durga Bala Vinuthna Darisipudi, Dr. Deepthi Dandu, Dr. Sree Rekha Movva, Dr. Sameera A Khan, Dr. Anam fazal, and Dr. Sandeep Singh, “Infection Control in U.S. Dental Practice: Current Standards, Guidelines, and Emerging Challenges.” American Journal of Medical Case Reports, vol. 14, no. 3 (2026): 34-41. | ||
| In article | View Article | ||
| [28] | Houser SH, Crew D, Flite CA, Goethals C. Shaping the Future of the Health Information Profession: The Impact of Emerging Technologies on the Workforce. Adv Health Inf Sci Pract. 2025 Aug 11; 1(2): RBQG5825. | ||
| In article | View Article | ||
| [29] | Căminișteanu F, Vorovenci A, Perieanu VȘ, Petri SA, Burlibașa L, David M, Drăguș AC, Burlibașa M. Occupational diseases among dental personnel: a scoping review. J Med Life. 2025 Jun; 18(6): 526-535. | ||
| In article | |||
| [30] | Dunbar P, Keyes LM, Browne JP. Determinants of regulatory compliance in health and social care services: A systematic review using the Consolidated Framework for Implementation Research. PLoS One. 2023 Apr 13; 18(4): e0278007. | ||
| In article | View Article PubMed | ||
| [31] | Sakchhi S, Elbanna L, Chakor M, Nikferjam A Z, Saeedi N, Badve S, SinghS. Green Dentistry: Sustainable Practices and Materials for a Healthier Planet. Int J Dent Mater. 2025; 7(3): 84-92. | ||
| In article | View Article | ||
| [32] | Dodoo JE, Al-Samarraie H, Alzahrani AI, Lonsdale M, Alalwan N. Digital Innovations for Occupational Safety: Empowering Workers in Hazardous Environments. Workplace Health Saf. 2024 Mar; 72(3): 84-95. | ||
| In article | View Article PubMed | ||
| [33] | Cvijic A, Kvernenes M, Åstrøm A, Tsilingaridis G, Bletsa A. Approaches to Continuing Professional Development in Dental Traumatology-A Qualitative Study of General Dentists' Experiences. Dent Traumatol. 2026 Feb; 42(1): 32-41. | ||
| In article | View Article PubMed | ||



{kind=link}