This study evaluated the efficacy of UBPN01 (Salvia miltiorrhiza extract) for alleviating menopausal syndrome. This study was a randomized, double-blind, placebo-controlled clinical trial involving female subjects (40 – 60 years) with menopausal syndrome. Subjects were administered 600 mg/day UBPN01 or placebo, and efficacy endpoints were menopausal symptoms according to the total Kupperman Index (KI) score and individual categories. After 12 weeks, the total KI scores decreased and depression and vaginal dryness symptoms improved, especially in UBPN01 compared to placebo. Moreover, we observed no significant difference between the two groups in estradiol, follicle stimulating hormone, or luteinizing hormone. These results demonstrated that UBPN01 alleviates menopausal symptoms without notable side effects and improves quality of life, suggesting its efficacy as an alternative supplement for women ineligible for hormone therapy.
Menopause, including peri-menopause and post-menopause, is the time of life when female hormones change and menstrual cycles cease 1. It is characterized by a decrease in estrogen level in particular 2. This sharp decline in estrogen induces psychological, emotional, and physical symptoms such as fatigue, excitement, insomnia, vaginal dryness, anxiety, nervousness, recurrent facial hot flashes, dizziness, vertigo, lethargy, numbness, diarrhea, joint pain, and muscle pain 3, 4, 5, 6. In addition, the risk of osteoporosis and other chronic diseases is greater during this time, as is increased mortality from cardiovascular diseases such as heart disease, high blood pressure, and stroke.
Evaluating and quantifying menopausal syndrome in a standardized manner is critical for diagnosis and treatment. The two most commonly used tools are the Kupperman Index (KI) and the menopause rating scale (MRS) 10, 11. Both of these instruments are widely accepted, self-administered questionnaires designed to measure menopausal syndromes and show strong correlation with each other 12.
Salvia miltiorrhiza Bunge is a perennial plant belonging to the family Labiatae and is a traditional Chinese herb with more than 1,000 years of clinical experiments 13. S. miltiorrhiza Bunge root is an herbal medicine used to treat various diseases including coronary artery disease, arthritis, osteoporosis, cerebrovascular disease, diabetes, heart disease, hepatitis, and cancer 14, 15, 16, 17. In addition, S. miltiorrhiza exhibits estrogen-like activity and induces proliferation of MCF-7 cells 18. Previous studies have reported that S. miltiorrhiza extract improves osteoporosis through recovery of spongy bone loss caused by natural aging in an estrogen-deficient animal model 19. Also, S. miltiorrhiza extract tends to stimulate bone formation, and calcium should be added concurrently to improve osteoporosis as shown in a calcium-deficient animal model 20.
In Chinese medicine, danshen-honghua (DSHH) is effective to treat cognitive impairment caused by hippocampal damage from ischemia 21. Clinical therapeutic effects on menopausal depression by DSHH have also been reported 22. There are no studies on the relief of menopausal symptoms with S. miltiorrhiza extract alone, but relief of menopausal symptoms using a prescription containing S. miltiorrhiza in combination with other ingredients has been reported.
The purpose of this study was to investigate whether S. miltiorrhiza extract improves menopause symptoms in women. The results of this study provide valuable information for further pharmacological studies and clinical trials.
This clinical trial (21PR0022-008) was reviewed and approved by Syncorp Health Pvt. Ltd (India). This clinical study was conducted according to a protocol in compliance with Good Clinical Practice (GCP E6(R2)), with the Declaration of Helsinki (Version 1989), and with other applicable regulatory requirements. Prior to screening, all subjects provided written informed consent to participate after having been informed about the nature and purpose of the study and participation/withdrawal conditions.
2.1. Clinical Study MaterialUBPN01 is a capsule containing a 70% ethanol extract of S. miltiorrhiza Bunge. One capsule of UBPN01 (1,000 mg) contains 300 mg of the S. miltiorrhiza extract and 700 mg of soybean lecithin (30 mg), beeswax (50 mg), and soybean oil (620 mg). Placebo capsules were identical to the UBPN01 capsules (a chocolate brown, soft, rectangular capsule) in size, texture, and color. The manufacturing process was in accordance with good manufacturing process (GMP) standards, and the drugs were delivered and stored according to the manufacturer’s instructions.
2.2. ParticipantsThis study included women aged 40 to 60 (both inclusive) years with menopause (amenorrhea for 12 consecutive months), transition to menopause (FSH > 30 IU/L without menstruation for more than 3 months), or severe menopausal symptoms (modified Kupperman Index total score ≥ 25 points). The exclusion criteria comprised treatment with medications that could influence hormones such as phytoestrogen containing foods (kudzu root, soybean extract, red clover extract (tripatra), fenugreek, wild yam, pomegranate); vitamins (vitamin E, vitamin B6); herbal extracts (black cohosh (rattleroot), flaxseed, St. John’s wort, Angelica sinensis (dong quai), products containing Salvia officinalis (common sage), cinnamon, moringa, peony root, or ginseng products); gamma linoleic acid; therapeutic agents for osteoporosis such as a bisphosphonate preparation; body mass index (BMI) > 30 kg/m2; hypertension (160 /100 mmHg or more, after 10 minutes of stabilization); fasting blood sugar (>180 mg/dl); TSH ≤ 0.1 μU/ml or > 10 μU/ml; 3.0-fold elevated alanine transaminase (ALT) and aspartate transaminase (AST) compared with normal values; 2.0-fold elevated creatinine compared with normal values; endometrial thickness > 5 mm; thyroid hormone preparations; clonidine, anticoagulants, or antithrombotic agents within 3 months; endometrial hyperplasia, uterine cancer, endometrial cancer, breast cancer, or breast disease; and sex hormone-related cancer, thrombo-embolism, cerebrovascular disease, myocardial infarction, unstable angina, coronary angioplasty, depression, anxiety disorder, or pregnancy.
2.3. ProtocolThe clinical trial consisted of a multi-center, randomized, double-blind, placebo-controlled, parallel study. After inclusion in the study, subjects were randomly administered 1,000mg of UBPN01 capsules twice a day or placebo capsules twice a day for 12 weeks.
The parameters of modified KI total/individual item scores, menopause rating scale (MRS), vaginal maturation index (VMI), and vaginal pH were used to assess the efficacy of UBPN01. The safety of UBPN01 was evaluated by hematological, blood biochemical, urinalysis, vital signs, estradiol (E2), follicle stimulating hormone (FSH), luteinizing hormone (LH), endometrial thickness parameters, and occurrence of adverse events (AE) or serious adverse events (SAE) during the study period.
As an additional analysis, the isoflavone intake of each subject during the study period was calculated and compared between the two groups, as isoflavone can favorably affect postmenopausal symptoms. Analysis was performed to determine whether intake of isoflavone affected the efficacy of UBPN01.
2.4. Primary Outcome MeasurementA total of 100 subjects was recruited to demonstrate that the change in the total/individual item score of Modified KI in the 12-week experimental group after ingestion of UBPN01 was superior to that of the control group. To evaluate whether the difference between the experimental and control groups was significant, an independent t-test analysis was used. Based on a two-sided test in this calculation, the model has a power of 80% and a significance level of 5%.
H0: There is no difference between the experimental and control groups in the Modified KI total/individual item score change relative to the baseline value.
H1: There is a significant difference between the experimental and control groups in the Modified KI total/individual item score change relative to the baseline value.
To estimate the number of valid subjects in this study, the following are assumed.
1. Superiority test
2. 5% Level of significance, two-sided
3. Type II error (β) 0.2, Power of the test 80%
4. Ratio between the experimental group and the control group 1:1
5. A previous study reported that changes in total KI score were significantly different between the experimental group and the control group. Therefore, the sample size was calculated considering the difference of the evaluation variables and the standard deviation in the previous study. Based on a previous study, we assume that the difference between experimental and control groups is 11.0 units, and standard deviation is 15.7 units.
 |
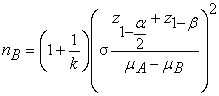 |
z1-α/2: z score for 1-α/2
z(1-β): z score for 1-β
α: probability of type I error
β: probability of type II error
σ: standard deviation
k: nA/nB
μA: mean of experimental group
μB: mean of control group
When the number of test subjects was calculated as follows, the result was about 32 per group.
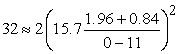 |
To reinforce the statistical power, a weight of 25% was applied to the number of subjects calculated for each group, resulting in 40 subjects per group (total: 80). Considering a dropout rate of 20%, the number of subjects enrolled in the clinical trial was 50 per group (total: 100).
2.5. Safety EvaluationThe safety analysis set included all randomized subjects who received at least one dose of UBPN01 or placebo, with treatment assignment according to actual treatment received. The safety variables were compared within and between the treatment groups (UBPN01 or placebo) at baseline and after 12 weeks from the baseline. The variables were summarized with number of non-missing observations (N), mean, standard deviation, median, minimum, and maximum. The change at EOT was calculated by subtracting the baseline value from EOT value. Therefore, a positive change indicates increase in value from baseline and a negative sign indicates decrease in values.
2.6. Statistical AnalysisAn independent, two-sample, two-tailed t-test was used to compare the changes be-tween baseline and week 12. A p-value ≤ 0.05 was considered statistically significant. Analyses were performed using a per-protocol set (PPS).
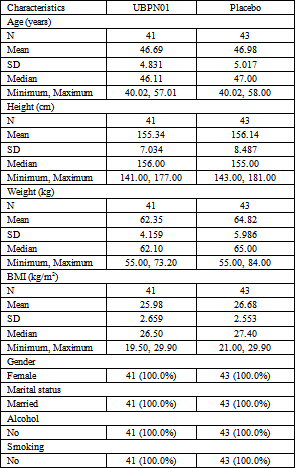
The demographic and baseline characteristics of all the subjects randomized into the study were summarized for PP analysis sets, with N (number of non-missing observations, mean (standard deviation), median, and range (minimum, maximum) (Table 1). The 41 subjects in UBPN01 and 43 subjects in placebo were included in the analysis of PPS. The mean age of the subjects in the UBPN01 group was 46.7 years (46.7 ± 4.83) with mean height 155.3 cm (155.3 ± 7.03), weight 62.4 kg (62.4 ± 4.16), and BMI 26 kg/m2 (26.0 ± 2.66). The subjects were non-alcoholic and non-smokers. The mean age of the subjects in the placebo group was 47 years (47.0 ± 5.02) with mean height 156.1 cm (156.1 ± 8.49), weight 64.8 kg (64.8 ± 5.99), and BMI 26.7 kg/m2 (26.7 ± 2.55). The subjects were non-alcoholic and non-smokers.
The Kupperman Index (KI) is widely used internationally, and its role in clinical practice is well established 10.
For the UBPN01 and placebo groups, there was a statistically significant difference in modified KI total score according to visit point. The rate of change in the modified KI total score at the last visit compared to baseline decreased to 19.71% in the UBPN01 group and 8.35% in the placebo group. The modified KI consists of 12 items of symptoms/comfort. Depending on the degree of symptoms, the scores were recorded as non (0), mild (1), moderate (2), or severe (3), and individual item stores were calculated by multiplyging each factor by importance.
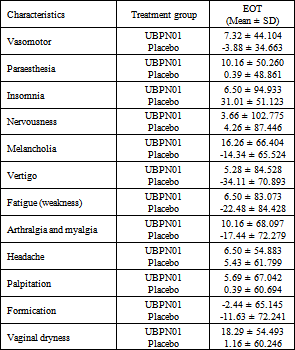
When the rate of change at the last point compared to the baseline was investigated, vasomotor symptoms decreased by 7.32% in the UBPN01 group, but increased by 3.88% in the placebo group. At the last point compared to baseline, paraesthesia decreased by 10.16% in the UBPN01 group and to 0.39% in the placebo group. There was no statistically significant inter-group difference as p-value was 0.05 or higher at all visit times, but the p-value was less than 0.05 at 12 weeks compared to baseline of the UBPN01 group, confirming a significant inter-group difference. Insomnia symptoms decreased by 6.50% in the UBPN01 group and 31.01% in the placebo group, and statistically significant differences between groups were confirmed. Nervousness symptoms were reduced by 3.66% in the UBPN01 group and 4.26% in the placebo group, and statistically significant intra-group differences were confirmed. No statistically significant difference in depressive symptoms was found between the groups, but the rate of change in the UBPN01 group at the last point compared to baseline decreased by 16.26%. Depression increased by 14.34% in the placebo group.
There were no statistically significant differences in fatigue, arthralgia, or myalgia symptoms, but in the UBPN01 group, fatigue symptoms decreased by 6.5% at the last point compared to baseline and increased by 22.48% in the placebo group. Symptoms or arthralgia and myalgia also decreased by 10.16% in the UBPN01 group and increased by 17.44% in the placebo group.
The rate of change in headache decreased by 6.5% (UBPN01) and 5.43% (placebo), and palpitations decreased by 5.69% (UBPN01) and 0.39% (placebo). However, the rate of increase in formication was identified as 2.44% (UBPN01) and 11.6% (placebo).
In the case of vaginal dryness caused by vaginal atrophy due to lack of female hormones, an average reduction rate of 18.20% in the UBPN01 group and 1.16% in the placebo group was confirmed.
In the UBPN01 group, the symptoms of all individual items were improved except for formication, but in the placebo group, symptoms except insomnia, paraesthesia, nervousness, headache, palpitations, and vaginal dryness continued to worsen. Therefore, the rate of change of individual items showed better results in the UBPN01 group from baseline to EOT than in the placebo group.
The menopause rating scale (MRS) consists of 11 items of symptoms/comfort, each of which was scored from 0 to 4 points depending on the degree of symptoms/comfort felt by the subjects in the study. The degree of symptoms was evaluated and scored as none (0), mile (1), moderate (2), severe (3), or very severe (4). It was confirmed that there was a statistically significant difference in the MRS, and the average reduction rate at the last point compared to the baseline was 18.47% in the UBPN01 group and 5.15% in the placebo group. Therefore, the severity of the symptoms decreased over time with use of UBPN01. Vaginal pH decreased by 3.22% in the UBPN01 group and increased by 1.95% in the placebo group. Thus, symptoms related to menopause as evaluated by modified KI and MRS were found to improve when UBPN01 was ingested.
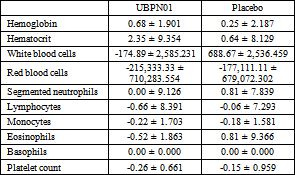
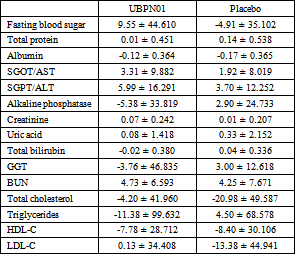
3.3. Evaluation of the Quality of LifeThe safety analysis group took UBPN01 or placebo at least once and included randomly assigned subjects. The results of the blood biochemical test indicated no significant change in all test items.
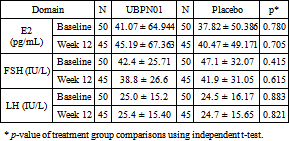
The E2, FSH and LH of the subjects were measured to check the safety of the UBPN01. The change in estradiol (pg/mL) from baseline to EOT was compared within the treatment groups. From the table, the p-value was observed to be greater than 0.05 for the UBPN01 treatment group or placebo, indicating that there was no statistically significant change from baseline. We found that the maximum value of estradiol was 366 pg/mL in the UBPN01 group and 259 pg/mL in the placebo group at baseline. The probable causes for the increase in estradiol in some subjects are increases in weight and other circulating androgens.
We observed that the obtained minimum value of FSH was 3.39 IU/L in the UBPN01 group and 3.39 IU/ml in the placebo group at baseline. When the difference between the baseline of EOT and change after 12 weeks was observed at the FSH level, the p-value between the groups was greater than 0.05, indicating no statistically significant difference. LH level also observed that when the difference between the criteria of EOT and the change after 12 weeks was confirmed, the p-value between groups was greater than 0.05, so there was no statistically significant difference.
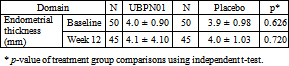
In the Table 7, the p-value was greater than 0.05 for the UBPN01 group, which indicates no statistically significant change from baseline. However, in the placebo group, we observed a statistically significant change from baseline to EOT with an average decrease of 3.9 mm of endometrial thickness.
Out of 100 participants, nine were reported to have adverse events. Seven subjects in the UBPN01 group and two subjects in the placebo group reported AEs. One subject in the UBPN01 group experienced two adverse events. The reported adverse events in the UBPN01 group were cold (16.7%), itching (16.7%), skin rashes (16.7%), toothache (16.7%), vomiting (33.3%), and stomachache (100.0%). They reported that the most common adverse events in the placebo group were fever (50.0%), and there were three episodes of vomiting and stomach pain (epigastric pain) (50.0%). The adverse events were evaluated by the researcher and were confirmed to be unrelated to the UBPN01 or placebo consumed by the subjects. The adverse reactions were all mild; death and other significant adverse reactions were not observed due to the end of study of participation, and clinically significant laboratory test numbers were not observed. In addition, no clinically significant vital signs or physical examination results were reported through the research.
Therefore, consumption of 1,000mg of UBPN01 significantly improved menopausal symptoms and is safe for healthy menopausal women.
This study was a randomized, double-blinded, placebo-controlled study to evaluate the efficacy and safety of UBPN01 in healthy women with postmenopausal syndrome. It was conducted after recruiting healthy women from the age of 40 to 60 years during menopause transition or menopause after obtaining written consent. Registered subjects (n=100) were randomly assigned to one of two groups (group 1: UBPN01, group 2: placebo) at a ratio of 1:1 for 12 weeks (84 ± 5 days). Due to failure of follow-up observation, five subjects in each group were eliminated. The test group ingested one UBPN01 soft capsule twice a day with water, and the placebo group ingested one placebo soft capsule twice a day with water. Demographic factors (date of birth, age, gender, marital status, drinking status, smoking status) and physical examination items (weight, height, and BMI) were identified and recorded in both groups.
The KI is a short-term measurement of the symptoms commonly associated with menopause and representing the quality of life of menopausal women. However, it has been criticized for not including urinary tract symptoms, which are thought to be common in menopausal women 23, 24. The modified version adds urogenital symptoms in the form of urinary infection, and so overcomes the limitations of the original KI. The modified KI used in the study was updated in the original index and is widely used in China 25.
In this study, participants who received UBPN01 treatment for 12 weeks showed reduction in modified KI scores relative to baseline scores. As a result, in the UBPN01 group, all individual items except vertigo, arthralgia and myalgia, palpitation, and formication symptoms were statistically significant. In the placebo group, only the symptoms of nervousness and insomnia were statistically significant.
Vaginal dryness is a typical female sexual dysfunction. When female hormones are deficient, vaginal atrophy changes appear, resulting in decreased elasticity and decreased vascular distribution that cause vaginal dryness. More than 50% of all women or 80% of menopausal women experience vaginal dryness, and vaginal dryness occurs mainly in menopausal women. Menopausal women took UBPN01 or placebo for 12 weeks, and the change before and after ingestion of placebo was very slight at 1.16%, but vaginal dryness improved by 18.20% after ingestion of UBPN01.
Estrogen, a female hormone, is involved in the regulation of serotonin, a neurotransmitter that controls emotions in the brain. A decrease in estrogen can lead to depression. There-fore, the more severe are the menopausal symptoms, the worse is the depression. Depression increased by 14.34% when placebo was ingested for 12 weeks but decreased by 16.26% when UBPN01 was ingested. Consumption of UBPN01 can improve the quality of life of menopausal women because it is effective in improving emotional anxiety disorders caused by reduced estrogen.
The values of estradiol, FSH, and LH were confirmed as safety evaluation variables, and no significant change was observed with UBPN01 consumption. The main ingredient of UBPN01 used in this study is S. miltiorrhiza, which has been reported to improve female hormone-related diseases (osteoporosis, hot flash, menopause, etc.) since ancient times. However, clinical trials for female menopause using an S. miltiorrhiza extract alone have not been conducted.
In summary, we report an improvement in menopausal symptoms following UBPN01 treatment according to the results of a randomized, double-blinded, placebo-controlled clinical trial. Consumption of UBPN01 has been found to have a clinically significant effect on menopausal symptoms in women and to have an excellent effect on depression and vaginal dryness among menopausal symptoms. In addition, it was confirmed to be safe for healthy subjects suffering from menopausal symptoms.
This research was funded by UNDBIO Co., Ltd (2018).
| [1] | Nelson, H.D. Menopause. Lancet. Elsevier Publishers. 760-770. | ||
| In article | View Article | ||
| [2] | Avis, N.E, Stellato, R, Crawford, S, Bromberger, J, Ganz, P, Cain, V. “Is there a menopausal syndrome? Menopausal status and symptoms across racial/ethnic groups,” Social Science & Medicine. 52 (3). 345-356. Feb. 2001. | ||
| In article | View Article | ||
| [3] | Dennerstein, L, Dudley, E.C, Hopper, J.L, Guthrie, J.R, Burger, H.G. “A prospective population-based study of menopausal symptoms,” Obstet Gynecol., 96(3). 351-358. Aug. 2000. | ||
| In article | View Article PubMed | ||
| [4] | Casper, R.F, Yen, S.S. “Neuroendocrinology of menopausal flushes: a hypothesis of flush mechanism,” Clinical Endocrinology, 22(3). 293-312. Mar. 1985. | ||
| In article | View Article PubMed | ||
| [5] | Brown, W.J, Mishra, G.D, Dobson, A. “Changes in physical symptoms during the menopause transition,” International Journal of Behavioral Medicine, 9. 53-67. Mar. 2002. | ||
| In article | View Article PubMed | ||
| [6] | Patel, S. “Disruption of aromatase homeostasis as the cause of a multiplicity of ailments: A comprehensive review,” Journal of Steroid Biochemistry & Molecular Biology, 168. 19-25. Apr. 2017. | ||
| In article | View Article PubMed | ||
| [7] | Ruiz-Cabello, P, Coll-Risco, I, Acosta-Manzano, P, Borges-Cosic, M, Gallo-Vallejo, F.J, Aranda, P, Lopez-Jurado, M, Aparicio, V.A. “Influence of the degree of adherence to the Mediterranean diet on the cardiometabolic risk in peri and menopausal women,” Nutrition, Metabolism and Cardiovascular Diseases, 27(3). 217-224. Mar. 2017. | ||
| In article | View Article PubMed | ||
| [8] | Zago, V, Sanguinetti, S, Brites, F, Berg, G, Verona, J, Basilio, F, Wikinski, R, Schreier, L. “Impaired high density lipoprotein antioxidant activity in healthy postmenopausal women,” Atherosclerosis, 177(1). 203-210. Nov. 2004. | ||
| In article | View Article PubMed | ||
| [9] | Roa-Diaz, Z.M.; Raguindin, P.F.; Bano, A.; Laine, J.E.; Muka, T.; Glisic, M. “Menopause and cardiometabolic diseases: What we (don't) know and why it matters,” Maturitas, 152. 48-56. Oct. 2021 | ||
| In article | View Article PubMed | ||
| [10] | Kupperman, H.S, Blatt, M.H, Wiesbader, H, Filler, W. “Comparative clinical evaluation of estrogenic preparations by the menopausal and amenorrheal indices,” The Journal of Clinical Endocrinology and Metabolism, 13(6). 688-703. Jun. 1953. | ||
| In article | View Article PubMed | ||
| [11] | Tao, M.F, Shao, H.F, Li, C.B, Teng, Y.C. “Correlation between the modified Kupperman Index and the Menopause Rating Scale in Chinese women,” Patient Prefer Adherence, 7. 223-229. Mar. 2013. | ||
| In article | View Article PubMed | ||
| [12] | Heinemann, L.A, Potthoff, P, Schneider, H.P. “International versions of the Menopause Rating Scale (MRS),” Health and Quality of Life Outcomes, 28(1). Jul. 2003. [Online]. Available: https://hqlo.biomedcentral.com/articles/10.1186/1477-7525-1-28 [Accessed Jul. 30. 2003]. | ||
| In article | View Article PubMed | ||
| [13] | Wu, Y.L, Lin, H, Li, H.F, Don, M.J, King, P.C, Chen, H.H. “Salvia miltiorrhiza Extract and Individual Synthesized Component Derivatives Induce Activating-Transcription-Factor-3-Mediated Anti-Obesity Effects and Attenuate Obesity-Induced Metabolic Disorder by Suppressing C/EBP alpha in High-Fat-Induced Obese Mice,” Cells, 11(6). Mar. 2022. [Online] Available: https://www.mdpi.com/2073-4409/11/6/1022 | ||
| In article | View Article PubMed | ||
| [14] | Ji, X.Y, Tan, B.K, Zhu, Y.Z. “Salvia miltiorrhiza and ischemic diseases,” Acta Pharmacologica Sinica, 21(12). 1089-1094. Dec. 2000. | ||
| In article | |||
| [15] | Tian, D.D.; Jia, W.W.; Liu, X.W.; Wang, D.D.; Liu, J.H.; Dong, J.J.; Li, L.; Du, F.F.; Xu, F.; Wang, F.Q.; et al. “Methylation and its role in the disposition of tanshinol, a cardiovascular carboxylic catechol from Salvia miltiorrhiza roots (Danshen),” Acta Pharmacologica Sinica, 36. 627-643. Apr. 2015. | ||
| In article | View Article PubMed | ||
| [16] | Guo, Y, Sun, J, Zhang, R, Yang, P, Zhang, S, Wu, Z. “Salvia miltiorrhiza improves type 2 diabetes: A protocol for systematic review and meta-analysis,” Medicine (Baltimore), 100(6). Feb. 2021 [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7886461/. | ||
| In article | View Article PubMed | ||
| [17] | Nagappan, A, Kim, J.H, Jung, D.Y, Jung, M.H. “Cryptotanshinone from the Salvia miltiorrhiza Bunge Attenuates Ethanol-Induced Liver Injury by Activation of AMPK/SIRT1 and Nrf2 Signaling Pathways,” International Journal of Molecular Sciences, 21(1). Dec. 2019. [Online] Available: https://www.mdpi.com/1422-0067/21/1/265. | ||
| In article | View Article PubMed | ||
| [18] | Kim, J.M, Noh, E.M, Song, H.K, Lee, M, Lee, S.H, Park, S.H, Ahn, C.K, Lee, G.S, Byun, E.B, Jang, B.S. et al. “Salvia miltiorrhiza extract inhibits TPA-induced MMP-9 expression and invasion through the MAPK/AP-1 signaling pathway in human breast cancer MCF-7 cells,” Oncology Letters 14. 3594-3600. Jul. 2017. | ||
| In article | View Article PubMed | ||
| [19] | Lee, S.R, Jeon, H, Kwon, J.E, Suh, H, Kim, B.H, Yun, M.K, Lim, Y.J, Kang, S.C. “Anti-osteoporotic effects of Salvia miltiorrhiza Bunge EtOH extract both in ovariectomized and naturally menopausal mouse models,” Journal of Ethnopharmacology, 258. 112874. Aug. 2020. | ||
| In article | View Article PubMed | ||
| [20] | Park, B, Song, H.S, Kwon, J.E, Cho, S.M, Jang, S.A, Kim, M.Y, Kang, S.C. “Effects of Salvia miltiorrhiza extract with supplemental liquefied calcium on osteoporosis in calcium-deficient ovariectomized mice,” BMC Complementary and Alternative Medicine, 545(17). Dec. 2017. [Online] Available: https://link.springer.com/article/10.1186/s12906-017-2047-y. | ||
| In article | View Article PubMed | ||
| [21] | Zhang, X, Zheng, W, Wang, T, Ren, P, Wang, F, Ma, X, Wang, J, Huang, X. “Danshen-Chuanxiong-Honghua Ameliorates Cerebral Impairment and Improves Spatial Cognitive Deficits after Transient Focal Ischemia and Identification of Active Compounds,” Frontiers in Pharmacology, 8(452). Jul. 2017 [Online] Available: https://www.frontiersin.org/articles/10.3389/fphar.2017.00452/full. | ||
| In article | View Article PubMed | ||
| [22] | Gu, S, Ma, Y, Ge, K, Nie, R, Wu, E, Li, Y. “Danshen-Honghua Ameliorates Stress-Induced Menopausal Depression in Rats,” Neural Plasticity, 2018(6589608). May. 2018. [Online] Available: https://www.hindawi.com/journals/np/2018/6589608/. | ||
| In article | View Article PubMed | ||
| [23] | Alder, E. “The Blatt-Kupperman menopausal index: a critique,” Maturitas, 29(1). 19-24. May. 1998. | ||
| In article | View Article | ||
| [24] | Schneider, H.P, Heinemann, L.A, Rosemeier, H.P, Potthoff, P, Behre, H.M. “The Menopause Rating Scale (MRS): comparison with Kupperman index and quality-of-life scale SF-36,” Climacteric, 3:1. 50-58. Jan. 2000. | ||
| In article | View Article PubMed | ||
| [25] | Ahn, K, Kim, S, Yi, K, Park, H, Shin, J, Kim, Y, Hur, J, Kim, S, Lee, K, Kim, T. “The Effect of Pomegranate on Postmenopausal Syndrome A Randomized, Double-blind, Placebo-controlled Trial,” The Journal of Korean Society of Menopause, 16(2). 99-106. Aug. 2010. | ||
| In article | |||
Published with license by Science and Education Publishing, Copyright © 2022 Jeong Eun Kwon, Yeong-Geun Lee, Tae Hee Kim, Gyoungok Gang, Gokce Altun, Farzana Mushtaq Ahmed, Narayanaswamy Venkatappa, Hyukjin Kwon, Jihyeong Park and Se Chan Kang
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Nelson, H.D. Menopause. Lancet. Elsevier Publishers. 760-770. | ||
| In article | View Article | ||
| [2] | Avis, N.E, Stellato, R, Crawford, S, Bromberger, J, Ganz, P, Cain, V. “Is there a menopausal syndrome? Menopausal status and symptoms across racial/ethnic groups,” Social Science & Medicine. 52 (3). 345-356. Feb. 2001. | ||
| In article | View Article | ||
| [3] | Dennerstein, L, Dudley, E.C, Hopper, J.L, Guthrie, J.R, Burger, H.G. “A prospective population-based study of menopausal symptoms,” Obstet Gynecol., 96(3). 351-358. Aug. 2000. | ||
| In article | View Article PubMed | ||
| [4] | Casper, R.F, Yen, S.S. “Neuroendocrinology of menopausal flushes: a hypothesis of flush mechanism,” Clinical Endocrinology, 22(3). 293-312. Mar. 1985. | ||
| In article | View Article PubMed | ||
| [5] | Brown, W.J, Mishra, G.D, Dobson, A. “Changes in physical symptoms during the menopause transition,” International Journal of Behavioral Medicine, 9. 53-67. Mar. 2002. | ||
| In article | View Article PubMed | ||
| [6] | Patel, S. “Disruption of aromatase homeostasis as the cause of a multiplicity of ailments: A comprehensive review,” Journal of Steroid Biochemistry & Molecular Biology, 168. 19-25. Apr. 2017. | ||
| In article | View Article PubMed | ||
| [7] | Ruiz-Cabello, P, Coll-Risco, I, Acosta-Manzano, P, Borges-Cosic, M, Gallo-Vallejo, F.J, Aranda, P, Lopez-Jurado, M, Aparicio, V.A. “Influence of the degree of adherence to the Mediterranean diet on the cardiometabolic risk in peri and menopausal women,” Nutrition, Metabolism and Cardiovascular Diseases, 27(3). 217-224. Mar. 2017. | ||
| In article | View Article PubMed | ||
| [8] | Zago, V, Sanguinetti, S, Brites, F, Berg, G, Verona, J, Basilio, F, Wikinski, R, Schreier, L. “Impaired high density lipoprotein antioxidant activity in healthy postmenopausal women,” Atherosclerosis, 177(1). 203-210. Nov. 2004. | ||
| In article | View Article PubMed | ||
| [9] | Roa-Diaz, Z.M.; Raguindin, P.F.; Bano, A.; Laine, J.E.; Muka, T.; Glisic, M. “Menopause and cardiometabolic diseases: What we (don't) know and why it matters,” Maturitas, 152. 48-56. Oct. 2021 | ||
| In article | View Article PubMed | ||
| [10] | Kupperman, H.S, Blatt, M.H, Wiesbader, H, Filler, W. “Comparative clinical evaluation of estrogenic preparations by the menopausal and amenorrheal indices,” The Journal of Clinical Endocrinology and Metabolism, 13(6). 688-703. Jun. 1953. | ||
| In article | View Article PubMed | ||
| [11] | Tao, M.F, Shao, H.F, Li, C.B, Teng, Y.C. “Correlation between the modified Kupperman Index and the Menopause Rating Scale in Chinese women,” Patient Prefer Adherence, 7. 223-229. Mar. 2013. | ||
| In article | View Article PubMed | ||
| [12] | Heinemann, L.A, Potthoff, P, Schneider, H.P. “International versions of the Menopause Rating Scale (MRS),” Health and Quality of Life Outcomes, 28(1). Jul. 2003. [Online]. Available: https://hqlo.biomedcentral.com/articles/10.1186/1477-7525-1-28 [Accessed Jul. 30. 2003]. | ||
| In article | View Article PubMed | ||
| [13] | Wu, Y.L, Lin, H, Li, H.F, Don, M.J, King, P.C, Chen, H.H. “Salvia miltiorrhiza Extract and Individual Synthesized Component Derivatives Induce Activating-Transcription-Factor-3-Mediated Anti-Obesity Effects and Attenuate Obesity-Induced Metabolic Disorder by Suppressing C/EBP alpha in High-Fat-Induced Obese Mice,” Cells, 11(6). Mar. 2022. [Online] Available: https://www.mdpi.com/2073-4409/11/6/1022 | ||
| In article | View Article PubMed | ||
| [14] | Ji, X.Y, Tan, B.K, Zhu, Y.Z. “Salvia miltiorrhiza and ischemic diseases,” Acta Pharmacologica Sinica, 21(12). 1089-1094. Dec. 2000. | ||
| In article | |||
| [15] | Tian, D.D.; Jia, W.W.; Liu, X.W.; Wang, D.D.; Liu, J.H.; Dong, J.J.; Li, L.; Du, F.F.; Xu, F.; Wang, F.Q.; et al. “Methylation and its role in the disposition of tanshinol, a cardiovascular carboxylic catechol from Salvia miltiorrhiza roots (Danshen),” Acta Pharmacologica Sinica, 36. 627-643. Apr. 2015. | ||
| In article | View Article PubMed | ||
| [16] | Guo, Y, Sun, J, Zhang, R, Yang, P, Zhang, S, Wu, Z. “Salvia miltiorrhiza improves type 2 diabetes: A protocol for systematic review and meta-analysis,” Medicine (Baltimore), 100(6). Feb. 2021 [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7886461/. | ||
| In article | View Article PubMed | ||
| [17] | Nagappan, A, Kim, J.H, Jung, D.Y, Jung, M.H. “Cryptotanshinone from the Salvia miltiorrhiza Bunge Attenuates Ethanol-Induced Liver Injury by Activation of AMPK/SIRT1 and Nrf2 Signaling Pathways,” International Journal of Molecular Sciences, 21(1). Dec. 2019. [Online] Available: https://www.mdpi.com/1422-0067/21/1/265. | ||
| In article | View Article PubMed | ||
| [18] | Kim, J.M, Noh, E.M, Song, H.K, Lee, M, Lee, S.H, Park, S.H, Ahn, C.K, Lee, G.S, Byun, E.B, Jang, B.S. et al. “Salvia miltiorrhiza extract inhibits TPA-induced MMP-9 expression and invasion through the MAPK/AP-1 signaling pathway in human breast cancer MCF-7 cells,” Oncology Letters 14. 3594-3600. Jul. 2017. | ||
| In article | View Article PubMed | ||
| [19] | Lee, S.R, Jeon, H, Kwon, J.E, Suh, H, Kim, B.H, Yun, M.K, Lim, Y.J, Kang, S.C. “Anti-osteoporotic effects of Salvia miltiorrhiza Bunge EtOH extract both in ovariectomized and naturally menopausal mouse models,” Journal of Ethnopharmacology, 258. 112874. Aug. 2020. | ||
| In article | View Article PubMed | ||
| [20] | Park, B, Song, H.S, Kwon, J.E, Cho, S.M, Jang, S.A, Kim, M.Y, Kang, S.C. “Effects of Salvia miltiorrhiza extract with supplemental liquefied calcium on osteoporosis in calcium-deficient ovariectomized mice,” BMC Complementary and Alternative Medicine, 545(17). Dec. 2017. [Online] Available: https://link.springer.com/article/10.1186/s12906-017-2047-y. | ||
| In article | View Article PubMed | ||
| [21] | Zhang, X, Zheng, W, Wang, T, Ren, P, Wang, F, Ma, X, Wang, J, Huang, X. “Danshen-Chuanxiong-Honghua Ameliorates Cerebral Impairment and Improves Spatial Cognitive Deficits after Transient Focal Ischemia and Identification of Active Compounds,” Frontiers in Pharmacology, 8(452). Jul. 2017 [Online] Available: https://www.frontiersin.org/articles/10.3389/fphar.2017.00452/full. | ||
| In article | View Article PubMed | ||
| [22] | Gu, S, Ma, Y, Ge, K, Nie, R, Wu, E, Li, Y. “Danshen-Honghua Ameliorates Stress-Induced Menopausal Depression in Rats,” Neural Plasticity, 2018(6589608). May. 2018. [Online] Available: https://www.hindawi.com/journals/np/2018/6589608/. | ||
| In article | View Article PubMed | ||
| [23] | Alder, E. “The Blatt-Kupperman menopausal index: a critique,” Maturitas, 29(1). 19-24. May. 1998. | ||
| In article | View Article | ||
| [24] | Schneider, H.P, Heinemann, L.A, Rosemeier, H.P, Potthoff, P, Behre, H.M. “The Menopause Rating Scale (MRS): comparison with Kupperman index and quality-of-life scale SF-36,” Climacteric, 3:1. 50-58. Jan. 2000. | ||
| In article | View Article PubMed | ||
| [25] | Ahn, K, Kim, S, Yi, K, Park, H, Shin, J, Kim, Y, Hur, J, Kim, S, Lee, K, Kim, T. “The Effect of Pomegranate on Postmenopausal Syndrome A Randomized, Double-blind, Placebo-controlled Trial,” The Journal of Korean Society of Menopause, 16(2). 99-106. Aug. 2010. | ||
| In article | |||