 sciepub.com
sciepub.com
 Quick Submission
Quick Submission

Effectiveness of Nutritional Counseling in the Management of Overweight/Obesity in Calabar Metropolis, Cross River State, Nigeria
Iniubong Abasiodiong Thomas1, Margaret Akpana Agiang1, , Julie Omaghomi Jemide1, Kufre John Ekabua2
, Julie Omaghomi Jemide1, Kufre John Ekabua2
1Department of Biochemistry, College of Medical Sciences, University of Calabar, Calabar, Cross River State, Nigeria
2Nutrition Unit, Department of Community Medicine, University of Calabar Teaching Hospital, Calabar, Cross River State, Nigeria
Abstract
A healthy diet is essential for optimal nutritional and health status and the prevention of chronic disease. However, poor diet contributes to the growing epidemics of overweight/obesity and chronic disease both in the developed and developing countries. Furthermore, most individuals lack nutrition knowledge necessary to develop healthier eating patterns. Weight control is considered the best non-medical means of managing overweight/obesity. Improving nutritional knowledge in individuals is also an appropriate strategy. Thus, this study presents the effectiveness of nutritional counseling in the management of overweight/obesity in an urban area in Nigeria. A cross-sectional descriptive clinic-based study was done using a validated interviewer-administered questionnaire to collect information from men and women aged 18-65 years. The effectiveness of nutritional counseling on weight reduction was evaluated; nutrition knowledge, food consumption, behavioural patterns and anthropometry of the overweight/obese individuals were assessed. The findings showed a significant reduction in the body mass index (BMI) within the short duration of intervention indicating a positive correlation between nutritional counseling therapy and nutritional status. Thus, the study postulated nutrition therapy as an important strategy in weight reduction. In addition, the study confirmed an existing evidence of an association between poor dieting and lack of physical exercise as predictors of overweight/obesity. Hence, adequate nutritional counseling and patient involvement in self care plan may be considered positive factors in obesity management.
Keywords: nutritional status, nutritional counseling, overweight/obesity, weight reduction, nutritional knowledge
Copyright © 2017 Science and Education Publishing. All Rights Reserved.Cite this article:
- Iniubong Abasiodiong Thomas, Margaret Akpana Agiang, Julie Omaghomi Jemide, Kufre John Ekabua. Effectiveness of Nutritional Counseling in the Management of Overweight/Obesity in Calabar Metropolis, Cross River State, Nigeria. World Journal of Nutrition and Health. Vol. 5, No. 1, 2017, pp 14-29. http://pubs.sciepub.com/jnh/5/1/3
- Thomas, Iniubong Abasiodiong, et al. "Effectiveness of Nutritional Counseling in the Management of Overweight/Obesity in Calabar Metropolis, Cross River State, Nigeria." World Journal of Nutrition and Health 5.1 (2017): 14-29.
- Thomas, I. A. , Agiang, M. A. , Jemide, J. O. , & Ekabua, K. J. (2017). Effectiveness of Nutritional Counseling in the Management of Overweight/Obesity in Calabar Metropolis, Cross River State, Nigeria. World Journal of Nutrition and Health, 5(1), 14-29.
- Thomas, Iniubong Abasiodiong, Margaret Akpana Agiang, Julie Omaghomi Jemide, and Kufre John Ekabua. "Effectiveness of Nutritional Counseling in the Management of Overweight/Obesity in Calabar Metropolis, Cross River State, Nigeria." World Journal of Nutrition and Health 5, no. 1 (2017): 14-29.
| Import into BibTeX | Import into EndNote | Import into RefMan | Import into RefWorks |
At a glance: Figures
1. Introduction
Nutrition is defined as the science of food and its relationship to health [1]. Adequate food is one of the basic human needs. The types of food eaten in any society should be able to provide the six basic nutrients-carbohydrates, proteins, fats and oils, vitamins, minerals and water necessary for preventing deficiencies, allowing proper growth, maintenance of body weight, and physiological function. Non-nutrients called phytochemicals or phytonutrients are also present in foods which function in maintenance of health. Thus, nutrition plays very significant role in health. Nutritional status, defined as the evidence of nutrition of an individual, can be determined by the quality of nutrients consumed and the body’s ability to utilize the nutrients for its metabolic need [2]. From all indications, consuming the right type of food will promote good nutritional and health status and prevent diseases. Adequate nutrition ensures proper growth, high reproductive level and capability of the immune system from conception to adulthood. If food cannot provide for the needs of the body, poor nutrition will result in nutritional problems and increased risk to infections thus emphasizing a relationship between food, nutrition, and health.
Poor nutrition, in addition to directly causing disease, can have a more subtle influence on our health. It is strongly associated with chronic diseases. The world is currently experiencing a major health transition: a shift in disease epidemic from high rates of infectious diseases to increasing rates of non-communicable diseases (NCDs). With long standing history of infectious diseases, developing countries are now facing a rising tide of non-communicable diseases which is popularly known as the double burden of malnutrition (coexistence of over- and under-nutrition) [3]. The NCDs were previously thought to be “diseases of affluence" affecting only developed world. Good nutrition is thus, critical to preventing not only diseases of deprivation, but also chronic diseases such as cardiovascular diseases (CVDs), diabetes mellitus and cancer. One key modifiable risk factor, however noted for these chronic diseases is obesity. It is a well-established risk factor for heart disease, stroke, type 2 diabetes mellitus, and some forms of cancer.
Obesity is a heterogeneous group of conditions with multiple causes, the outcome of an imbalance between energy intake and energy expenditure [4]. Generally, obesity is defined as excess body fat. But in relation to this definition, there is a hinge. According to Ogden et al. [5], “adiposity is a continuous trait not marked by a clear division into normal and abnormal and it is also difficult to measure body fat directly”. Thus, obesity is often defined as excess body weight rather than as excess fat. Overweight/obesity is seen to be associated with deleterious health conditions such as arteriosclerosis, certain forms of cancer, hypertension, arthritis, diabetes, coronary heart diseases and others [6]. Being overweight is associated with higher rates of death from cardiovascular disease which is primarily to a greater occurrence of high blood pressure, abnormal blood lipids and higher rates of diabetes in overweight individuals [7]. The increasing incidence of overweight/obesity is noted worldwide. Currently, the prevalence rates of overweight, obesity and diet-related chronic diseases such as diabetes and hypertension are increasing in every region and most rapidly in low- and middle-income countries: In sub-Saharan African men, the growth rate of overweight and obesity now exceeds that for underweight; for South Asian women, the prevalence of overweight and obesity is almost the same as the prevalence of underweight; in China, the combined rate of overweight and obese adults is projected to rise to over 50% by 2030 [8]. This is a major concern as no country to date has successfully reversed growth in obesity once it has been allowed to develop [8]. However, even though the prevalence of overweight and obesity in Nigeria continues to increase, literature reviews reveal that recent data is lacking and few studies have been done in this area. According to Ogunjimi et al. [9], in Nigeria, there are no data to back up prevalence of obesity among members of the entire population and this has been attributed to lack of interest by the government towards the welfare of her citizenry.
Obesity is known as a multifactorial disease, meaning that there are many factors that cause it. It has been attributed to rapid urbanization, nutrition transition and reduced physical activity especially in the developing countries. In Nigeria where undernutrition coexist with overnutrition, this emerging burden of disease has been attributed to globalization of western lifestyle: increase in fast food market, inexpensive fast food, increasing fast food culture, coupled with sedentary lifestyle, all leading to increase in overweight and obesity. It is a critical issue as these have brought changes in composition of diets: this dietary transition is basically characterized by a shift from a diet with a higher proportion of carbohydrate based foods such as cereal grains (rice, wheat, maize), vegetables (leaves, roots, legumes) and low animal products (meat, egg, milk) to one which is lower in carbohydrate and higher in animal-based food with high sugar and caloric content and larger amount of processed food (chocolates, soft drinks) [3]. Consequently, this has led to increased rates of nutrition problems. Obesity has also been related positively with dietary factors such as increased snacking [10], and larger portion sizes [11]. Healthy diet therefore, may protect against many chronic diseases, such as cancers, Type 2 diabetes and heart disease, as well as improve general health and wellbeing. Knowledge about dietary needs is also essential for good health and overall nutritional status even when resources are few. Sometimes the importance of variety and balance in diet and the right amount and types of foods needed by the body to meet dietary needs is lacking. Without adequate nutrition knowledge, overweight/obesity can occur even in households with food insecurity.
General management options for overweight/obesity consist of lifestyle modifications in terms of diet and physical activity, surgery and pharmacological methods. While studies have focused on bariatric surgery and anti-obesity medications [12, 13], little is known about the utilization and impact of health behavior education and counseling delivered during routine clinical practice. Research suggests that brief counseling for obesity occurs infrequently, and when it does occur, it is not very effective [14, 15]. According to Lok et al. [16], patient education and counseling skills have been identified as key intervention strategies to tackle obesity; but there has been a lack of reliable evidence for nutrition interventions through counseling as a treatment for obesity [17]. A comprehensive program of lifestyle modification is considered the first option for achieving this goal. Lifestyle modification, also referred to as behavioral weight control, includes three primary components: diet, exercise, and behavior therapy. Hence, studies on the application of this approach to validate, among other things, details for nutrition therapy and adherence rates to such treatment, especially in developing countries like Nigeria, may be necessary. Therefore, this study sought to evaluate the effectiveness of nutritional counseling in the management of overweight/obesity in Calabar Metropolis, Cross River State, Nigeria.
2. Methodology
2.1. Study DesignThe study was a cross-sectional descriptive clinic-based study, carried out in the University of Calabar Teaching Hospital, Calabar Municipality, Cross River State, Nigeria. Calabar Municipality lies between latitude 04° 151 and 5°N and longitude 8° 251E, in the North. It has an area of 331.551sq.km. It has a population of 179,392 at the 2006 census [18]. The people are predominantly farmers, civil servants and traders. The sample population selected for the study was adult male and female patients (18-65 years), resident in the study area and attending the University of Calabar Teaching Hospital, Calabar, Nigeria. The sample size was 100. But 65 participants completed the study. The purposive sampling technique of the non-probability sampling method was used. Ethical clearance was obtained from the Ethics Committee of the University of Calabar Teaching Hospital, Calabar, Nigeria. Informed consent of patients was obtained, requesting their voluntary consent orally.
2.2. Data CollectionInformation was collected from respondents using a content validated interviewer-administered questionnaire. Anthropometric measurement of the subject was assessed by measuring weight and height and converting to body mass index (BMI); dietary pattern was assessed using the 24hr recall. Nutrition counseling involved individual counseling with the subjects by a nutritionist of the University of Calabar Teaching Hospital who was engaged in the study. The counseling in general was targeted at three key areas - diet, physical activity and behaviour. The discussion on dietary intervention consisted of sessions taken with the individual participant every two weeks, which included nutrient requirements/dietary guidelines, eating habits, and the importance of conformity with the diet regimen in order to promote weight loss and improve health. The topics discussed focused on the significance of eating healthy diets (i.e. increasing intake of fruits and vegetables, water, and decreasing consumption of fat, sugar, sodium, and fried foods) in order to guide against the incidence of overweight/obesity. Also, there was administration of test questions to know the subjects’ level of knowledge on nutrition and obesity before and after the counseling. On physical activity, patients were encouraged to increase physical activity, and engage in exercises mainly by walking, or aerobic ball games or other simple exercises. Compliance was recorded. The benefits of exercise in weight-control were explained to the participants. On behaviour modification, they were guided on the need to change their attitude on overeating and under exercising.
2.3. Data AnalysisThe data collected from the research were coded, entered and summarized using statistical package for social science (SPSS version 20.0). Data was analyzed according to the objective of the study using descriptive statistics including frequency, mean, standard deviation and inferential statistics including chi-square, ANOVA. Differences were considered significant at p<0.05.
3. Results
3.1. Socio-demographic CharacteristicsSocio-demographic characteristics of a total of 65 participants are shown in Table 1. Mean age of participants was 43.5±9.95 years and were differentiated as 66.2% male and 33.8% female, the male to female ratio was 2:1. The study was dominated by participants who were married (69.2%) with few participants who were single (24.6%), others were separated (3.1%), divorced (1.5%) or widowed (1.5%). In terms of education, a higher proportion of participants had Bachelor degree and above (60.0%) while lowest proportion were participants who had primary school education (9.2%) as a highest level of education; secondary education and diploma was 18.5% and 12.3% respectively. Majority of participants were civil servants or employed salary earners (60%); self-employed were 24.6%, and percentage of unemployed participants were 4.6%. Monthly income of more than N40, 000 was earned more among 55.0% of participants, while 3.3% earned below N10, 000.








Health characteristics of participants in the study are shown in Table 2. Participants who reported to have coronary heart diseases were 3.1%. Osteoarthritis was reported among 15.4% of participants. Other disease conditions reported among participants were hypertension (25.0%), type II diabetes mellitus (4.6%), waist and joint pain (52.3% and 63.1% respectively). Participants who reported to have undergone any weight loss attempts in the past were 36.9%; 26.2% reported to have tried to lose weight by dieting. More than two third of participants indicated that they were very interested and equally confident in weight loss activities, 10.8% of participants indicated keen interests but had no confidence in weight loss activities; while 7.7% participants were neither interested nor confident in outcome of weight loss activities.





Results of the feeding practices of respondents are presented in Table 3. Special dieting was observed among 15.4% of respondents, as equal percentage of those on special diets were either on a low fat or low salt diet. A greater proportion of the participants took lunch as main meals, while 24.6% had breakfast and lunch as their main meals, only 43.6% ate breakfast as main meals. Those who had all three meals – breakfast, lunch and dinner, were 7.7%. Snacks were observed to be taken mainly in the afternoon (81.1%) and sometimes in the evenings (11.3%). More than two-third of participants often ate out (84.6 %) where foods were prepared away from home or at fast food joints and 83.4% of these respondents ate out 1-5 times in a week, while 4.2% eat outside daily. An average of 7 cups of water was reported to be consumed daily by the participants.




The frequency of consumption of assorted beverages is shown in Table 4. Coffee was never consumed by 43.1% of participants but very often taken by 15.4%. The percentage of adults in the study who seldom consume tea was 40.0% whereas 40.0% drank tea very often. Participants who never consumed beer were 56.9%, 12.3% often consumed and 10.8% very often consumed beer. More than halve of the participants reported never drinking alcoholic wine (58.7%) and those who very often consumed alcoholic wine were 9.5%. Those who said they did not drink non-alcoholic wine were 19.0% while 46.0% seldom drank and 11.1% very often drank non-alcoholic wine. Participants who reported never to drink liquor products were 73.8%, seldom, 15.4% and very often 6.2%. Carbonated soft drinks were never consumed by 23.8% but very often consumed by 47.6%. Non-carbonated soft drink was never consumed by 15.4% of the adults.




The data collected from participants on the frequency of food consumption in the previous week before the commencement of the study is presented in Table 5. The percentage of participants who consumed milk and its products at least once a week were 24.6%; 2-4 times was 20.0% and 5-6 times a week was 4.6% while those who seldom took milk was halve (50.8%). Meat product was consumed 2-4 times by 20.0% of participants and 53.8% by those who ate meat at least 5-6 times a week, and 18.5% seldom ate meat and its products. Fresh fish consumption was by 56.9% of the participants, 5-6 times a week. Similarly, poultry consumption was consumed by 30.5% of participants 5-6 times a week. A higher proportion of respondents consumed root and tubers food 5-6 times a week (69.2%), whereas, 12.3% consumed root and tubers once a week. The proportion of people who consumed legumes, nuts and seeds once a week was 38.5%; another 38.5% seldom ate these food products, while 12.3% ate legumes, nuts and seeds 5-6 times daily. Cereals and grains consumption was shown to be high, 5-6 times a week (83.1%). 32.3% of respondents ate fruits and vegetables 2-4 times a week, followed by those who seldom consumed fruits and vegetables (24.6%), 23.1% consumed fruits about once a week. Fats and oils were frequently taken 5-6 times by 78.5%.




Physical activity pattern of the participants were also studied as seen in Table 6. The respondents were predominantly public servants (46.2%) followed by those involved in trading (20.0%), then those involved in daily household chores (13.8%) and farming (9.2%). Majority of participants spent up to 5-8 hours on their work (46.2%) and 35.4% spent more than 8 hours on their work while others spent 3-4 hours daily at work. Less than half of participants engaged in exercises (43.1%). Sit-ups was the common form of exercise most participants were involved in a typical week (50.0%), while 25% performed brisk walking as a typical weekly exercise. The results also showed that 32.1% of participants spent less than 10 minutes on exercise; another 28.6% spent 10-20 minutes, with 17.9% spending up to 30 minutes and 21.5% spent up to one hour in a typical week. 21% of participants said they were engaged in some form of sporting activities and the common sporting activity reported was running (50.0%). Time spent on sedentary activities like watching television, being on work desk and on computer was also reported. Majority of participants (33.5%) spent 3-4 hours on these sedentary activities, 16.9% spent 5-7 hours and 18.5% spent more than eight hours.




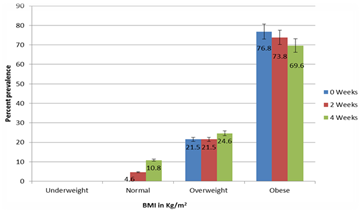
Mean BMI of all participants on pre-nutrition counseling intervention (week zero) was 33.98±4.26, a little higher among females (34.36±4.33) than males (33.24±1.31). After two weeks and four weeks post-interventions, the mean dropped to 32.99±4.41 and 31.58±4.43 respectively for the subjects (Table 7). Figure 1 presents percent prevalence of malnutrition among subjects; the trend shows obesity dropping from 76.8% at 0 week to 73.8% after two weeks and 69.6% at fourth week. Overweight remained unchanged at 21.5% at 0 week and after two weeks, while increasing to 24.6% at the fourth week.




 Download as
Download as
Participants’ knowledge on nutrition was tested before and after nutrition counseling was instituted. It consisted of 10 questions and each was awarded one point: 0-4 points (poor knowledge), 5-6 (average knowledge) and 7-10 (good knowledge). Mean pre-counseling test score was 4.61±1.33 lower for males (4.27±1.31) than females (4.79±1.31). Two weeks post counseling mean score was 6.61±1.39 which increased slightly to 7.01±1.53 at fourth week after nutrition education was repeated for the members. Females consistently showed higher scores in nutrition knowledge (Table 8).




Chi-square association analysis was performed between nutrition related characteristics and nutritional status results obtained on pre-nutritional counseling to test for significant associations as presented in Table 9. Only the variable, eating out, was significantly associated with BMI group; a higher proportion of people who ate outside their homes (81.8%) were more obese than people who did not eat outside (50.0%). The result also showed that people who followed special diets were more obese than those who were not on special diets (90.0% and 76.4% respectively). Among those who followed special diets, those who were on low salt meals were more obese (100%) compared with those who were on low fat meals (80.0%).




Frequency of beverage consumption was also tested against BMI at pre-counseling as presented in Table 10. People who often drank tea were insignificantly more obese (80.0%) compared with those who seldom drank tea (67.9%). A similar trend was observed among those who very often drank coffee (80.0%) compared with those who never drank coffee (67.9%). Also, an insignificant increase of obesity was observed as beer consumption frequency increased. There was no significant difference among people who never drank carbonated soft drinks (86.7%) and those who seldom drank (100%), these two groups were more obese than those who often drank (77.8%) or very often drank (70.0%).




Association between frequencies of the type of meal consumed and BMI of participants is presented in Table 11. Milk and milk products consumption was significantly associated with BMI group, as people who took milk 2-3 times a week (69.2%) or 5-6 times a week were highly obese than those who seldom took milk (18.2%) or once a week (18.8%). People who seldom ate fresh sea foods were statistically less overweight (33.3%) than those who ate fresh sea foods 2-4 times a week (64.3%) and 5-6 times a week (91.9%). Also, the rate of obesity observed among people according to frequency of poultry product consumption varied. There was no significant difference among those who consumed roots and tubers once a week (87.5%), 2-4 times a week (80.0%) and 5-6 times a week (77.8%) compared with those who seldom ate root and tubers (50%), although the results showed high incidence of obesity.
Table 11. Association between frequency of types of food consumed and nutritional status of participants




Association between physical activity and BMI of study subjects is presented in Table 12. A significantly higher rate of obesity was observed among participants who did not exercise (98.4%) compared with their counterparts who engaged in exercises (85.7%). There was however no significant difference among participants who were involved in sports (76.5%) compared with their counterparts who were not involved in sporting activities (85.7%). Among those whose typical daily work were farming, public service and those engaged in household chores, public servants were more obese (90.0%), followed by farmers (66.7%) and those involved in household chores (55.6%). An insignificantly increased rate of obesity was observed relative to increased time spent on work, as it was with sedentary lifestyle.




4. Discussion
Increasing importance is being attached to socio-demographic variables in the assessment and management of disorders including obesity in order to understand the social context in prevention and treatment of such diseases at both the individual and public health levels. As seen in this study, gender, increasing age, high socioeconomic status and marriage increased the likelihood for overweight/obesity. There have been concerns about inequalities in the distribution of overweight and obesity across social groups, particularly by gender, socio-economic status, marital status and ethnic background. The observed high rate of overweight/obesity, particularly among women, is consistent with studies in other developing countries [19, 20]. Study by Gupta et al. [21] revealed that cultural value and positive social attitudes towards fatness among women in Africa are also conducive to feminine obesity. The Calabar people of Cross River State, Nigeria in particular, are known to associate fatness with beauty in women as in the case of the era of fattening rooms. Thus, it is not surprising that some women and even men are still going out of their way to put on weight in order to appear beautiful or prosperous. The men in the area of study are also known to generally prefer overweight women to thin ones. This may have conceivably contributed to the higher rate of over nutrition among females. In line with previously reported studies [22, 23], the present study showed that the prevalence of general obesity was found to increase significantly with age. This could partly be explained by decrease in level of physical activity [24] and decreased metabolism that accompanies aging [33]. The high percentage of married adults in this study was consistent with data from 2013 Nigeria Demographic Health Survey which showed that 69.4% were married [25]. Majority of the participants were employed as civil servants, and more than half of participants earned more than N40 000 monthly which reflect better standard of living. While low socioeconomic status and poor neighborhoods have been associated with a higher prevalence of obesity and chronic diseases in developed countries [26], studies in Africa have demonstrated by contrast a strong positive relationship between obesity and high socioeconomic status [27]. According to Abrha et al. [20], in developing countries context the wealthier are likely to consume energy dense foods and follow a sedentary life style; hence they are more likely to be overweight and obese.
Excess body weight increases the risk of morbidity for numerous conditions especially chronic diseases such as hypertension, type 2 diabetes mellitus among others [6]. This study showed that a high percent of the respondents had related problems as seen in other studies [28, 29]. A study by Ejike et al. [28] revealed that there was a high probability that hypertensive subjects gained weight with time than normotensive subjects, suggesting that even hypertensive patients with normal weight are at increased risk of developing obesity and visceral fat accumulation, associated with increased secretion of free fatty acids, hyperinsulinemia, insulin resistance, hypertension, hyperglycemia and dyslipidemia. Such conditions may have contributed to the high proportion of individuals expressing keen interest and confidence in activities that might assist in reducing weight and a relatively low number have even undergone one form of weight loss program or another. This could be attributed to the fact that adhering to weight loss activities, like exercise and dieting can be difficult as its effect may be slow and time consuming. Ibarra [30] observed that effective and permanent weight loss is a difficult process with a known compliance rate of only 20% after one year. According to a report from a study by Veteran Affairs/Department of Defense, VA/DoD [31], many patients were not ready to make serious attempts to lose weight even though they had been told by their healthcare provider to do so leading to poor outcome in weight management. Many healthcare providers wrongly assumed that patients would comply with instructions.
While genetic factors play an important role in the development of overweight and obesity, environmental factors particularly diet also contribute to this condition. Some eating behaviours among individuals can serve either as risk or protective factors for overweight and obesity [32, 33]. Studies have shown that increased fat intake and dietary salt are associated with body weight gain which can lead to obesity and other related metabolic diseases [34, 35]. In the present study very few subjects were following a special diet like low salt diet and low fat diet. It has been proven that low salt diet has the potential of reducing body fat [33]. This is supported by the notion that intake of dietary salt increases consumption of sugar-sweetened beverages which causes weight gain [33]. According to this author, the mechanism behind this relationship lies in the homeostatic trigger of thirst in response to the ingestion of dietary salt; consumption of dietary salt leads to a rise in plasma sodium concentration, and to maintain body fluid homeostasis, thirst is stimulated, thus promoting fluid intake. Similarly, Samaha et al. [36] reported that consumption of low fat diet was found to reduce the risk of obesity and those severely obese subjects with a high prevalence of diabetes lost more weight in six months on a carbohydrate-restricted diet than on a fat-restricted diet.
In respect to eating pattern such as eating or skipping meals among adults, while some studies have reported association between skipping breakfast as a risk factor to weight gain [37, 38], others have however reported the opposite [39]. Results from this study showed that the rate of eating all three meals (breakfast, lunch and dinner) daily was very low which may not only be a consequence of an individual’s behaviour but as a result of food insecurity especially in low resource settings [40]. The results, however, showed high consumption of snacks in the afternoon which may have an implication in making individuals skip eating a good meal for lunch. In addition, consumption of sweetened snacks has been shown to contribute to weight gain [41]. It was not surprising to record, in this study, very high percentage of respondents who had the habit of eating out in the ever increasing number of restaurants and fast-foods in urban centers in Nigeria in recent years. Results from the assessment of beverages and food consumption in this study showed high frequency of coffee and tea consumption. Several studies have been published on the frequencies of consumption of soft-drinks and alcohol and their effects on health particularly on changes in body weight gain. Okoro [42] reported a rapid increase in the consumption of coffee due to amplified demand for the drink amongst corporate Nigerians in the private and public sectors that are regularly confronted with the rigors of their busy schedule and have the need to stay alert in challenging work environment. Coffee and tea are stimulants which contain caffeine, its consumption in high doses have been reported to have negative effect on indigestion, insomnia and nervousness [43]. Some researchers have however indicated a relation between coffee and tea consumption with reduction in weight loss among adults [44], others have shown that consumption of coffee and/or tea with artificial sweeteners was associated with obesity [45]. Results showed that alcohol consumption from beer, alcoholic wine and liquor was not at an alarming frequency in this study which is encouraging. It is seen that frequent drinkers of alcohol are prone to addiction and are unaware of high intake of calorie from alcoholic drinks. Bates et al. [46] reported that alcohol accounts for nearly 10% of the calorie intake amongst adults who drink, and an energy value of 7kcal/g, second only to fat which is the most energy dense macronutrient at 9kcal/g. The same trend was shown for consumption of carbonated and non-alcoholic drinks. Regular intake of soft drinks has been reported to have negative consequences on diet and health; that soft drinks can increase body weight if the overall energy intake due to their consumption is not compensated for by reducing the intake of other foods, thus resulting in increased total energy intake regular diet [47]. The increased amount of sweetener in regular soft drinks increases caloric intake and is a contributory factor in the development of obesity.
Dieting is one of the most important approaches to maintaining a healthy outlook. Foods when consumed in an unwholesome manner can contribute to intake of excessive calories which can lead to weight gain. Fruits and vegetables which are good sources of vitamins were less consumed compared with carbohydrate foods and fats which was most consumed especially as they constitute the majority of prepared food items consumed in most households in Nigeria. Carbohydrate-rich diets like fats are rich-energy diets, and consumption of high-energy diets has been implicated in weight gain and obesity [48]. Amole et al. [49] reported that consumption of high-energy diets is one of the major contributing factors to the development of obesity.
The type of work an individual engages in can have an adverse effect in weight changes. There is a great body of literature which shows that people who have sedentary lifestyle or who take jobs that require them being sedentary at all times may most likely gain weight over time [50, 51][50, 51]. The predominant typical daily work in the present study was working as public servants, who sometimes worked for very long hours in the day. Ogunjimi et al. [9] studied the prevalence of obesity among nurses working in public health institutions, and attributed the increased sluggish attitude in carrying out their duties to excessive consumption of high calorie foods and lack of exercise. There have been studies that have shown the importance of exercise to weight reduction and reduced risk of cardiovascular diseases [52]. The authors have decried lack of exercise and sporting activities among many people as a major contributor to weight gain. Increased TV viewing time among people as seen in the present study is associated with a likelihood of overweight. More studies have also supported the reports that overweight/obesity could result from a combination of unhealthy dietary habits [53], sedentary behaviour and exposure to TV advertising [54, 55].
Although, as stated by Ogunjimi et al. [9], there are no data to back up prevalence of obesity in Nigeria, some studies have shown that the rate is alarming with figures ranging from 8.1-22.2% and overweight ranging from 20.3-35.1% [56]. Wahab et al. [57] has reported even higher rate of overweight among apparently healthy adults in Nigeria with rate up to 53%. Although the present study only included participants whose BMI were ≥ 25 kg/m2, the prevalence of obesity (BMI ≥30.0 kg/m2) was however observed to be substantially higher than overweight with BMI 25.0-29.9 kg/m2 before the commencement of the study; obesity rate remained higher two weeks after the first intervention and at fourth week, after second intervention was carried out. Test-of-difference result in this study indicated significant difference in mean BMI between mean at zero week and fourth week with a modest reduction of up to 2.4 kg/m2, which was encouraging considering the short duration of this intervention study. Blackburn [58] and Srinivas et al. [59] have reported that even modest weight reduction in the range of 5–10% of the initial body weight of an individual is associated with significant improvements in a wide range of co-morbid conditions.
Nutrition counseling therapy constitutes advice on healthy diets, behaviour modification, with a combination of weight loss programme. This can help people who are overweight or obese to cut down on excessive body fat, and prevent health-related conditions associated with overweight. As seen in a similar study, Melin et al. [60] showed in a nutrition intervention study which not only comprised dietary counseling but behaviour modification, very-low-calorie diet and a continuous measuring of metabolic and anthropometrical status, that high attendance in the programme, consequently adherence to programme therapy, was positively associated with weight reduction.
5. Conclusion
From the results of this study, it could be concluded that there is high prevalence of obesity in Calabar Metropolis, Nigeria, and there is an imperative need for intensive public health education. The significant reduction in the BMI within the short duration of intervention indicates a positive correlation between nutrition counseling therapy and nutritional status, thus the study postulates nutrition therapy as an important strategy in weight reduction. In addition, the study confirmed an existing evidence of an association between poor dieting and lack of physical exercise as predictors of overweight and obesity. Healthy living in terms of consumption of fruits and vegetables, regular aerobic exercises and discouragement of consumption of calorie-dense diets are some of the issues that should be addressed in educating the populace on this avoidable epidemic. If consideration is given to the fact that the battle against infectious diseases like malaria and HIV/AIDS is still far from being won, all efforts should, therefore, be made to stem the tide of the rising prevalence of overweight and obesity so that the burden of other related non-communicable cardiovascular disorders can be reduced.
Adequate nutritional counseling and patient involvement in self care plan are shown to be positive factors in obesity management. The prolonged hospitalization and waste of funds experienced by patients due to obesity related conditions can be alleviated by simple practical nutrition education, and healthy food choice. Thus, the use of nutrition education as a tool in obesity management has proven to be a cheaper and cost effective tool. As seen in the study, attitude to the choice of food and practice was shown to have impact on the development of obesity. More research should be focused on local foods that can be used in the reverse of degenerative conditions associated with obesity. Attention should be directed towards practical demonstration in nutrition education of obese patients.
References
| [1] | Park, K. Park’s textbook of preventive and social medicine, 19th Ed, Banarsidas Bahot Publishers, Japalpur (India), 2007. | ||
 In article In article | |||
| [2] | Amosu, A. M., Degun, A. M., Atuolomah, N. O. and Olarenwaju, M. F. A study of the nutritional status of under five children of low-income earners in South-Western Nigerian community. Current Research Journal of Biological Sciences, 3(6):578-585. | ||
| In article | |||
| [3] | Bishwajit, G. Nutrition transition in South Asia: the emergence of non-communicable chronic diseases. F1000 research, 4:8, Nov, 2015. | ||
| In article | |||
| [4] | National Task Force on the Prevention and Treatment of Obesity. Overweight, Obesity, and Health Risk. Archives of Internal Medicine, 160(7):898-904, 2000. | ||
| In article | View Article PubMed | ||
| [5] | Ogden, C.L., Carroll, M.D., Curtin, L.R., McDowell, M.A., Tabak, C.J. and Flegal, K.M. Prevalence of overweight and obesity in the United States, 1999-2004. Journal of American Medical Association, 295(13):1549-55, 2006. | ||
| In article | View Article PubMed | ||
| [6] | Kozak, A.T., Daviglus, M.L., Chan, C., Kiefe, C.I., Jacobs, D.R. and Liu, K. Relationship of body mass index in young adulthood and health-related quality of life two decades later: the coronary artery risk development in young adults study. International Journal of Obesity, 35:134-141, 2011. | ||
| In article | View Article PubMed | ||
| [7] | Pesek, K., Pesesk, T. and Roginic, S. The importance of risk factors analysis in the prevention of cardiovascular disease (CVD), 2015, Available at www.intechopen.com [Accessed on 3rd February, 2017]. | ||
| In article | |||
| [8] | Global Panel on Agriculture and Food Systems for Nutrition. Food systems and diets: facing the challenges of the 21st century, 2016, Available at www.gpafsn.org [Accessed on 12th January, 2017]. | ||
| In article | |||
| [9] | Ogunjimi, L.O., Ikorok, M.M. and Yusuf, O.O. Prevalence of obesity among Nigeria nurses: the Akwa Ibom State experience, International Non Governmental Organization Journal, 5(2): 045-049, 2010. | ||
| In article | |||
| [10] | Duffey K.J. and Popkin B.M. Energy density, portion size, and eating occasions: contributions to increased energy intake in the United States, 1977-2006. PLoS Medicine, 8. June, 2011. | ||
| In article | View Article | ||
| [11] | Piernas C. and Popkin B.M. Food portion patterns and trends among U.S. children and the relationship to total eating occasion size, 1977-2006. Journal of Nutrition, 141: 1159-1164, 2011. | ||
| In article | View Article PubMed | ||
| [12] | Padwal, R.S., Gabr, R.Q. and Sharma, A.M, Effect of gastric bypass surgery on the absorption and bioavailability of metfotmin. Diabetes Care, 34:1295-1300, 2011. | ||
| In article | View Article PubMed | ||
| [13] | Geraldo, M.P., Fonseca, F.A., Goveia, M.V. and Feder, D. The use of drugs in patients who have undergone bariatric surgery. International Journal of General Medicine, 7: 219-224, 2014. | ||
| In article | View Article PubMed | ||
| [14] | McAlpine, D.D. and Wilson, A.R. Trends in obesity-related counseling in primary care: 1995-2004. Medical Care, 45: 322-329. 2007. | ||
| In article | View Article PubMed | ||
| [15] | Ma, J., Xiao, L. and Stafford, R.S. Under-diagnosis of obesity in adults in US outpatient settings. Archives of Internal Medicine, 169:313-314, 2011. | ||
| In article | |||
| [16] | Lok, K.H., Fiehn, O., Garvey, W.T., Newman, J.W., Hoppel, C.L. and Adams, S.H. Plasma metabolomic profiles reflective of glucose homeostasis in non-diabetic and type 2 diabetic obese African-American women. PLoS One, 5(12): e15234, 2010. | ||
| In article | View Article PubMed | ||
| [17] | Aetna, Nutritional counseling, 2013, Available: www.aetna.org [Accessed: 10th August, 2014]. | ||
| In article | |||
| [18] | National Population Commission (NPC). Provisional census figure of the 2006 national census for Cross River State, Nigeria, 2006 Available at http//www.population.gov.ng [Accessed 12th January, 2017]. | ||
| In article | |||
| [19] | Ng, M., Fleming, T. & Robinson, M., Thomson, B., Graetz, N., Margono, C. et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet, 384(9945):766-781, 2014. | ||
| In article | View Article | ||
| [20] | Abrha, S., Shifera, S. and Ahmed, K. Overweight and obesity and its socio-demographic correlates among urban Ethiopian women: evidence from the 2011 EDHS. BMC Public Health, 16:636, 2016. | ||
| In article | View Article PubMed | ||
| [21] | Gupta, N., Goel, N., Shah, P. and Misra, A. Childhood obesity in developing countries: epidemiology, determinants, and prevention. Endocrinology Reviews, 33:48-70, 2012. | ||
| In article | View Article PubMed | ||
| [22] | Neuman, M., Finlay, J.E., Davey, S.G and Subramanian, S.V. The poor stay thinner: stable socioeconomic gradients in BMI among women in lower- and middle-income countries. American Journal of Clinical Nutrition, 94(5):1348-57, 2011. | ||
| In article | View Article PubMed | ||
| [23] | Henok A, A., Ephem, M. G. and Solomon, S. Effect of shift-work on hypertension among factory workers in Ethiopia. American Journal of Clinical and Experimental Medicine, 3(4):142-148, 2015. | ||
| In article | View Article | ||
| [24] | Alemu, E., Atnafu, A., Yitayal, M. and Yimam, K. Prevalence of overweight and/or obesity and associated factors among high school adolescents in Arada Sub city, Addis Ababa, Ethiopia. Journal of Nutritional Food Science, 4:261, 2014. | ||
| In article | View Article | ||
| [25] | National Population Commission (NPC) (Nigeria) and ICF International. Nigeria Demographic and Health Survey 2013, Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International, 2014. | ||
| In article | |||
| [26] | Lopez, R.P. Neighborhood risk factors for obesity. Obesity (Silver Spring), 15(8):2111-2119, 2007. | ||
| In article | View Article PubMed | ||
| [27] | Christensen, D.L., Eis, J., Hansen, A.W., Larsson, M.W., Mwaniki, D.L. et al. Obesity and regional fat distribution in Kenyan populations: impact of ethnicity and urbanization. Annals of Human Biology, 35 (2): 232-249, 2008. | ||
| In article | View Article PubMed | ||
| [28] | Ejike, C., Chukwunonso, E.C., Ugwu, C., Chidiebere, E. and Ezeanyika, L.U. Nutritional status, prevalence of some metabolic risk factors for cardiovascular disease and BMI-metabolic-risk sub-phenotypes in an adult Nigerian population. Health Psychology, 21(1):17-24, 2009. | ||
| In article | |||
| [29] | Ziraba, A.K., Fotso, J.C. and Ochako, R. Overweight and obesity in urban Africa: a problem of the rich or the poor? BMC Public Health, 9(1):465, 2009. | ||
| In article | View Article PubMed | ||
| [30] | Ibarra, J. Obesity and cardiovascular disease. The Journal of Lancaster General Hospital, 4(4):130-133, 2009. | ||
| In article | |||
| [31] | Veteran Affairs/Department of Defense (VA/DoD), Clinical practice guideline for screening and management of overweight and obesity, 2014. Available at www.healthquality.va.gov [Accessed on 1st December, 2016]. | ||
| In article | |||
| [32] | Arora, R., James, S. and Fredericks, R. Association of breakfast intake with obesity, dietary and physical activity behavior among urban school-aged adolescents in Delhi, India: results of a cross-sectional study. British Medical Council of Public Health, 12:881, 2012. | ||
| In article | View Article | ||
| [33] | Grimes, C. A., Riddell, L. J. Campbell, K.J. and Nowson, C. A. Dietary salt intake, sugar-sweetened beverage consumption, and obesity risk. Pediatrics, 131(1):14-21, 2013. | ||
| In article | View Article PubMed | ||
| [34] | Hooper, L., Abdelhamid, A., Bunn, D., Brown, T., Summerell, C.D. and Skeaf, C.M. Effects of total fat intake on body weight. Cochrane Database System Reviews, 7(8):CD011834, 2015. | ||
| In article | View Article | ||
| [35] | Ma, Y., He, F.J. & MacGregor, G.A. (2015). High Salt Intake: independent risk factor for obesity? Hypertension, 66(4):843-849, 2015. | ||
| In article | View Article PubMed | ||
| [36] | Samaha, F., Frederick, F., Nayyar, I., Prakash, S., Kathryn, L. et al. Low-carbohydrate as compared with a low-fat diet in severe obesity. New England Journal of Medicine, 348:2074-81, 2003 | ||
| In article | View Article PubMed | ||
| [37] | Mesas, A.E., Munoz-Pareja, M., Lopez-Garcia, E. and Rodriguez-Artalejo, F. Selected eating behaviours and excess body weight: A systematic review. Obesity Review, 28(10), 2011. | ||
| In article | |||
| [38] | Watanabe, Y., Saito, I., Henmi, I., Yoshimura, K., Marvyama, K., et al. Skipping breakfast is correlated with obesity. Journal of Rural Medicine, 9(2):51-58, 2014. | ||
| In article | View Article PubMed | ||
| [39] | Rampersaud, G.C., Pereira, M.A., Girard, B.L., Adams, J. and Metzl, J.D. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. Journal of the American Dietetic Association, 105(5):743-60, 2005 | ||
| In article | View Article PubMed | ||
| [40] | Pearson, N., Biddle, S.J. and Gorely, T. Family correlates of breakfast consumption among children and adolescents: a systematic review. Appetite, 52(1):1-7, 2005. | ||
| In article | View Article PubMed | ||
| [41] | Fielding‐Singh, P., Almy, J.D., Margo, M.S. and Wootan, G. Sugar overload: Retail checkout promotes obesity. Center for Science in the Public Interest (CSPI), USA, 2014. | ||
| In article | |||
| [42] | Okoro, G. Is moderate coffee consumption benevolent? 2014. Available at http://www.dairlyindependentnig.com [Accessed on 15th December, 2016]. | ||
| In article | |||
| [43] | Wammanda, R. D. Hyperactivity and inattention: a successful response to table coffee. Nigerian Journal of Clinical Practice, 10 (2):182-183, 2007. | ||
| In article | PubMed | ||
| [44] | Vernarelli, J.A. and Lambert, J.D. Tea consumption is inversely associated with weight status and other markers for metabolic syndrome in U.S. adults. European Journal of Nutrition, 52(3):1039-1048, 2013. | ||
| In article | View Article PubMed | ||
| [45] | Bouchard, D.R., Ross, R. and Janssen, I. Coffee, tea and their additives: association with BMI and waist circumference. Obesity Facts, 3(6): 345-352, 2010. | ||
| In article | View Article PubMed | ||
| [46] | Bates, B, Alison, A. and Lennox, A.G. (2009). National diet and nutrition survey: headline results from year one of the rolling programme (2008/2009), London: Food Standards Agency. | ||
| In article | |||
| [47] | Vartanian, L. R., Schwartz, M. B., Brownell, K. D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. American journal of public health, 97(4): 667-675, 2007. | ||
| In article | View Article PubMed | ||
| [48] | National Center for Health Statistics (NCHS)/Centers for Disease Control and Prevention, United State, Hyattsville, MD 2007. Available at http://www.cdc.gov/nchs [Accessed 12th June 2016]. | ||
| In article | |||
| [49] | Amole, I.O., OlaOlorun, A.D., Odeigah, L.O. & Adesina, S.A. The prevalence of abdominal obesity and hypertension amongst adults in Ogbomoso, Nigeria. African Journal of Primary Health Care & Family Medicine, 3(1): 1-6, 2011. | ||
| In article | View Article PubMed | ||
| [50] | Adegun, J.A. Nutrition and body weight control among public servants in Ekiti State, Nigeria. Health and Fitness Journal International, 4 (142): 51-57, 2003. | ||
| In article | |||
| [51] | Sodjinou, R., Agueh, V. and Fayomi, B. Obesity and cardio-metabolic risk factors in urban adults of Benin: relationship with socio-economic status, urbanization, and lifestyle patterns. BMC Public Health, 8:84, 2008. | ||
| In article | View Article PubMed | ||
| [52] | Oyerinde, O.O. and Owojaiye, S.O, Diet, exercise and obesity: health consequences civil-servants in Nigeria. Fourth International Council for Health and Physical Education, Recreation, Sport and Dance (ICHPERSD). Africa Regional Congress, 4:14-17, 2008. | ||
| In article | |||
| [53] | Dubois L., Farmer, A., Girard, M. and Peterson, K. Social factors and television use during meals and snacks is associated with higher BMI among pre-school children. Public Health Nutrition, 11(12):1267-79, 2008. | ||
| In article | View Article PubMed | ||
| [54] | Anschutz, D.J., Engels, R.C. and Van Strien, T. Side effects of television food commercials on concurrent non-advertised sweet snack food intakes in young children. The American Journal of Clinical Nutrition, 89(5):1328-1333, 2009. | ||
| In article | View Article PubMed | ||
| [55] | Boyland, E.J., Harrold, J.A., Kirkham, T.C., Corker, C., Cuddy, J. & Evans, D. Food commercials increase preference for energy-dense foods, particularly in children who watch more television. Pediatrics, 128(1):93-100, 2011. | ||
| In article | View Article PubMed | ||
| [56] | Chukwuonye, I., Chuku, A., John, C., Ohagwu, K.., Imoh, M.E., Isa, S.I., Ogah, O.S. and Oviasu, E. Prevalence of overweight and obesity in adult Nigerians – a systematic review. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 6:43-47, 2013. | ||
| In article | View Article PubMed | ||
| [57] | Wahab, K.W., Mahmoud, U.S., Bashir, O., Yusuf, M. G., Gbadamosi, A. and Mahmoud, I.Y. Prevalence and determinants of obesity - a cross-sectional study of an adult Northern Nigerian population. International Archives of Medicine, 4:10, 2010. | ||
| In article | View Article PubMed | ||
| [58] | Blackburn, G.L. Effect of degree of weight loss on health benefits. Obesity Research, 3:211s-216s, 1995. | ||
| In article | View Article PubMed | ||
| [59] | Srinivas, N., Srinivas, S.K., Krishna, M.C. and Krishna, M.B. Obesity: an overview on its current perspectives and treatment options. Nutrition Journal, 3:3-9, 2004. | ||
| In article | View Article PubMed | ||
| [60] | Melin, I., Karlstro, M,B., Lappalainen, R., Berglund, L., Mohsen, R. and Vessby, B. A programme of behaviour modification and nutrition counseling in the treatment of obesity: a randomised two year clinical trial. International Journal of Obesity, 27, 1127-1135, 2003. | ||
| In article | View Article PubMed | ||
 CiteULike
CiteULike Delicious
Delicious



{kind=link}
{kind=link}