Diabetes is a major public health problem, due to its high and growing prevalence on the one hand, and its socio-economic impact on the other. Correcting this disease relies on glycemic control, particularly through medication. The majority of African populations are attached to the use of traditional herbal treatments, due to the high cost of modern treatments. The aim of this study is to demonstrate the anti-hyperglycemic activity of M. Charantia leaf extract, its corrective effect on streptozotocin-induced pancreatic lesions and its anti-glucose activity.Phytochemical screening was carried out on the extract and on extraction by the maceration method. Diabetes was induced in rats by injection of five doses of streptozotocin (40 mg/kg) body weight. Efficacy in animals was tested by treating them with the extracts for 28 consecutive days at 10mg/L. Biochemical and hematological parameters were measured by spectrophotometer and hematology apparatus respectively. Histological studies were carried out by fixing pancreases with a 10% formalin solution and staining with hematoxylin-eosin (HE).Phytochemical analysis of the plant revealed that the leafy stem is very rich in secondary metabolites (9 groups). In the efficacy test, leaf extract reduced cholesterol levels, and regulated triglyceridemia and white blood cell count. Leaf extract restored islet lesions in the pancreas.
Diabetes is a major public health problem due to its significant and growing prevalence on the one hand, and its socio-economic impact on the other. (Schlosser, 2019). It is chronic and occurs when the pancreas does not produce enough insulin, or when the body is unable to effectively use the insulin, it does produce, leading to hyperglycemia. Hyperglycemia is a common effect of unmanaged diabetes, which over time leads to severe damage to many parts of the body, particularly nerves and blood vessels 1. According to global estimates for 2021, diabetes affects more than 537 million people worldwide (or 1 in 10), including 61 million in Europe (source: International Diabetes Federation Atlas 2021). The latest estimates from the International Diabetes Federation (IDF/IDF), reveals that the number of diabetics in Africa will almost triple between 2017 and 2045, rising from 16 million to 41 million 2. The prevalence of diabetes rose from 1.26 in 2008 to 3.30% in 2015 3. Type I diabetes, formerly known as insulin-dependent or juvenile diabetes 1, mainly affects children and young adults. It is caused by progressive autoimmune destruction of the b islets of the pancreas responsible for endogenous insulin secretion ensuring carbohydrate homeostasis under physiological conditions 4. Correction of this disease relies on control of blood glucose levels, notably through a healthy diet, and oral medication or insulin. Regular screening is also necessary to detect possible complications (Treatments European Center for the Study of Diabetes) (ceed-diabete.org).
Despite the availability of insulin as a drug treatment for type 1 diabetes, the majority of people in Africa continue to rely on traditional herbal treatments due to the high cost of modern therapy. The use of medicinal plants is growing rapidly in most countries of the world, based in particular on the idea that plants are a natural means of treatment that is risk-free 5 and easily accessible at low cost. Herbal medicine is enjoying renewed success in more and more countries around the world, including Benin. In addition, many medicinal plants are now used in traditional medicine to treat a wide range of conditions, including diabetes and its complications. This is the case of Momordica Charantia, or bitter melon or African cucumber, whose extracts have been shown to have various medicinal properties, notably anti-hyperglycemic 6, 7. This work aims to demonstrate the component of M. Charantia leaf extract and anti-hyperglycemic activity, the corrective effect of streptozotocin-induced damage to the pancreas and its anti-glucose activity.
The leaves of the plant were collected in November 2021 at Sèmè-Kpodji in the Ouémé department in southeastern Benin, then identified at the Herbier national du Benin at the Université Abomey-Calavi (M. charantia L. Cucurbitaceae).
Preparation of extracts and phytochemical analysisThe leaves were cold-dried (22°C) for around 14 days. Finally, extraction of total chemical principles was carried out using the maceration method, by mixing 50g of drug with 500mL of distilled water on a continuous shaker for 48 hours, according to the method described by Assou et al. (2022). Phytochemical screening was also carried out using staining and precipitation reactions to differentiate the main groups of chemical compounds 8.
Efficacy testM. charantia leaf extract was administered orally to diabetic rats at a dose of 10 mg/kg body weight for 28 consecutive days from diabetes induction (day 12). Biochemical and hematological parameters were determined by taking blood samples from Wistar rats in dry, fluoridated EDTA tubes from the retroorbital sinus throughout the experimental period. Several biochemical parameters (glycemia, creatininemia, cholesterols and triglycerides) were assayed for efficacy. The extract's anti-inflammatory activity was measured by means of a complete blood count, performed using a KX21 automated leukocyte count and hemoglobin assay.
Tissue preparation and histopathological analysisRats were sacrificed after being anesthetized with ether for 5 min at the end of treatment. Organs (pancreas, liver and kidney) were harvested and fixed in 10% buffered formalin. The 5 µm of the organs were sectioned and preserved in tubes. Sections were then stained with hematoxylin and eosin (H&E), following a standard protocol 9.
Statistical analysisBiological parameter results were expressed as the mean. Results of efficacy tests were compared on days 0, 12, 17, 22 or 28 using the Mann Whitney test. A significance level was set at 5%. Photos were captured at 400X magnification.
Ethics statementThe study was approved by the National Research Ethics Committee of Benin. The plant was identified by the Principal Botanist of the National Herbarium of the University of Abomey-Calavi where a specimen of the plant is deposited under the number M. charantia L. Cucurbitaceae: AP2033/HNB. The Wistar rats used in our study were handled in accordance with institutional animal safety guidelines (Animal facility, National School of Biosciences appliquées et Biotechnologies, Université Nationale des Sciences, des technologies, de l'Ingénierie et des Mathématiques, Benin).
Leaf screening revealed that the species studied is very rich in secondary metabolites (9 groups). The organs studied do not contain the toxic chemical groups, namely cyanogenic derivatives. Alkaloids, triterpenes, steroids, mucilages, flavonoids, saponosides and reducing compounds are present in the leafy stems and in one of the fruits. The most frequent chemical groups in the species studied are alkaloids, triterpenes, steroids, mucilages, flavonoids, reducing compounds and saponosides. Polyphenols (catechic tannins, anthocyanins and leuco-anthocyanins) are intrinsic to leafy stems (Table 1).
Treatment of rats with streptozotocin caused a marked change in biochemical parameters (blood glucose, triglycerides, total cholesterol, HDL-cholesterol and creatinine) at D12 compared with values at D0.
Blood glucose and lipidsBlood glucose levels ranged from 1.0 ± 0.15 to 1.05 ± 0.11 g/L in the different groups of rats at D0. It increased significantly with a peak at D12 following treatment of the rats with streptozotocin, thus creating diabetes. Subsequently, blood glucose levels fell significantly and returned to normal from D17 in the insulin-treated group. Hyperglycemia persisted at D28 in the group treated with M. charantia leaf extract and in the untreated diabetic group. In the control group not treated with streptozotocin, blood glucose levels remained normal throughout the experimental period (Figure 1).

Triglyceridemia ranged from 1.34 ± 0.28 to 1.48 ± 0.18 g/L in the different groups of rats at D0. It increased significantly with a peak at D12 following streptozotocin treatment of the rats. It then fell significantly and returned to normal values from D17 in the insulin-treated groups and in the M. charantia leaf extract-treated group. Hypertriglyceridemia persisted at D28 in the untreated diabetic group. In the control group, triglyceridemia was normal throughout the experimental period (Figure 2).

La cholestérolémie totale varie de 1,00 ± 0,27 à 1,16 ± 0,16 g/L dans les différents groupes de rats à J0. Elle augmente à J12, suite au traitement à la streptozotocine. Elle est revenue à sa valeur normale à partir de J17 dans les groupes traités à l'insuline et à l'extrait de feuilles de M. charantia. L'hypercholestérolémie totale persiste à J28 dans le groupe diabétique non traité. Dans le groupe témoin, la cholestérolémie totale est restée normale tout au long de la période expérimentale (Figure 3).

HDL cholesterol levels ranged from 0.41 ± 0.04 to 0.45 ± 0.03 g/L in the different groups of rats at D0. It decreased significantly with a peak at D12 following streptozotocin treatment of the rats, creating HDL hypocholesterolemia. It then increased progressively, returning to normal values from D17 in the insulin-treated group and from D22 in the M. charantia leaf extract-treated group. In the untreated diabetic group, HDL cholesterol returned to normal at D28. In the untreated control group, HDL cholesterol levels did not change significantly over the course of the experiment (Figure 4).

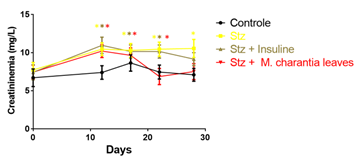
Serum creatinine ranged from 6.7 ± 1.0 to 7.7 ± 0.9 mg/L in the different groups of rats at D0. Serum creatinine increased significantly with a peak at D12 after treatment of rats with streptozotocin, indicating renal distress. It then fell progressively, returning to its values at D28 in the insulin-treated group and in the M. charantia leaf extract-treated group. In the untreated diabetic group, hypercreatininemia persisted until D28. In the untreated control group, serum creatinine did not vary significantly over the course of the experiment (Figure 5).
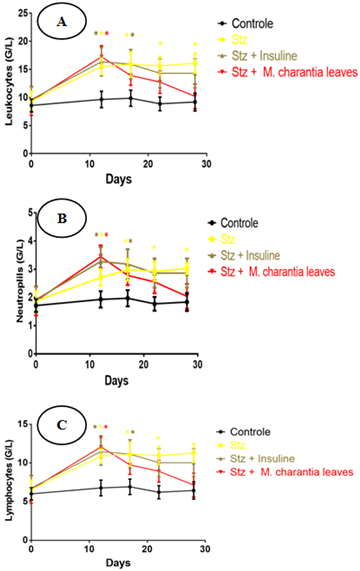
Inflammatory parametersBlood leukocyte counts ranged from 8.6 ± 1.0 to 9.6 ± 2.0 G/L in the different rat groups at D0. It increased significantly with a peak at D12 following treatment of rats with streptozotocin, indicating inflammation. It then decreased progressively, returning to its initial values at D17 in the groups treated with M. charantia leaf extracts and at D22 in the insulin-treated group. In the group of untreated diabetic rats, hyperleukocytosis persisted at D28. In the non-diabetic control group, the number of blood leukocytes did not vary significantly over the course of the experiment (Figure 6A). Neutrophil counts ranged from 1.7 ± 0.2 to 1.9 ± 0.46 G/L in the different rat groups at D0. It increased significantly with a peak at D12 following treatment of the rats with streptozotocin, indicating acute inflammation. It then falls progressively, returning to its initial values at D17 in the group treated with M. charantia leaf extract and at D22 in the insulin-treated groups. In the group of untreated diabetic rats, hyperneutrophilia persisted at D28. In the non-diabetic control group, neutrophil counts did not vary significantly over the course of the experiment (Figure 6B). Blood lymphocyte counts ranged from 6.0 ± 6.7 to 6.7 ± 1.6 G/L in the different groups of rats at D0. It increased significantly with a peak at D12 after treatment of rats with streptozotocin, indicating chronic inflammation. It then decreased progressively, returning to its initial values at D17 in the groups treated with M. charantia leaf extract and at D22 in the insulin-treated group. In the group of untreated diabetic rats, hyperlymphocytosis persisted at D28. In the non-diabetic control group, the number of blood lymphocytes did not vary significantly over the course of the experiment (Figure 6C).
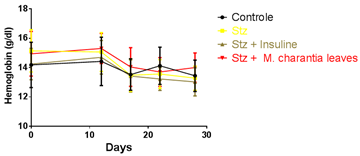
Hemoglobin levels ranged from 14.2 ± 1.4 to 15.1 ± 1.3 g/dL in the different groups of rats at D0. It did not vary significantly in the different diabetic or non-diabetic groups over the course of the experiment, indicating an absence of disturbance in erythrocyte parameters (Figure 7).
Histology of the pancreasIn controls (Figure 8A), endocrine islets of Langerhans (LI) are typical, well surrounded by exocrine pancreatic serous acini. In streptozotocin-treated rats (Figure 8B), islets are altered by cell necrosis (asterisks). In rats treated with streptozotocin, followed by insulin (Figure 8C) and M. charantia leaf extract (Figure 8D), islet architecture is restored.

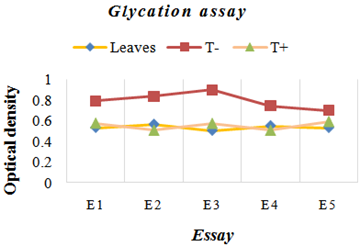
The five tests carried out showed that leaf extract inhibited the glycation reaction in the same way as aminoguanidine (positive control) compared with the negative control.
The use of medicinal plants still suffers from a lack of appropriate scientific research that could support their inclusion in therapy. The mechanism of action of extracts from these plants are poorly studied, particularly that of M. charantia which has been shown to have anti-diabetic properties 10, 11. Our study focused on the different components of M. Charantia leaf extract and its hypoglycemic effect on type I diabetes in rats. The leafy stem was very rich in secondary metabolites (9 groups), with the presence of alkaloids, triterpenes, steroids, mucilages, flavonoids, reducing compounds and saponosides. This composition is similar to that described by Gurav et al. where the phytochemical study revealed the presence of alkaloids, tannins, flavonoids, saponosides, glycosides, terpenoids, carbohydrates and sterols(Gurav, Mondal & Vijayakumar, 2014; Fachinan et al., 2017). However, Samba et al. recently reported that cold-extracted oil retains as many of its physico-chemical properties as possible and contains a very high content of phenolic compounds and anti-free radical activity 14. As for polyphenols (catechic tannins, anthocyanins and leuco-anthocyanins), they were intrinsic to the leafy stems.
Treatment of the different groups with leaf stem extract and insulin led to a correction of blood glucose levels only in the insulin group. Our work has shown that the traditional use of M. charantia leaf remains ineffective against type 1 diabetes, particularly in reducing blood sugar levels. This observation can be explained by the low presence of flavonoids.
The triglyceride-lowering action of the leaf extract on triglycerides obtained in our study is supported by Chaturvedi et al. who demonstrated that administration of methanoic extracts of bitter melon to diabetic rats led to a significant decrease in triglyceride levels 15. The significant increase in HDL cholesterol from D22 onwards in the group treated with M. charantia leaf extract corroborates the findings of Chaturvedi et al. that administration of methanoic extracts of bitter melon to diabetic rats leads to an increase in HDL cholesterol 15. These results on triglycerides, total and HDL cholesterol showed that the leaf extract corrected the lipid disorders linked to diabetes.
Since diabetes was often accompanied by a disturbance of renal function, we evaluated serum creatinine during the experiment. M. charantia leaf extract lowered diabetes-induced hypercreatinine. Such an improvement in renal function in diabetes was also obtained with the green fruit extract of M. charantia 8.
Since diabetes was often accompanied by an inflammatory condition, we also evaluated the effect of the extract on blood leukocytes during the experiment. The reduction in white cells following treatment in groups treated with leaf extract at D17 demonstrated the plant's anti-inflammatory effect, as shown by authors 12. It reduced the number of neutrophils and that of lymphocytes showing its action on both acute and chronic inflammation, as obtained with the extract of the green fruits of the plant 8. Some authors have also demonstrated that oral feeding of M. charantia fruit juice may play a role in 𝛽pancreatic cell renewal in STZ diabetic rats or alternatively may allow recovery from partial 𝛽 cell destruction 16.
Histology revealed in streptozotocin-treated rats (Figure 8B), islets are altered by cell necrosis (asterisks). This effect has already been reported by authors showing that chronic hyperglycemia causes destruction of pancreatic islets, leading to pancreatic dysfunction and the development of type II diabetes 17, 18, 19. However, in rats treated with streptozotocin, followed by insulin (Figure 8C) and M. charantia leaf extract (Figure 8D), islet architecture was significantly restored.
Diabetes is also associated with oxidative stress, which plays an important role in the development of diabetic complications 20. Our results show that leafy stem extract has strong antiglycative activity compared with aminoguanidine. This results in various types of destruction of pancreatic ß-cells 21. Some studies have reported Momordica Charantia antioxidant effects 22, 23 and amelioration of diabetes-induced oxidative stress.
Our results suggest that M. Charantia leaf extract controls pancreatic ß-cell damage without affecting hyperglycemia.
Our study investigated type 1 diabetes in rats and the metabolic activity of M. charantia leaf extract. M. charantia leaf was very rich in secondary metabolites. The most frequent chemical groups in the species studied are alkaloids, triterpenes, steroids, mucilages, flavonoids, reducing compounds and saponosides. The corrective effect on pancreatic necrosis was demonstrated by variations in lipid and renal parameters, and comparatively anti-inflammatory activity in leukocytes. Rats treated with streptozotocin, insulin and M. charantia leaf extract had restored islet architecture. The antiglycative activity of the leaf extract was also demonstrated.
The authors declared no conflicts of interest.
| [1] | WHO. https://www.who.int/fr/news-room/fact-sheets/detail/diabetes. | ||
| In article | |||
| [2] | Diop SN, Djrolo F, Traoré Sidibé A, et al. Consensus pour la prise en charge de l’hyperglycémie dans le diabète de type 2 en Afrique subsaharienne. Rédigé par un groupe d’experts africains du diabète. Médecine des Mal Métaboliques. 2019;13(2):210-216. | ||
| In article | View Article | ||
| [3] | Djrolo F, Houinato D, Gbary A, Akoha R, Djigbénoudé O, Sègnon J. Prévalence du diabète sucré dans la population adulte à Cotonou, Bénin: Prevalence of diabetes mellitus in the adult population at Cotonou, Benin. Médecine des Mal Métaboliques. 2012;6(2):167-169. | ||
| In article | View Article | ||
| [4] | Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. | ||
| In article | View Article PubMed | ||
| [5] | Akesbi M. Dissertation)., La Pratique de La Médecine Alternative et Complémentaires Chez Les Herboristes a La Région de Fès (Doctoral).; 2021. | ||
| In article | |||
| [6] | Liu Z, Gong J, Huang W, Lu F, Dong H. The Effect of Momordica charantia in the Treatment of Diabetes Mellitus: A Review. Evidence-based Complement Altern Med. 2021. | ||
| In article | View Article PubMed | ||
| [7] | Yessoufou A, Gbenou J, Grissa O, et al. Anti-hyperglycemic effects of three medicinal plants in diabetic pregnancy: Modulation of T cell proliferation. BMC Complement Altern Med. 2013;13. | ||
| In article | View Article PubMed | ||
| [8] | Assou C, Anago E, Senou M, et al. Anti-hyperglycemic effect of Momordica charantia green fruit extract. Int J Pharm Sci Invent. 2022;11(5):6-16. | ||
| In article | |||
| [9] | Senou M, Khalifa C, Thimmesch M, et al. A coherent organization of differentiation proteins is required to maintain an appropriate thyroid function in the pendred thyroid. J Clin Endocrinol Metab. 2010;95(8):4021-4030. | ||
| In article | View Article PubMed | ||
| [10] | I. Ahmed, M.S. Lakhani, M. Gillett, A. John HR. Hypotriglyceridemic and hypocholesterolemic effects of anti- diabetic Momordica charantia ( karela ) fruit extract in streptozotocin-induced diabetic rats. Diabetes Res Clin Pract. 2000:155–161. | ||
| In article | View Article PubMed | ||
| [11] | Aljohi A, Matou-Nasri S, Ahmed N. Antiglycation and antioxidant properties of Momordica charantia. PLoS One. 2016;11(8):1-14. | ||
| In article | View Article PubMed | ||
| [12] | Fachinan R, Yessoufou A, Nekoua MP, Moutairou K. Effectiveness of Antihyperglycemic Effect of Momordica charantia: Implication of T-Cell Cytokines. Evidence-based Complement Altern Med. 2017;2017:1-9. | ||
| In article | View Article PubMed | ||
| [13] | Gurav, A., Mondal, D. B., & Vijayakumar H. . In vitro qualitative and quantitative phytochemical analysis of ethanolic and 50% ethanolic extracts of Tinospora cordifolia, Momordica charantia, Cucurbita maxima and Raphanus sativus. In: ; 2014:4-6. | ||
| In article | |||
| [14] | Samba B, Cyrille AN, Niane K, Ndiaye B, Cisse M, Diop CM. Impact of Extraction on Biochemical Properties and Antioxidant Potential of Momordica charantia L . Seeds ’ Oil. 2022:147-164. | ||
| In article | View Article | ||
| [15] | Chaturvedi, P., George, S., Milinganyo, M., & Tripathi YB. Effect of Momordica charantia on lipid profile and oral glucose tolerance in diabetic rats. Phytotherapy Research: An International Journal Devoted to Pharmacological and Toxicological Evaluation of Natural Product Derivatives. 2004:18(11), 954-956. | ||
| In article | View Article PubMed | ||
| [16] | Ahmed I, Adeghate E, Sharma AK, Pallot DJ, Singh J. Effects of Momordica charantia fruit juice on islet morphology in the pancreas of the streptozotocin-diabetic rat. Diabetes Res Clin Pract. 1998;40(3):145-151. | ||
| In article | View Article PubMed | ||
| [17] | Hardt, P. D., Killinger, A., Nalop, J., Schnell-Kretschmer, H., Zekorn, T., & Klör HU. Chronic pancreatitis and diabetes mellitus: a retrospective analysis of 156 ERCP investigations in patients with insulin-dependent and non-insulin-dependent diabetes mellitus. ,. Pancreatology. 2002;2(1), 30-3. | ||
| In article | View Article PubMed | ||
| [18] | Poitout, V., & Robertson RP. Minireview: secondary β-cell failure in type 2 diabetes—a convergence of glucotoxicity and lipotoxicity. Endocrinology. 2002:143(2), 339-342. | ||
| In article | View Article PubMed | ||
| [19] | Nivitabishekam, S. N., Asad, M., & Prasad VS. Pharmacodynamic interaction of Momordica charantia with rosiglitazone in rats. Chem Biol Interact. 2009;177(3), 24. | ||
| In article | View Article PubMed | ||
| [20] | Baynes, J. W., & Thorpe SR. Role of oxidative stress in diabetic complications: a new perspective on an old paradigm. . Diabetes. 1999;48(1), 1-9. | ||
| In article | View Article PubMed | ||
| [21] | Cemek, M., Kağa, S., Şimşek, N., Büyükokuroğlu, M. E., & Konuk M. Antihyperglycemic and antioxidative potential of Matricaria chamomilla L. in streptozotocin-induced diabetic rats. J Nat Med. 2008:62, 284-293. | ||
| In article | View Article PubMed | ||
| [22] | Grover, J. K., & Yadav SP. Pharmacological actions and potential uses of Momordica charantia: a review. J Ethnopharmacol. 2004:93(1), 123-132. | ||
| In article | View Article PubMed | ||
| [23] | Wu, S. J., & Ng LT. Antioxidant and free radical scavenging activities of wild bitter melon (Momordica charantia Linn. var. abbreviata Ser.) in Taiwan. LWT-Food Sci Technol. 2008:41(2), 323-330. | ||
| In article | View Article | ||
Published with license by Science and Education Publishing, Copyright © 2023 Assou Cendra, Anago Eugénie, Agbogba Félicienne, Agniwo Privat, Abissi Yollande, Lokonon Jacques Ezéchiel, Tchogou Pascal, Houngbeme Alban, Baba-Moussa Lamine, Gbénou Joachim and Sènou Maximin
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | WHO. https://www.who.int/fr/news-room/fact-sheets/detail/diabetes. | ||
| In article | |||
| [2] | Diop SN, Djrolo F, Traoré Sidibé A, et al. Consensus pour la prise en charge de l’hyperglycémie dans le diabète de type 2 en Afrique subsaharienne. Rédigé par un groupe d’experts africains du diabète. Médecine des Mal Métaboliques. 2019;13(2):210-216. | ||
| In article | View Article | ||
| [3] | Djrolo F, Houinato D, Gbary A, Akoha R, Djigbénoudé O, Sègnon J. Prévalence du diabète sucré dans la population adulte à Cotonou, Bénin: Prevalence of diabetes mellitus in the adult population at Cotonou, Benin. Médecine des Mal Métaboliques. 2012;6(2):167-169. | ||
| In article | View Article | ||
| [4] | Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. | ||
| In article | View Article PubMed | ||
| [5] | Akesbi M. Dissertation)., La Pratique de La Médecine Alternative et Complémentaires Chez Les Herboristes a La Région de Fès (Doctoral).; 2021. | ||
| In article | |||
| [6] | Liu Z, Gong J, Huang W, Lu F, Dong H. The Effect of Momordica charantia in the Treatment of Diabetes Mellitus: A Review. Evidence-based Complement Altern Med. 2021. | ||
| In article | View Article PubMed | ||
| [7] | Yessoufou A, Gbenou J, Grissa O, et al. Anti-hyperglycemic effects of three medicinal plants in diabetic pregnancy: Modulation of T cell proliferation. BMC Complement Altern Med. 2013;13. | ||
| In article | View Article PubMed | ||
| [8] | Assou C, Anago E, Senou M, et al. Anti-hyperglycemic effect of Momordica charantia green fruit extract. Int J Pharm Sci Invent. 2022;11(5):6-16. | ||
| In article | |||
| [9] | Senou M, Khalifa C, Thimmesch M, et al. A coherent organization of differentiation proteins is required to maintain an appropriate thyroid function in the pendred thyroid. J Clin Endocrinol Metab. 2010;95(8):4021-4030. | ||
| In article | View Article PubMed | ||
| [10] | I. Ahmed, M.S. Lakhani, M. Gillett, A. John HR. Hypotriglyceridemic and hypocholesterolemic effects of anti- diabetic Momordica charantia ( karela ) fruit extract in streptozotocin-induced diabetic rats. Diabetes Res Clin Pract. 2000:155–161. | ||
| In article | View Article PubMed | ||
| [11] | Aljohi A, Matou-Nasri S, Ahmed N. Antiglycation and antioxidant properties of Momordica charantia. PLoS One. 2016;11(8):1-14. | ||
| In article | View Article PubMed | ||
| [12] | Fachinan R, Yessoufou A, Nekoua MP, Moutairou K. Effectiveness of Antihyperglycemic Effect of Momordica charantia: Implication of T-Cell Cytokines. Evidence-based Complement Altern Med. 2017;2017:1-9. | ||
| In article | View Article PubMed | ||
| [13] | Gurav, A., Mondal, D. B., & Vijayakumar H. . In vitro qualitative and quantitative phytochemical analysis of ethanolic and 50% ethanolic extracts of Tinospora cordifolia, Momordica charantia, Cucurbita maxima and Raphanus sativus. In: ; 2014:4-6. | ||
| In article | |||
| [14] | Samba B, Cyrille AN, Niane K, Ndiaye B, Cisse M, Diop CM. Impact of Extraction on Biochemical Properties and Antioxidant Potential of Momordica charantia L . Seeds ’ Oil. 2022:147-164. | ||
| In article | View Article | ||
| [15] | Chaturvedi, P., George, S., Milinganyo, M., & Tripathi YB. Effect of Momordica charantia on lipid profile and oral glucose tolerance in diabetic rats. Phytotherapy Research: An International Journal Devoted to Pharmacological and Toxicological Evaluation of Natural Product Derivatives. 2004:18(11), 954-956. | ||
| In article | View Article PubMed | ||
| [16] | Ahmed I, Adeghate E, Sharma AK, Pallot DJ, Singh J. Effects of Momordica charantia fruit juice on islet morphology in the pancreas of the streptozotocin-diabetic rat. Diabetes Res Clin Pract. 1998;40(3):145-151. | ||
| In article | View Article PubMed | ||
| [17] | Hardt, P. D., Killinger, A., Nalop, J., Schnell-Kretschmer, H., Zekorn, T., & Klör HU. Chronic pancreatitis and diabetes mellitus: a retrospective analysis of 156 ERCP investigations in patients with insulin-dependent and non-insulin-dependent diabetes mellitus. ,. Pancreatology. 2002;2(1), 30-3. | ||
| In article | View Article PubMed | ||
| [18] | Poitout, V., & Robertson RP. Minireview: secondary β-cell failure in type 2 diabetes—a convergence of glucotoxicity and lipotoxicity. Endocrinology. 2002:143(2), 339-342. | ||
| In article | View Article PubMed | ||
| [19] | Nivitabishekam, S. N., Asad, M., & Prasad VS. Pharmacodynamic interaction of Momordica charantia with rosiglitazone in rats. Chem Biol Interact. 2009;177(3), 24. | ||
| In article | View Article PubMed | ||
| [20] | Baynes, J. W., & Thorpe SR. Role of oxidative stress in diabetic complications: a new perspective on an old paradigm. . Diabetes. 1999;48(1), 1-9. | ||
| In article | View Article PubMed | ||
| [21] | Cemek, M., Kağa, S., Şimşek, N., Büyükokuroğlu, M. E., & Konuk M. Antihyperglycemic and antioxidative potential of Matricaria chamomilla L. in streptozotocin-induced diabetic rats. J Nat Med. 2008:62, 284-293. | ||
| In article | View Article PubMed | ||
| [22] | Grover, J. K., & Yadav SP. Pharmacological actions and potential uses of Momordica charantia: a review. J Ethnopharmacol. 2004:93(1), 123-132. | ||
| In article | View Article PubMed | ||
| [23] | Wu, S. J., & Ng LT. Antioxidant and free radical scavenging activities of wild bitter melon (Momordica charantia Linn. var. abbreviata Ser.) in Taiwan. LWT-Food Sci Technol. 2008:41(2), 323-330. | ||
| In article | View Article | ||




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}