The objective of this study was to assess the nutritional status of displaced and non-displaced children in a context of security crisis in North Center of Burkina Faso. The study population comprised 205 internally displaced children and 167 non-displaced children, all aged 6 to 59 months, and their mothers/primary caregivers living in the commune of Kaya in North Center of Burkina Faso. Children were selected using a two-stage cluster sampling procedure. This cross-sectional study was carried out between June-July 2020. Demographic characteristics, child nutrition and health status, and maternal and household information were collected from mothers through interviews. The distribution of different nutritional status, such as underweight, stunting and wasting and malnutrition-related factors was analyze. The overall prevalent rates of underweight, wasting and stunting were 20.4%, 13.7% and 33.6%, respectively. In the group of displaced children, these were 21.5%, 12.2% and 37.1%, while in the non-displaced, they were 19.2%, 15.6% and 29.3%, respectively. The mean nutritional indices were found to be significantly lower among the displaced children than non-displaced (P<0.001). The present study revealed that in the multivariate analysis, diarrhoea and ARI, mother’s BMI < 18.5 kg/m2, LBW < 2.5 kg, household size of five and above using a latrine and source of drinking water were positively associated with malnutrition of children in both communities. Prevention of malnutrition should be given a high priority in the implementation of the ongoing primary health care programmes with particular attention paid to the displaced populations.
• The study shows that internally displaced and non-displaced children face multiple health and nutrition problems.
• Internally displaced children are at increased risk of infectious diseases, as well as increased difficulties in accessing health and sanitation services.
• The study indicates poorer nutritional status among internally displaced children and a poorer status among non-displaced children.
• There is a complex chain of factors that have a significant impact on the health and nutrition of displaced and non-displaced children, and further intervention studies are needed to understand ways of improving health and nutrition.
At the end of 2020, some 48 million people were internally displaced glogally 1. Sub-Saharan Africa is affected by massive internal displacement, with some 18.5 million people displaced on the continent in 2019. 2. Internal displacement in sub Saharan Africa was higher than in any other region in 2018,with approximately 7.4 million people displaced due to conflict and violence 3. According to the United Nations Guiding Principles on Internal Displacement, internally displaced persons (IDPs) are ‘persons or groups of persons who have been forced or obliged to flee or to leave their homes or places of habitual residence, in particular as a result of or in order to avoid the effects of armed conflict, situations of generalized violence, violations of human rights or natural or human-made disasters, and who have not crossed an internationally recognized State border’ 4. They are among the most vulnerable populations in the world. Children are a particularly vulnerable group of IDPs because they have health needs that are unique to adult health needs. Therefore, they may be left unsupported by general health service provision 5.
There is limited information on the health status and malnutrition of displaced children in the North Center of Burkina Faso, a region with the largest number of IDPs. This is significant given that displacement exacerbates the already existing diverse health challenges of these individuals. Since 2015, Burkina Faso has been experiencing enormous difficulties linked to a security and health crisis in previous years. This security crisis has resulted in nearly one and a half million displaced people from the countryside to the cities. In Burkina Faso, child malnutrition constitutes a particularly daunting challenge as the country had a 54 % under-five mortality rate in 2019, of which the majority was linked to malnutrition 6. According to the 2020 SMART (Standardised Monitoring and Assessment of Relief and Transitions), among children under age five, 24.9% were stunted, 17.6% are underweight, and 9.1% were wasted 7. In Burkina Faso, more than a third of the deaths of children under five are directly or indirectly attributable to malnutrition 8.
According to the SMART survey conducted in 2019 among children under five in the north-central region, it emerged that 19.7% of displaced children suffer from acute malnutrition, including 7.8% in severe form. Among non-displaced children, this prevalence of acute malnutrition was 9.4%, of which 2.6% was severe 9. The nutritional situation is much more worrying among displaced children with a prevalence exceeding the emergency threshold of 10%.
The commune of Kaya in the north-center of Burkina Faso is home to more than 50% of these displaced populations, of which more than 17% are children under the age of five 10. This security situation has also disrupted the functioning of the health system and the implementation of activities to combat malnutrition in several localities of the country.
This context is then marked by the deterioration of the food and nutritional situation of the populations already weakened by climatic hazards in this region. This situation has a negative impact on the way of life of displaced people, host communities. In addition, this region was already confronted with the highest infant and child mortality rate, going from 81.6‰ in 2015 to 54% in 2019. Among the main causes of child mortality, malaria represents 23, 8%, neonatal conditions 21.9%, acute respiratory infections 13.4% and diarrhoea 11.5% 11.
Access to drinking water, hygiene and sanitation conditions remains precarious. Indeed, the rate of access to drinking water and sanitation is 69.5% and 19.9% respectively 12, 13.
The objective of the study was to determine the nutritional status of displaced children and non-displaced in the Kaya commune in North Center of Burkina Faso. The study also makes important contribution to future research by contributing to the existing literature particularly on nutrition among under-five children. The finding further avails information that could be used in policy planning and implementation particularly in children under five.
The study was carried out in the commune of Kaya located in the province in the North Center region of Burkina Faso.
The North Center region covers an area of 19,508 km2 and representing 7.1% of the national territory. It is limited to the North by the Sahel region, to the South by the Central Plateau and Center-East regions, to the East by the East region and to the West by the North region 14. The North Center region has three (03) provinces (Bam, Namentenga and Sanmatenga), and eight hundred and thirty-five (835) villages with a population of 1,639,966 inhabitants 15. In 2019, the population was estimated at 172,103 Inhabitants in 2019 16. Children under five represented around 18.52% of the population. There were 55 health workers in 09 health centers 15. The most of the population (80.0%) practice agriculture as their main occupation while some are involved in commerce. The main staple foods, including maize, sorghum and millet are generally harvested from November until December. The food security situation is generally quite good during the harvest period, but becomes poor from June 17.
According to the 2019 SMART survey, 23.3% of children age 6 to 23 months consumed at least 4 food groups and 18.0% had a minimum acceptable diet. According to the Food Crisis Prevention Network, 35% of the population in the North Center are food insecure 17. Indeed, according to the SMART survey, the prevalence of diarrhea in children under five years of age decreased from 20.8% in 2018 to 19.6% in 2019 7.
It was observed that 46.5% of households in the municipality do not use water, soap, or other cleaning product to wash their hands 18.
2.2. Study Type and Target PopulationsIt was a community-based cross-sectional study for descriptive and analytical purposes. Anthropometric and health data were collected in children under 5 years of age. The children's mothers were questioned.
2.3. Study Population and SamplingTwo types of sampling have been proposed depending on whether the population lives in a reception site or dispersed in the community.
The sampling technique used for the survey in the communities is a two-stage probability cluster survey stratified according to the residence status of the respondent.
Out of 36 districts in the municipality, 21 were randomly selected. The total sample size was distributed to each district proportionally based on the number of households in the district, using the probability proportional to size method.
The first-stage selection was the drawing of 500 households from the database of host households for the survey. Then, a systematic random sampling technique was used to select study participants from the households selected for measures. Children who were seriously ill during data collection and households absent after two visits by the interviewers were excluded. The minimum sample size was estimated at 159 children with a non-response margin of 5%.
Second-degree selection concerned children aged 6 to 59 months. In each selected household, a census of the targets according to the status of residence was made and all were surveyed.
Mothers or care givers were interviewed on socio-demographic, economic, child health related characteristics and environmental conditions with a pre-tested structured questionnaire. Detailed description of the sample design is available in another publication 19.
Internally displaced populations have been distributed to five reception sites. The selection of the sample was made in the host sites through a simple systematic random survey. A total of 500 internally displaced households spread over eleven villages were randomly drawn from the database of internally displaced persons (IDPs). In each selected household, all children aged 6 to 59 months were counted. Seriously ill children and households absent from the site after two visits by the interviewers are excluded from the study. The minimum sample size was estimated at 195 children with a non-response margin of 5%.
2.4. Data Collection and AnalysisData were collected by well-trained community health workers from June-July 2020. Mothers or care givers were interviewed and anthropometry measurement (height, weight and upper mid-arm circumference) was taken on children.
Height of children aged six months to 23 months was measured in a recumbent position to the nearest 0.1 cm, using a board with an upright wooden base and movable headpieces. Children aged 24 to 59 months were measured in a standing up position to the nearest of 0.1 cm.
Additionally, child weight was measured by an electronic digital weight scale for children who were comfortable to be measured alone, and also for children who were uncomfortable to be measured alone, we used the combined mother and child weight and the mother's individual weight to calculate the child's weight 3. The Categories of morbidity status were based on the types of diseases that the child encountered in the previous fourteen weeks. For instance, if the child had one type of disease it will be categorized as one disease. Data were collected via the ODK (Open Data Kit) application using forms implemented.
Data on sex, age, height, and weight was transferred with participants' identification number to ENA (Emergency Nutrition Assessment) software for SMART software to convert nutritional data into Z scores of the indices HAZ, WHZ and WAZ using the WHO standard. The anthropometry measurement of height for age (HAZ), weight for age (WAZ) and weight for height (WHZ) was calculated through ENA SMART software, and children less than -2 SD were classified as moderate malnutrition.
Those children with indices between -2 and -3 SD were classified as moderate malnutrition while <-3 SD were classified as severe malnutrition. Data was also exported to STATA (Stata Statistical) Software 14 for further analysis and identification of factors associated with malnutrition by the binary logistic regression model. Variables with a p-value less than or equal to 0.05 in the bivariate analysis were included in the multivariate logistic regression model. The strength of association was determined by the Adjusted Odds Ratio (AOR) a 95% confidence interval and p-value < 0.05 was used to show the association between independent variables and the presence of malnutrition. Variables having p-value, of <0.05 were considered as statistically significant.
Differences in means were compared using Student’s t-test while ratios, rates and proportions were compared using chi square (2) test. Statistically significance level was taken as P-value <0.05.
2.5. Ethical ConsiderationsThe permission to carry out this study was sought from district health authorities and the study protocol was approved by the Institutional Ethics Committee for Research in Health Sciences, Burkina Faso. Approval was obtained on 6 March 2020 under the reference N/Ref.A10-2020/ CEIRES Informed consent was also obtained verbally after needed information and explanation. Participation was voluntary and each woman signed (or provided a thumb print if she was uneducated) a statement of an informed consent after which she was interviewed.
A total of 372 children aged 6 to 59 months were studied. Of these, 167 (44.9%) and 205 (55.1%) were the non-displaced children and displaced children, respectively.
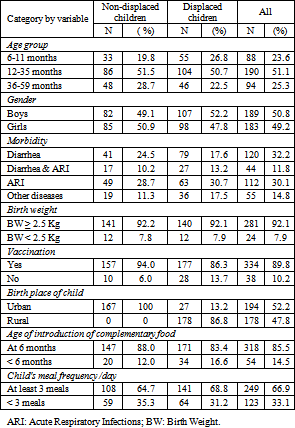
The group of non-displaced children were predominantly made up of 50.9% girls and 49.1% boys, on the other hand the displaced children had a male predominance of 52.2% and 47.8% girls. More than half of the children under five in the two groups were aged 12 to 35 months. Displaced children tended to be younger than non-displaced children. The same distribution was observed by gender.
In terms of child morbidity, non-displaced children (24.5%) and displaced children (17.6%) recently suffered from diarrhoea, fever and ARI, respectively. Most of the displaced children 58 (30.8%) had infectious diseases such as diarrhoea caused by infectious agents for the day before survey. Regarding maternal undernutrition, 70.20 % of displaced mothers had BMI ranging between 18.5 and 24.9 kg/m2 and 10.1 % were wasted. Additionally, 7.8% and 7.9% of non-displaced and displaced children respectively had low birth weight less than 2.5 kg (Table 1).
The majority (61.5%) of the displaced households used public well water for drinking. Wheras, 57 (30%), of the non-displaced households used the same water source.
Regarding the availability of toilet, 131 (84.4%) and 149 (72.7%) of non-displaced and displaced households had toilettes respectively; traditional pit latrines were most commonly used, whilst 56 (27.3%) displaced households used open field defecation (Table 1).
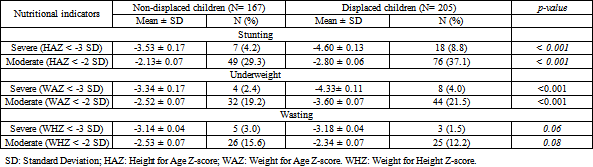
The group of displaced children was more affected by stunting than the group of non-displaced.
In fact, the mean HAZ <-3SD of displaced children was significantly higher than that of non-displaced (P <0.001). Similar trend was observed with the meanHAZ < -2SD nutritional indice (p< 0.001). The mean WAZ < -3 SD nutritional indice was higher among displaced children than non-displaced (p=0.01)
The group of non-displaced children tended to be wasted than displaced children, but the difference was not significant (Table 2).
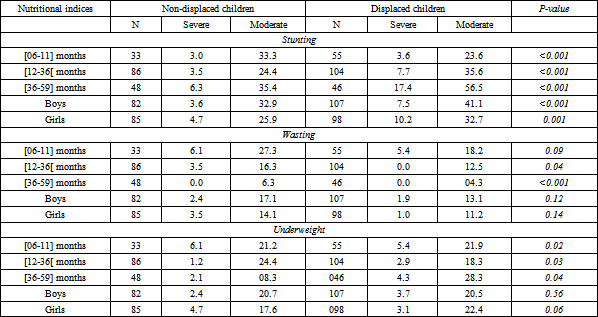
Table 3 shows the prevalence of malnutrition among non-displaced and displaced children by age group and gender.
The comparison of the nutritional status (Wasting) at different age groups of displaced children and non-displaced revealed higher prevalence of under-weight among 36–59 months in groups of displaced children. The difference was statistically significant in both communities (P <0.001). In the group of displaced children, the prevalence of severe underweight was 3.9%, and the highest prevalent rate of severe underweight of 5.4% was found among 6–11months age group while mild-moderate underweight prevalent rate was 28.3% among 36–59 months age group. In the group of non-displaced children, the prevalent rates of mild-moderate and severe underweight were 16.8 and 2.4%, respectively. The highest prevalence of 24.4% for mild-moderate underweight and 6.1% for severe underweight were found among 12–36 months and 6–11 months age groups, respectively.
The overall prevalence of wasting based on percentage weight for height of a reference median (WHM) was 13.7%. Twenty-six (15.6%) of the 167 non-displaced children and 25 (12.2%) of the 205 displaced children were wasted. The prevalence of wasting was higher among males non-displaced (17.1%) than males displaced (13.1%), the difference was statistically significant (p <0.001). Similar trend was observed in the girls. The prevalence of wasting was highest in the 6–11months age group in both group of displaced children and non-displaced communities, while it was lowest in age groups of 36–59 months. The prevalence of wasting was higher among 6–11 months age group when compared with 36–59 months age group in both communities. The differences were statistically significant in both areas (p-value for each group was <0.001).
The prevalence of stunting in the group of displaced and non-displaced communities were 37.1% and 29.3%, respectively, giving an overall prevalence of stunting as 33.6%. The prevalence of stunting was significantly higher in non-displaced than in displaced children (P<0.001). Table 4 compares the prevalence of stunting between female and male children in the group of non-displaced and displaced children. The prevalent of stunting had tended to be higher among females displaced children compared with non-displaced children. The difference was not statistically significant (Table 3).
The prevalence of stunting was highest among the children in the 36–59 months age group in non-displaced and displaced children, while the lowest prevalence of stunting was found among displaced children in the 6–11 months age group and the group age of non-displaced children in the 12-36 months. The prevalent rates of stunting in both groups were significantly higher in 36–59 months than 6–11 months age groups (P<0.001).
3.4. Coexistence of Under Nutrition in ChildrenTable 4 shows the coexistence of the two forms of malnutrition (stunting and wasting) in children. Overall, 2% of children are found to be both wasted and stunted. This prevalence is higher among non-displaced than displaced children (p < 0.001). Overall, 43.5% of children are wasted or stunted. This means that 54.6% of children escaped these two forms of malnutrition (wasting and stunting).
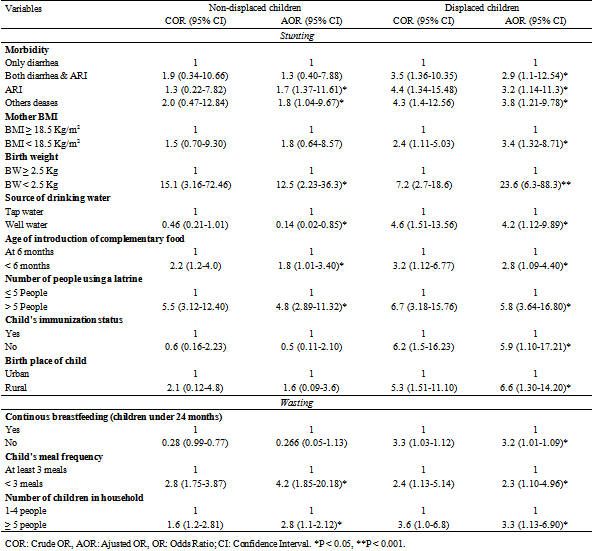
Child morbidity, low birth weight, source of drinking water, age of introduction of complementary food and number of people using a latrine were significantly associatedwith stunting in two groups of children (Table 5).
In displaced children specifically, mother’s BMI, child’s immunization status and birth place were significantly associated with stunting.
Child’s meal frequency and number children in household wer significantly associated with wasting in two groups of children, while no continous breastfeeding and number of children in household were significantly associated wasting in group of displaced children specifically.
Child morbidity was directly correlated with stunting. Accordingly, compared to non-displaced children, displaced children were 2.07 times more likely to be stunted [AOR = 2.07, 95% CI: (1.34, 3.18)]. Similarly, displaced children with malnourished mothers had 3.86 times more odds of being stunted than non-displaced children [AOR = 3.86, 95% CI: (2.50, 5.97)].
Thus displaced children without latrines had a stronger association with stunting. Displaced Children were 4.73 times [AOR = 4.73, 95% CI: (3.00, 10.91)] more stunted while non-displaced without latrines. Thus, displaced children with low meal frequency were 6.31 times more likely to be stunted compared to non-displaced children [AOR = 6.31, 95% CI: (3.65, 10.91)].
In addition, displaced children born rural area were 3.75 times [AOR = 6.60, 95% CI: (1.30, 14.20)] more likely to be stunted compared to children born in urban area (Table 5).
The overall prevalence of the different types of malnutrition in children in this study is higher than the recent national prevalence of malnutrition provided by the SMART surveys in 2020 7. This could be explained by the context of insecurity marked by massive internal displacement of populations. This is in agreement with the results of previous studies from other developing countries 7, 9. Another study conducted in the North Center of Burkina Faso showed that 13.9% of children were emaciated. This prevalence was higher than that reported in a recent study conducted in 2019 in the same region 9. Similarly, the prevalence of stunting was higher than those of studies conducted in southwest Ethiopia, which was 35.4% 20. Two studies conducted in Uganda and Zambia showed that internally displaced children often had poorer levels of nutritional health than non-displaced childrenand many bore the consequences thereof 21, 22.
The observation of high prevalence of undernutrition could be attributed to economic recession presently experienced and crisis security in Burkina Faso, thus undermining the gains from the child survival programmes. However, our study showed the highest prevalence of stunting among non-displaced children and among displaced children. This discrepancy could be explained by the context of insecurity and the occurrence of the COVID-19 pandemic, which had an impact on the living conditions of the population. Previous research indicates that children with moderate or severe wasting are at greater risk of death 23.
The mean HAZ and WAZ nutritional indices were lower in displaced children compared to non-displaced and could be attributed to the consequences of the security crisis marked by limited access to basic social services, leading to a deprivation of resources, rights of these populations and important needs in terms of protection, health, education, and water. Displaced children were less emaciated than their non-displaced brothers in host communities due to the special attention given to displaced communities, which could explain this result.
The high rate of wasting observed among non-displaced children could be explained by the poor water, sanitation and hygiene (WASH) practices in Kaya and insufficient treatment of malnutrition in health centers 24. In both groups studied, the prevalence of stunting and underweight increased with the age of the children whereas the prevalence of wasting seemed to decrease with age. This progressive increase in the prevalence of malnutrition with could have resulted from recent deterioration in socio-economic standards and living conditions in the country.
Consequently, this might have led to a situation where older children are left to fend for themselves, thereby exposing them to poor feeding that is inimical to their total wellbeing 8
Children aged 12 to 36 months have been reported by several studies to be a preferred age for the occurrence of malnutrition 25, 26, 27, 28. Similar observations reported by the survey SMART in 2016 revealed that this age group was the most affected by stunting 29. In addition, underweight was more pronounced in the 36 to 59 monts age group. Therefore, it is evident that a child's nutrition is dependent on his age. In effect, children aged 6 to 11 months should not be fed like children aged 12 to 36 months and the latter should not be fed like those aged to 36-59 months.
This situation would be explained by the poor child weaning practices, in particular the inadequate introduction of complementary foods that do not meet the nutritional needs of the children for his growth. Equally important factors that may adversely affect nutritional intake are traditional beliefs and practices that are more rooted in displaced children than non-displaced 30. For instance, it is believed that eating eggs may turn the child into a thief in later life and eating too much meat may give him worms.
Overall, boys were more affected by stunting and wasting in both groups. Male gender has been recognized by several authors as a risk factor for malnutrition, but other studies believe that gender disparities in child under nutrition may be due to gender differences in body composition, primarily muscle mass and the distribution of body fat measured by different anthropometric indicators 31, 32.
This study also reveals cumulative forms of malnutrition in children. The coexistence of stunting and wasting was more pronounced in the non-displaced children. Our results corroborated with a recent analysis which showed an over all prevalence of both wasted and stunted children ranging from 0% to 8.0% in children aged 6 to 59 months in 84 countries 33.
Others studies indicated an increased risk of mortality for children with multiple anthropometric deficits 23. Non-displaced children who were both wasted and stunted are 12 times more likely to die than children who were neither wasted nor stunted. The same high risk of mortality is estimated in children with severe wasting 23.
Thus, it would be more interesting if the management or prevention approaches jointly address wasting and stinting in the environments where they coexist. Evidence suggests that wasting and stunting share the same underlying and fundamental causal factors 25. This present study has explored the prevalence of malnutrition and its associated factors in two groups of children.
Higher prevalence of infectious diseases like malaria and diarreha with inadequate health care may contribute higher occurrences of child stunting in our study subjects 34, 35. However, the magnitude of stunting in the study area is much higher compared to the national prevalence and efforts should be made to alleviate the problem 7. Also this study showed that the prevalence of wasting is higher in the displaced mothers.
This might be due to the nutritional status of the mother since stunting has a chronic and cyclic nature, poor dietary practice, weaning, lower and inappropriate breast and complementary feeding practices. The other possible explanation for increased risk of stunting in displaced children may be due to unhygienic preparation of complementary foods which exposes children to recurrent infections. Limited access to safe drinking water in the study area also exposes these children to varied types of infections and diarrheal diseases which further increase the risk of chronic malnutrition.
Children with birth weight of less than 2.5 kg were more likely to be underweight, stunted or wasted. Similarly, the aprevious study in Bangladesh showed a very strong positive association between low birth weight and malnutrition among children < 5 years 36. The association between infection and child malnutrition is bidirectional 37, 38, 39, and this study showed that child morbidity, such as diarrhea, fever and ARI were associated with malnutrition of children in both groups.
The present study reported that diarrhea and ARI increased the risk of being stunting. In addition, fever was shown as a risk factor for being underweight, while ARI was found as a risk factor for being wasting. The displaced children were more vulnerable to be infected possibly due to their living environment such as the source of drinking water and household sanitations.
The childhood illness could be prevented by educational intervention related to child healthcare and the implementation of integrated community case management to improve the health and hygiene practices 40, 41. Optimal quality of health care must be guaranteed to all children 42. According to a systematic review conducted by Owoaje et al 43 on the health problems of IDPs in Africa, the most prevalent symptoms among children were fever, cough and diarrhoea. Demographic factors associated with malnutrition included being a male child, being between 3 and 24 months of age and the presence of fever. In addition, several authors reported a high rate of infectious diseases, including parasitic infections that cause diarrhoea, cholera, schistosomiasis, malaria and sexually transmitted infections among internally displaced children 3, 44, 45.
In addition, the study observed a significant association between maternal BMI and displaced child’s nutritional status. A low maternal BMI was associated with child, stunting and wasting in this study. Similarly, the aprevious study reported that maternal stature was inversely associated with offspring mortality, underweight and stunting in infancy and childhood using 109 demographic and health surveys (DHS) in 54 low- to middle-income countries 46. Another study also found that the child born to an underweight mother increased the risk of being stunted and underweight by 5 and 24%, respectively, compared with that born from a healthy-BMI mother in Bangladesh 47.
Improved diet and healthcare for women before and during pregnancy and lactation would significantly reduce child undernutrition. Low maternal BMI leading to child undernutrition could be due to poor diet.
The high prevalence of malnutrition observed in the present study calls for comprehensive public health intervention measures. The nutrition studies reviewed indicate that community interventions, including incentive-based nutrition education, do not improve growth and nutrition for internally displaced children; however, the presence of aid agencies and the ability of families to connect with host communities appear to improve nutritional outcomes 48, 49. A comprehensive health education programme with emphasis on good nutrition (targeting displaced children and their parents) should be carried out.
The strength of our study is that it was carried out in a displaced population and non-displaced with high background rate of malnutrition and risk of mortality. Further, the study was conducted prospectively with anthropometric measurements being taken by a trained resident. As a limitation, this study did not include household wealth index and biochemical data to assess dietary deficiencies in children, which could be considered in future study.
The study revealed that the nutritional status of the children studied is critical. Overall, the prevalence of acute malnutrition, stunting and underweight are above WHO alert thresholds. It is observed that underweight and stunting were more accentuated among displaced children with prevalence exceeding the alert thresholds while wasting was more frequent among non-displaced children with prevalence above the threshold of WHO emergency (15%). Among displaced children, the 36 to 59 months age group was most affected by stunting with prevalence above the WHO emergency threshold (40%).
Based on these findings, interventions should be focused on child health promotion and prevention, improvement of household WASH and food security, including mother’s awareness regarding health nutritional care of children < 5 years. New policies in nutritional intervention, particularly for mother with low BMI and children who have low birth weight, current diseases such as diarrhea, fever and ARI, should be implemented by the government to improve health and nutritional status of children < 5 years in Burkina Faso.
IDPs: Internally Displaced Persons; ENA: Emergency Nutrition Assessment; SMART: Standardized monitoring and assessment on relief and transitions; STATA: Statistical Software for Data Science; ODK: Open Data Kit; DHS: Demographic and Health Surveys; WASH: Water Sanitation and Hygiene; WHO: World Health Organization; BMI: Body Mass Index; ARI: Acute Respiratory Infections; SD: Standard Deviation, HAZ: Height for Age Z-score; WAZ: Weight for Age Z-score; WHZ: Weight for Height Z-score; OR: Odds Ratio; CI: Confidence Interval; COR: Crude OR; AOR: Adjusted OR; BW: Birth Weight
The authors unanimously agree that the information in this manuscript will be taken into account by your journal for publication and confirm that the results of this manuscript have not been published elsewhere, nor that they are in progress review by another editor.
The authors declare no conflict of interest.
SB drafted the initial manuscript and analyzed and interpreted the results. FHB conceptualized the study and was a major contributor to writing the manuscript. FG performed the statistical analysis and, AS is the main supervisor of the work. All authors read and approved the final manuscript.
We thank Mcknight Fundation for the financial study and the health centers in the North Central Region for their contribution to the study
| [1] | Internal Displacement Monitoring Center, 2019. Internal displacement. Geneva;. | ||
| In article | |||
| [2] | Internal Displacement Monitoring Center, 2019. Global report on internal displacement. Geneva.. | ||
| In article | |||
| [3] | United Nations, Guiding principles on internal displacement United Nations; 1998. | ||
| In article | |||
| [4] | Salami B, Iwuagwu S, Amodu O, Tulli M, Ndikom C, Gommaa H, Lavin T, Kariwo M: 2020. The health of internally displaced children in sub-Saharan Africa: a scoping review. BMJ Glob Health, 5. | ||
| In article | View Article PubMed | ||
| [5] | Statistiques de poche sur la santé pour les décideurs. 2020. Ministère de la santé.Burkina Faso;. | ||
| In article | |||
| [6] | Enquête nutritionnelle nationale SMART. 2018. Ministère de la santé, Burkina Faso. | ||
| In article | |||
| [7] | Rapport. “L’incidence sociale et économique de la sous-nutrition chez l’enfant au Burkina Faso”. 2012, Programme Alimentaire Mondial PAM. | ||
| In article | |||
| [8] | Enquête nutritionnelle dans les communautés et sites d’accueil des personnes déplacées internes selon la méthodologie Rapid SMART 2019. Ministère de la santé, Burkina Faso. | ||
| In article | |||
| [9] | Rapport sur la situation des personnes déplacées internes. Burkina Faso; 2019. Office for the Coordination of Humanitarian Affairs. | ||
| In article | |||
| [10] | Enquête Modulaire Demographie et Santé. 2015. Institut National de la Statistique et de la Démographie, Burkina Faso; | ||
| In article | |||
| [11] | Rapport national bilan annuel 2020. Programme national d’approvisionnement en eau potable (pn-aep).Ministère de l'Eau et de l'Assainissement, | ||
| In article | |||
| [12] | Programme national d'assainissement des eaux usées et excréta, bilan national 2020. Ministère de l'Eau et de l'Assainissement, | ||
| In article | |||
| [13] | Enquête Multisectorielle Continue. Burkina Faso; 2015. Profil de pauvreté et d’inégalités. Institut National de la Statistique et de la Démographie. | ||
| In article | |||
| [14] | Projections démographiques des communes.; 2017. Institut National de la Statistique et de la Démographie, Burkina Faso | ||
| In article | |||
| [15] | Institut National de la Statistique et de la Démographie, Projections démographiques des communes du Burkina Faso de 2014 à 2019. | ||
| In article | |||
| [16] | Réseau de prévention des crises alimentaires, Situation alimentaire et nutritionnelle au Burkina Faso. Cadre Harmonisé; 2019. | ||
| In article | |||
| [17] | Institut National de la Statistique et de la Démographie et Macro International. Enquête Démographique et de Santé (EDS-IV) et à Indicateurs Multiples (MICS) EDSBF-MICS IV. Rapport préliminaire. Burkina Faso; 2011. | ||
| In article | |||
| [18] | Uauy R, A.C., Kain J. Obesity trends in Latin America: transiting from under to overweight. J Nutr 2001; 131:893S-9S. | ||
| In article | View Article PubMed | ||
| [19] | Ministère de la santé. Enquête nutritionnelle dans les communautés et sites d’accueil des personnes déplacées internes au Burkina Faso selon la méthodologie Rapid SMART 2020. | ||
| In article | |||
| [20] | Geberselassie SB, Abebe SM, Melsew YA, Mutuku SM, Wassie MM: Prevalence of stunting and its associated factors among children 6-59 months of age in Libo-Kemekem district, Northwest Ethiopia; A community based cross sectional study. PLOS ONE 2018, 13:e0195361. | ||
| In article | View Article PubMed | ||
| [21] | Crooks DL, C.L., Gillett-Netting R. Migration following resettlement of the Gwembe Tonga of Zambia: the consequences for children's growth. Ecol Food Nutr 2008; 47: 363-81. | ||
| In article | View Article | ||
| [22] | Tumwine JK, B.W., Nutrition status of children in Kasese district at the Uganda-Congo border. East Afr Med J 2002;79: 427-34. | ||
| In article | View Article PubMed | ||
| [23] | Olofin I, McDonald CM, Ezzati M, Flaxman S, Black RE, Fawzi WW, Caulfield LE, Danaei G, for the Nutrition Impact Model S: Associations of Suboptimal Growth with All-Cause and Cause-Specific Mortality in Children under Five Years: A Pooled Analysis of Ten Prospective Studies. PLOS ONE 2013, 8:e64636. | ||
| In article | View Article PubMed | ||
| [24] | Ministère de l'Eau et de l'Assainissement. Enquête nationale sur l’accès des ménages aux ouvrages d’assainissement familial (ENA). Burkina Faso; 2010. | ||
| In article | |||
| [25] | WHO. WHO child growth standards, length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva. 2006. | ||
| In article | |||
| [26] | Bougma S, Garanet F, Sawadogo N, Savadogo A: Facteurs associés au retard de croissance dans un contexte de supplémentation alimentaire au Burkina Faso. Cahiers de Nutrition et de Diététique 2019. | ||
| In article | View Article | ||
| [27] | Dewey, K.G.H., M. G. Brown, K. H. Infant weight-for-length is positively associated with subsequent linear growth across four different populations. Matern Child Nutr .2005; 1(1): p. 11-20. | ||
| In article | View Article PubMed | ||
| [28] | Victora, C.G.d.O., M. Hallal, P. C. Worldwide timing of growth faltering: revisiting implications for interventions. Pediatrics. 2010; 125(3): p. e473-80. | ||
| In article | View Article PubMed | ||
| [29] | Ministère de la santé. Enquête nutritionnelle nationale SMART. Rapport final; 2016. | ||
| In article | |||
| [30] | Aurelius G, K.N., Truc DB, Ha TT, Lindgren G, Height, weight, and body mass index (BMI) of Vietnamese (Hanoi) schoolchildren aged 7-11 years related to parents' occupation and education. J Trop Pediatr. 1996 Feb; 42(1): 21-6. PMID: 8820616. | ||
| In article | View Article PubMed | ||
| [31] | Admassu B, Ritz C, Wells JCK, Girma T, Andersen GS, Belachew T, Owino V, Michaelsen KF, Abera M, Wibaek R, et al: Accretion of Fat-Free Mass Rather Than Fat Mass in Infancy Is Positively Associated with Linear Growth in Childhood. J Nutr 2018, 148:607-615. | ||
| In article | View Article PubMed | ||
| [32] | Park H, Park K, Kim MH, Kim GS, Chung S: Gender differences in relationship between fat-free mass index and fat mass index among Korean children using body composition chart. Yonsei Med J 2011, 52:948-952. | ||
| In article | View Article PubMed | ||
| [33] | Myatt, M.K., T. Dolan, C. Improving screening for malnourished children at high risk of death: a study of children aged 6-59 months in rural Senegal. Public Health Nutr. 2019; 22(5): p. 862-871. | ||
| In article | View Article PubMed | ||
| [34] | Herrador Z, S.L., Gadisa E, Buño A, Gómez-Rioja R, Iturzaeta JM, de Armas LF, Benito A, Aseffa A, Moreno J, Cañavate C, Custodio E. Micronutrient deficiencies and related factors in school-aged children in Ethiopia: a cross-sectional study in Libo Kemkem and Fogera districts, Amhara Regional State. PLoS One. 2014 Dec 29;9(12):e112858. doi: 10.1371/journal.pone.0112858. PMID: 25546056; PMCID: PMC4278675. | ||
| In article | View Article PubMed | ||
| [35] | López-Perea N, Sordo L, Gadisa E, Cruz I, Hailu T, Moreno J, Aseffa A, Cañavate C, Custodio E: Knowledge, Attitudes and Practices Related to Visceral Leishmaniasis in Rural Communities of Amhara State: A Longitudinal Study in Northwest Ethiopia. PLOS Neglected Tropical Diseases 2014, 8:e2799. | ||
| In article | View Article PubMed | ||
| [36] | Rahman MS, Howlader T, Masud MS, Rahman ML: Association of Low-Birth Weight with Malnutrition in Children under Five Years in Bangladesh: Do Mother's Education, Socio-Economic Status, and Birth Interval Matter? PloS one 2016, 11:e0157814-e0157814. | ||
| In article | View Article PubMed | ||
| [37] | Rodríguez L, C.E., Ortiz R. , Malnutrition and gastrointestinal and respiratory infections in children: a public health problem. Int J Environ Res Public Health 2011; 8: 1174-205. | ||
| In article | View Article PubMed | ||
| [38] | Rytter MJ, Kolte L, Briend A, Friis H, Christensen VB: The immune system in children with malnutrition--a systematic review. PLoS One 2014, 9:e105017. | ||
| In article | View Article PubMed | ||
| [39] | MB., K., Interaction of nutrition and infections globally: an overview. Ann Nutr Metab 2012; 61: 39-45. | ||
| In article | View Article PubMed | ||
| [40] | Doherty T, Zembe W, Ngandu N, Kinney M, Manda S, Besada D, Jackson D, Daniels K, Rohde S, van Damme W, et al: Assessment of Malawi's success in child mortality reduction through the lens of the Catalytic Initiative Integrated Health Systems Strengthening programme: Retrospective evaluation. J Glob Health 2015, 5:020412. | ||
| In article | View Article PubMed | ||
| [41] | Tawfiq E, Alawi SAS, Natiq K: Effects of Training Health Workers in Integrated Management of Childhood Illness on Quality of Care for Under-5 Children in Primary Healthcare Facilities in Afghanistan. Int J Health Policy Manag 2020, 9: 17-26. | ||
| In article | View Article PubMed | ||
| [42] | Kjærgaard J, Anastasaki M, Stubbe Østergaard M, Isaeva E, Akylbekov A, Nguyen NQ, Reventlow S, Lionis C, Sooronbaev T, Pham LA, et al: Diagnosis and treatment of acute respiratory illness in children under five in primary care in low-, middle-, and high-income countries: A descriptive FRESH AIR study. PLOS ONE 2019, 14:e0221389. | ||
| In article | View Article PubMed | ||
| [43] | Owoaje ET, Uchendu OC, Ajayi TO, Cadmus EO: A review of the health problems of the internally displaced persons in Africa. Niger Postgrad Med J 2016, 23:161-171. | ||
| In article | View Article PubMed | ||
| [44] | Ito EE, E.A., Schistosomiasis: the aftermath of 2012 floods in delta state, southern Nigeria. International Medical Journal 2015; 22: 218-23. | ||
| In article | |||
| [45] | Iyer AS, Bouhenia M, Rumunu J, Abubakar A, Gruninger RJ, Pita J, Lino RL, Deng LL, Wamala JF, Ryan ET, et al: Immune Responses to an Oral Cholera Vaccine in Internally Displaced Persons in South Sudan. Sci Rep 2016, 6: 35742. | ||
| In article | View Article PubMed | ||
| [46] | Ozaltin E, H.K., Subramanian SV. , Association of maternal stature with offspring mortality, underweight, and stunting in low- to middle-income countries. J Am Med Assoc 2010; 303: 1507–16. | ||
| In article | View Article PubMed | ||
| [47] | Hasan MT, Soares Magalhães RJ, Williams GM, Mamun AA: Long-term changes in childhood malnutrition are associated with long-term changes in maternal BMI: evidence from Bangladesh, 1996-2011. Am J Clin Nutr 2016, 104:1121-1127. | ||
| In article | View Article PubMed | ||
| [48] | Porignon D, Katulanya I, Elongo L, Ntalemwa N, Tonglet R, Dramaix M, Hennart P: The unseen face of humanitarian crisis in eastern Democratic Republic of Congo: was nutritional relief properly targeted? J Epidemiol Community Health 2000, 54:6-9. | ||
| In article | View Article PubMed | ||
| [49] | Glew RH, B.R., VanderJagt DJ. Effects of displacement resulting from ethnic/religious conflict on the growth and body composition of Fulani children in northern Nigeria. J Trop Pediatr 2003; 49: 279-85. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2022 Sibiri Bougma, Fatoumata Hama-Ba, Franck Garanet and Aly Savadogo
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Internal Displacement Monitoring Center, 2019. Internal displacement. Geneva;. | ||
| In article | |||
| [2] | Internal Displacement Monitoring Center, 2019. Global report on internal displacement. Geneva.. | ||
| In article | |||
| [3] | United Nations, Guiding principles on internal displacement United Nations; 1998. | ||
| In article | |||
| [4] | Salami B, Iwuagwu S, Amodu O, Tulli M, Ndikom C, Gommaa H, Lavin T, Kariwo M: 2020. The health of internally displaced children in sub-Saharan Africa: a scoping review. BMJ Glob Health, 5. | ||
| In article | View Article PubMed | ||
| [5] | Statistiques de poche sur la santé pour les décideurs. 2020. Ministère de la santé.Burkina Faso;. | ||
| In article | |||
| [6] | Enquête nutritionnelle nationale SMART. 2018. Ministère de la santé, Burkina Faso. | ||
| In article | |||
| [7] | Rapport. “L’incidence sociale et économique de la sous-nutrition chez l’enfant au Burkina Faso”. 2012, Programme Alimentaire Mondial PAM. | ||
| In article | |||
| [8] | Enquête nutritionnelle dans les communautés et sites d’accueil des personnes déplacées internes selon la méthodologie Rapid SMART 2019. Ministère de la santé, Burkina Faso. | ||
| In article | |||
| [9] | Rapport sur la situation des personnes déplacées internes. Burkina Faso; 2019. Office for the Coordination of Humanitarian Affairs. | ||
| In article | |||
| [10] | Enquête Modulaire Demographie et Santé. 2015. Institut National de la Statistique et de la Démographie, Burkina Faso; | ||
| In article | |||
| [11] | Rapport national bilan annuel 2020. Programme national d’approvisionnement en eau potable (pn-aep).Ministère de l'Eau et de l'Assainissement, | ||
| In article | |||
| [12] | Programme national d'assainissement des eaux usées et excréta, bilan national 2020. Ministère de l'Eau et de l'Assainissement, | ||
| In article | |||
| [13] | Enquête Multisectorielle Continue. Burkina Faso; 2015. Profil de pauvreté et d’inégalités. Institut National de la Statistique et de la Démographie. | ||
| In article | |||
| [14] | Projections démographiques des communes.; 2017. Institut National de la Statistique et de la Démographie, Burkina Faso | ||
| In article | |||
| [15] | Institut National de la Statistique et de la Démographie, Projections démographiques des communes du Burkina Faso de 2014 à 2019. | ||
| In article | |||
| [16] | Réseau de prévention des crises alimentaires, Situation alimentaire et nutritionnelle au Burkina Faso. Cadre Harmonisé; 2019. | ||
| In article | |||
| [17] | Institut National de la Statistique et de la Démographie et Macro International. Enquête Démographique et de Santé (EDS-IV) et à Indicateurs Multiples (MICS) EDSBF-MICS IV. Rapport préliminaire. Burkina Faso; 2011. | ||
| In article | |||
| [18] | Uauy R, A.C., Kain J. Obesity trends in Latin America: transiting from under to overweight. J Nutr 2001; 131:893S-9S. | ||
| In article | View Article PubMed | ||
| [19] | Ministère de la santé. Enquête nutritionnelle dans les communautés et sites d’accueil des personnes déplacées internes au Burkina Faso selon la méthodologie Rapid SMART 2020. | ||
| In article | |||
| [20] | Geberselassie SB, Abebe SM, Melsew YA, Mutuku SM, Wassie MM: Prevalence of stunting and its associated factors among children 6-59 months of age in Libo-Kemekem district, Northwest Ethiopia; A community based cross sectional study. PLOS ONE 2018, 13:e0195361. | ||
| In article | View Article PubMed | ||
| [21] | Crooks DL, C.L., Gillett-Netting R. Migration following resettlement of the Gwembe Tonga of Zambia: the consequences for children's growth. Ecol Food Nutr 2008; 47: 363-81. | ||
| In article | View Article | ||
| [22] | Tumwine JK, B.W., Nutrition status of children in Kasese district at the Uganda-Congo border. East Afr Med J 2002;79: 427-34. | ||
| In article | View Article PubMed | ||
| [23] | Olofin I, McDonald CM, Ezzati M, Flaxman S, Black RE, Fawzi WW, Caulfield LE, Danaei G, for the Nutrition Impact Model S: Associations of Suboptimal Growth with All-Cause and Cause-Specific Mortality in Children under Five Years: A Pooled Analysis of Ten Prospective Studies. PLOS ONE 2013, 8:e64636. | ||
| In article | View Article PubMed | ||
| [24] | Ministère de l'Eau et de l'Assainissement. Enquête nationale sur l’accès des ménages aux ouvrages d’assainissement familial (ENA). Burkina Faso; 2010. | ||
| In article | |||
| [25] | WHO. WHO child growth standards, length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva. 2006. | ||
| In article | |||
| [26] | Bougma S, Garanet F, Sawadogo N, Savadogo A: Facteurs associés au retard de croissance dans un contexte de supplémentation alimentaire au Burkina Faso. Cahiers de Nutrition et de Diététique 2019. | ||
| In article | View Article | ||
| [27] | Dewey, K.G.H., M. G. Brown, K. H. Infant weight-for-length is positively associated with subsequent linear growth across four different populations. Matern Child Nutr .2005; 1(1): p. 11-20. | ||
| In article | View Article PubMed | ||
| [28] | Victora, C.G.d.O., M. Hallal, P. C. Worldwide timing of growth faltering: revisiting implications for interventions. Pediatrics. 2010; 125(3): p. e473-80. | ||
| In article | View Article PubMed | ||
| [29] | Ministère de la santé. Enquête nutritionnelle nationale SMART. Rapport final; 2016. | ||
| In article | |||
| [30] | Aurelius G, K.N., Truc DB, Ha TT, Lindgren G, Height, weight, and body mass index (BMI) of Vietnamese (Hanoi) schoolchildren aged 7-11 years related to parents' occupation and education. J Trop Pediatr. 1996 Feb; 42(1): 21-6. PMID: 8820616. | ||
| In article | View Article PubMed | ||
| [31] | Admassu B, Ritz C, Wells JCK, Girma T, Andersen GS, Belachew T, Owino V, Michaelsen KF, Abera M, Wibaek R, et al: Accretion of Fat-Free Mass Rather Than Fat Mass in Infancy Is Positively Associated with Linear Growth in Childhood. J Nutr 2018, 148:607-615. | ||
| In article | View Article PubMed | ||
| [32] | Park H, Park K, Kim MH, Kim GS, Chung S: Gender differences in relationship between fat-free mass index and fat mass index among Korean children using body composition chart. Yonsei Med J 2011, 52:948-952. | ||
| In article | View Article PubMed | ||
| [33] | Myatt, M.K., T. Dolan, C. Improving screening for malnourished children at high risk of death: a study of children aged 6-59 months in rural Senegal. Public Health Nutr. 2019; 22(5): p. 862-871. | ||
| In article | View Article PubMed | ||
| [34] | Herrador Z, S.L., Gadisa E, Buño A, Gómez-Rioja R, Iturzaeta JM, de Armas LF, Benito A, Aseffa A, Moreno J, Cañavate C, Custodio E. Micronutrient deficiencies and related factors in school-aged children in Ethiopia: a cross-sectional study in Libo Kemkem and Fogera districts, Amhara Regional State. PLoS One. 2014 Dec 29;9(12):e112858. doi: 10.1371/journal.pone.0112858. PMID: 25546056; PMCID: PMC4278675. | ||
| In article | View Article PubMed | ||
| [35] | López-Perea N, Sordo L, Gadisa E, Cruz I, Hailu T, Moreno J, Aseffa A, Cañavate C, Custodio E: Knowledge, Attitudes and Practices Related to Visceral Leishmaniasis in Rural Communities of Amhara State: A Longitudinal Study in Northwest Ethiopia. PLOS Neglected Tropical Diseases 2014, 8:e2799. | ||
| In article | View Article PubMed | ||
| [36] | Rahman MS, Howlader T, Masud MS, Rahman ML: Association of Low-Birth Weight with Malnutrition in Children under Five Years in Bangladesh: Do Mother's Education, Socio-Economic Status, and Birth Interval Matter? PloS one 2016, 11:e0157814-e0157814. | ||
| In article | View Article PubMed | ||
| [37] | Rodríguez L, C.E., Ortiz R. , Malnutrition and gastrointestinal and respiratory infections in children: a public health problem. Int J Environ Res Public Health 2011; 8: 1174-205. | ||
| In article | View Article PubMed | ||
| [38] | Rytter MJ, Kolte L, Briend A, Friis H, Christensen VB: The immune system in children with malnutrition--a systematic review. PLoS One 2014, 9:e105017. | ||
| In article | View Article PubMed | ||
| [39] | MB., K., Interaction of nutrition and infections globally: an overview. Ann Nutr Metab 2012; 61: 39-45. | ||
| In article | View Article PubMed | ||
| [40] | Doherty T, Zembe W, Ngandu N, Kinney M, Manda S, Besada D, Jackson D, Daniels K, Rohde S, van Damme W, et al: Assessment of Malawi's success in child mortality reduction through the lens of the Catalytic Initiative Integrated Health Systems Strengthening programme: Retrospective evaluation. J Glob Health 2015, 5:020412. | ||
| In article | View Article PubMed | ||
| [41] | Tawfiq E, Alawi SAS, Natiq K: Effects of Training Health Workers in Integrated Management of Childhood Illness on Quality of Care for Under-5 Children in Primary Healthcare Facilities in Afghanistan. Int J Health Policy Manag 2020, 9: 17-26. | ||
| In article | View Article PubMed | ||
| [42] | Kjærgaard J, Anastasaki M, Stubbe Østergaard M, Isaeva E, Akylbekov A, Nguyen NQ, Reventlow S, Lionis C, Sooronbaev T, Pham LA, et al: Diagnosis and treatment of acute respiratory illness in children under five in primary care in low-, middle-, and high-income countries: A descriptive FRESH AIR study. PLOS ONE 2019, 14:e0221389. | ||
| In article | View Article PubMed | ||
| [43] | Owoaje ET, Uchendu OC, Ajayi TO, Cadmus EO: A review of the health problems of the internally displaced persons in Africa. Niger Postgrad Med J 2016, 23:161-171. | ||
| In article | View Article PubMed | ||
| [44] | Ito EE, E.A., Schistosomiasis: the aftermath of 2012 floods in delta state, southern Nigeria. International Medical Journal 2015; 22: 218-23. | ||
| In article | |||
| [45] | Iyer AS, Bouhenia M, Rumunu J, Abubakar A, Gruninger RJ, Pita J, Lino RL, Deng LL, Wamala JF, Ryan ET, et al: Immune Responses to an Oral Cholera Vaccine in Internally Displaced Persons in South Sudan. Sci Rep 2016, 6: 35742. | ||
| In article | View Article PubMed | ||
| [46] | Ozaltin E, H.K., Subramanian SV. , Association of maternal stature with offspring mortality, underweight, and stunting in low- to middle-income countries. J Am Med Assoc 2010; 303: 1507–16. | ||
| In article | View Article PubMed | ||
| [47] | Hasan MT, Soares Magalhães RJ, Williams GM, Mamun AA: Long-term changes in childhood malnutrition are associated with long-term changes in maternal BMI: evidence from Bangladesh, 1996-2011. Am J Clin Nutr 2016, 104:1121-1127. | ||
| In article | View Article PubMed | ||
| [48] | Porignon D, Katulanya I, Elongo L, Ntalemwa N, Tonglet R, Dramaix M, Hennart P: The unseen face of humanitarian crisis in eastern Democratic Republic of Congo: was nutritional relief properly targeted? J Epidemiol Community Health 2000, 54:6-9. | ||
| In article | View Article PubMed | ||
| [49] | Glew RH, B.R., VanderJagt DJ. Effects of displacement resulting from ethnic/religious conflict on the growth and body composition of Fulani children in northern Nigeria. J Trop Pediatr 2003; 49: 279-85. | ||
| In article | View Article PubMed | ||