 sciepub.com
sciepub.com
 Quick Submission
Quick Submission

Diagnostic Utility of 18F-FDG PECT/CT in Assessment of Post-therapy Remission or Relapse of Lymphoma
Nagham Nabil Omar1, Mostafa Shaker Abolela2, Marwa I. Abdelgawad3, , Abeer Ibrahim4, Amr F. Mourad5, Khalid Rezk6
, Abeer Ibrahim4, Amr F. Mourad5, Khalid Rezk6
1Radiology Department, Assuit University, Egypt
2Radiology Department, Nasser Institute Hospital
3Clinical Oncology Department, Assiut University, Egypt
4Medical Oncology Department, South Egypt Cancer Inistitute
5Radiodiagnosis Department, South Egypt Cancer Inistitute
6Surgical Oncology Department, South Egypt Cancer Inistitute
Abstract
Background: Treatment and prognosis of lymphoma depend on accurate staging and evaluation. Relapsed Lymphomas represent great problem in accurate quick diagnosis that imply appropriate treatment. Aim of the work: To evaluate diagnostic utility of 18F-FDG PECT/CT in assessment of treatment response and identification of disease relapse. Patients and Methods: This prospective study were conducted on 49 consecutive patients with histologically verified lymphoma. They were 27/49 (55.1%) male and 22/49 (44.9%) female aged 37.83±2.29. All patients were subjected to pretreatment as well a follow up clinical, laboratory, CT PET-CT. PET-CT findings were classified as positive and negative according to remission status and relapse. The sensitivity, specificity and accuracy of PET- CT in assessment of the remission status and relapse were calculated and to be confirmed by open or laparoscopic biopsy. Results: PET-CT detected complete regression in 28 patients (57.14%), partial regression in 4 patients (8.16%), stationary course in 2 patients (4.08%), progression / relapse in 15 patients (30.61%). According to PET/CT 9 (23%) patients were true positive, 25 (65%) were true negative and 5 (13%) were false negative with sensitivity, specificity, positive p predictive value and negative predictive value of 95% and 91%, 90% and 98%, respectively. Conclusion: Our results confirm FDG-PET as a valid tool for assessment of treatment response and detection of relapsing lymphoma. We recommended further multicentric prospective studies that incorporates a larger number of patients should be implemented to define the exact relation between certain clinical, pathological, laboratory and PET factors and fate of the disease.
Keywords: 18F-FDG PECT/CT, lymphoma, CT, Treatment, Relapsed Lymphoma
Copyright © 2016 Science and Education Publishing. All Rights Reserved.Cite this article:
- Nagham Nabil Omar, Mostafa Shaker Abolela, Marwa I. Abdelgawad, Abeer Ibrahim, Amr F. Mourad, Khalid Rezk. Diagnostic Utility of 18F-FDG PECT/CT in Assessment of Post-therapy Remission or Relapse of Lymphoma. Journal of Cancer Research and Treatment. Vol. 4, No. 5, 2016, pp 88-95. http://pubs.sciepub.com/jcrt/4/5/3
- Omar, Nagham Nabil, et al. "Diagnostic Utility of 18F-FDG PECT/CT in Assessment of Post-therapy Remission or Relapse of Lymphoma." Journal of Cancer Research and Treatment 4.5 (2016): 88-95.
- Omar, N. N. , Abolela, M. S. , Abdelgawad, M. I. , Ibrahim, A. , Mourad, A. F. , & Rezk, K. (2016). Diagnostic Utility of 18F-FDG PECT/CT in Assessment of Post-therapy Remission or Relapse of Lymphoma. Journal of Cancer Research and Treatment, 4(5), 88-95.
- Omar, Nagham Nabil, Mostafa Shaker Abolela, Marwa I. Abdelgawad, Abeer Ibrahim, Amr F. Mourad, and Khalid Rezk. "Diagnostic Utility of 18F-FDG PECT/CT in Assessment of Post-therapy Remission or Relapse of Lymphoma." Journal of Cancer Research and Treatment 4, no. 5 (2016): 88-95.
| Import into BibTeX | Import into EndNote | Import into RefMan | Import into RefWorks |
At a glance: Figures
1. Introduction
Lymphoma is the most common primary hematopoietic malignancy [1] It accounts for approximately 8% of all adult malignancies and 10–15% of all pediatric cancers, malignancies [1, 2]. It is broadly divided into Hodgkin‘s and non- Hodgkin‘s lymphoma, however in fact lymphomas are a heterogeneous group of diseases [1, 2, 3].
Many lymphomas are potentially curable when treated with chemotherapy alone or in combination with radiation therapy, however up to 20% of patients have primary refractory disease and an additional 20% will relapse following frontline treatment [2, 4]. Treatment and prognosis of lymphoma depend on accurate staging and evaluation which have been made in diagnosis and treatment [4, 5].
Diagnostic imaging provides important information for staging and response assessment in patients with lymphoma with the potential to improve disease characterization and treatment selection [4, 5, 6, 7, 8]. It provides advances in staging and response assessment of lymphomas which occurred with the introduction of prognostic indices CT, MRI. [4, 5] However, in up to 64% of computed tomography (CT) or magnetic resonance imaging (MRI) show remaining tumor masses after completed treatment, although only a few of these patients will eventually relapse. These masses may represent fibrotic tissue or even an active Hodgkin tumor [4-9][4].
In recent years, positron emission tomography (PET) with 2-[fluorine-18] fluoro-2-deoxy-dglucose (FDG) has become an established imaging method for the evaluation of lymphoma patients [9, 10]. It has gained a role in the staging and follow-up of lymphomas. Not every abnormal 18F-FDG PET/CT imaging implicates malignancy. Tuberculosis, inflammation, infection or granulomatous diseases are consistent with False-positive PET/CT.
Therby, attention should be paid to the positive PET/CT imaging interpretation. PET-CT response can be used to guide therapy to improve patient outcomes and increased the diagnostic sensitivity and specificity of lymphoma [4, 5, 8, 9, 10].
By assessing metabolic activity within a node, PET is not directly reliant on nodal size to determine the presence or absence of malignancy [9, 10]. Nodes that are not enlarged can be shown to contain tumor on FDG-PET images, and nodes that are enlarged can be shown to be reactive in nature [5, 8]. For this reason, PET has been shown to be more sensitive and specific than CT for identification of sites of disease. Studies have shown that FDG PET may be superior to computed tomography (CT), gallium- 67 scintigraphy, and bone scintigraphy in the staging and treatment evaluation of lymphoma because of good spatial resolution and the functionality of FDG PET scans [11, 12]. (Figure 1)
 Download as
Download as

2. Patients and Methods
2.1. Study PopulationDuring the period between April 2013 and August July 2015, this prospective study were conducted on 49 consecutive patients with histologically verified lymphoma. They were 27/49 (55.1%) male and 22/49 (44.9%) female aged 37.83±2.29 All patients were subjected to clinical examination and staging according to the Ann Arbor classification, chest X-ray and laboratory testing for lymphoma including LDH, ESR and CBC as well as pretreatment baseline contrast enhanced CT (CECT) and PET- CT. For follow up of remission status ad detection of relapse, all included patients were subjected to regular history, clinical examination, laboratory testing, contrast enhanced CT (CECT) and PET- CT, every 3-6 months after completion of chemotherapy and /or radiotherapy. The median follow up period was 14 month. Histopathological diagnosis was established in all cases in the initial study and follow up in cases with suspected disease relapse by means of surgical open, laparoscopic or image guided biopsy. Five patients were excluded from this study, 2 received previous chemotherapy and radiotherapy, 2 underwent previous surgery related to their lymphoma and one patient with uncontrolled diabetes. This study was approved by the ethical committee of our institutions.
2.2. FDG PET Technique and Image ProcessingAll examinations were done and data were obtained using GE Discovery 690 PET/CT scanner as well as Siemens Bio-graph true point PET/CT scanner. Prior to the examination, all patients were asked to fast for six hours, empty their bladders, remove metallic items, avoid any kind of strenuous activity, and administrate one liter of negative oral contrast agent (5% mannitol) one hour before the exam. An I.V. cannula was inserted in the patient‘s arm for administration of 3-7 MBq/Kg of 18F-FDG 45-90 minutes before examination. Then the patients were instructed to rest in a quiet room, devoid of distractions, and they were also asked to keep their movements, including talking, at an absolute minimum.
The patients were positioned in a comfortable head fixation with arms up. was performed following injection of 125 mL of a low- osmolarity iodinated contrast medium at a rate of 4 m /sec using a power injector. For a typical whole body PET -CT study (neck, chest, abdomen, and pelvis), scanning began at the level of the skull base and extended caudally to the upper thighs. The study was performed with the patient breathing quietly. Scanning parameters are collimation width of 5.0 mm, pitch of 1.5, and gantry rotation time of 0.8 second and field of view of 50cm. The helical data are retrospectively reconstructed at 1mm intervals. Forty-seven overlapping slices per bed position were acquired with a full width of 6.0 mm at half-maximal resolution and approximately 5.0-mm slice thickness with a 3.75 mm center-to-center distance in the axial direction. For PET/CT Fusion hundreds of trans-axial PET and CT images were first reconstructed, then reformatted into coronal and sagittal images to facilitate image interpretation. For each of these sets of PET and CT images, corresponding fusion images, combining the two types of data, also were generated. The whole acquisition time for an integrated PET/ CT scan was approximately 25-30 minutes. PET image data sets were reconstructed using CT data for attenuation correction and co-registered images were displayed using special software.
2.3. Surgical InterferenceEither open excisional or incisional lymph node biopsy, splenectomy or laparoscopic biopsy from inraabdominal relapsing lesion which highly suspicious by PET-CT scan to be confirm diagnosis and evaluate sensitivity of PET CT scan in diagnosis.
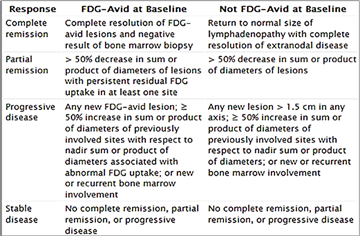
2.4. Image AnalysisAll PET/CT examinations were analyzed by a consensus of two experienced observers of nuclear medicine physicians and radiologists in a blind fashion. Firstly pretreatment baseline PET/CT were evaluated, followed by analysis of the follow up PET images and the volume of CT scans for evaluation of remission status or the presence and extent of 18F-FDG- positive lymphoma in different lymph nodes groups and the presence of extra- nodal sites for residual/recurrent abnormalities. Abnormal 18F-FDG uptake was defined as radiotracer accumulation outside the normal anatomic structures and of greater intensity than background activity, excluding normal areas of physiological uptake. In all cases estimation of 18- FDG uptake was done using SUVmax values for each group of enlarged nodes or mass lesion and comparison of values was done in the follow up studies respecting the ROI position as much as possible. Visual assessment was used as a secondary method for interpreting PET findings as positive or negative. According to the IHP definitions (Figure 1) , residual masses of 2 cm or more in greatest transverse diameter (GTD) with 18F-FDG activity visually exceeding that of mediastinal blood pool structures are considered PET positive, whereas residual masses 1.1 to 1.9 cm are considered PET positive only if their activity exceeds surrounding background activity. A smaller residual mass or a normal-sized lymph node (e.g., <1 × 1 cm) should be considered positive for disease if its activity is higher than that of the surrounding background. If there was a clearly multifocal increase in FDG uptake in the bone marrow, the patient was considered as PET positive excluding cases where there is diffuse pattern of uptake of reactive bone marrow hyperplasia after chemotherapy. In the liver and spleen, focal or diffuse FDG uptake with activity greater than that in surrounding liver or spleen parenchyma are considered PET/CT positive keeping in mind the absence of other confounding factors, such as physiologic hyperplasia after cytokine administration. The presence of single or multiple foci of clearly elevated FDG uptake within the bone marrow also is considered positive for PET/CT positive. Complete response (CR) was defined as disappearance of all detectable disease or lymph nodes >1.5 cm must decrease to ≤1.5 cm. Partial response (PR) was defined as more than 50% in SPD. Stationary (SD) was defined as less than 50% decrease in SPD. Progressive disease (PD)/relapse was defined as new lesion or SPD increase >50% from nadir of any lymph node.
2.5. Standard of ReferencesThe final diagnosis for PET/CT findings was made by correlation with clinical, laboratory, and other imaging modalities in addition to follow up for at least 6 months. The final diagnosis of relapse was made by histo-pathological analysis together with follow up for at least 6 months.
2.6.Statistical AnalysisThe PET/CT finding was classified as true positive, false positive, true negative and false negative according to the final diagnosis based on previously mentioned stranded of reference. The sensitivity, specificity, positive predictive value (PPV), negative (NPV),and accuracy were calculated by patients. Data were statistically described in terms of range, mean standard deviation (SD), median, frequencies (number of cases) and percentages when appropriate. P values less than 0.05 was considered statistically significant. All statistical calculations were done using computer programs Microsoft Excel 2010 (Microsoft Corporation, NY, USA) and SPSS (Statistical Package for the Social Science; SPSS Inc., ) version 15 for Microsoft Windows.
3. Results
Characteristics of the 49 eligible lymphoma patients are presented in Table 1 and included They were 27/49 (55.1%) male and 22/49 (44.9%) female aged 37.83±2.29. The median follow up period was 22.4 months. (Table 1)







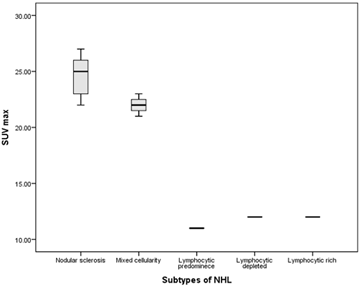
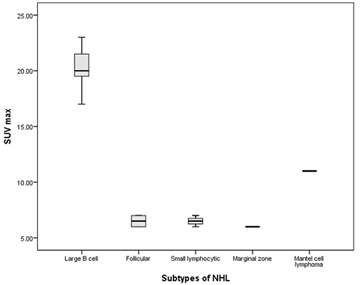
Pretreatment base line PET/CT depicted 4 cases in stage I, 10 cases in stage II, 10 cases in stage III, 25 cases in stage VI. Most subtypes of HD shows high SUV max, while in NHL B cell lymphoma shows high SUV max in nearly total cases recording in contrast to indolent follicular and marginal zone Table 2, Figure 2, Figure 3.





 Download as
Download as
 Download as
Download as
During follow-up of 12 months,PET-CT detected complete regression in 28 patients (57.14%), partial regression in 4 patients (8.16%), stationary course in 2 patients (4.08%), progression/relapse in 15 patients (30.61%). CT guided biopsy was performed in the latter patients and confirmed the initial subtype of lymphoma. (Table 3)




Sixty Five percent (65%) were PET/CT negative and all of them were disease free at a median period of 12 months. All were true positive and non of them were relapsed, PET/CT exclude active disease and free extra-nodal sites in all of them. (34 %) patients had a positive PET/CT scan, (54%) showed positive PET/CT nodal relapse and (31 %) showed positive PET/CT scan in nodal and extranodal relapse. Unfortunately 1 patient had combined nodal and hepatic relapse, 2 had diffuse splenic infiltration and 1 patient showed bone marrow infiltration. Three relapsed patients showed partial remission after high-dose chemotherapy, 2 showed progressive course, 3 patients died due to progressive disease, and 5 were currently subjected to palliative treatment. In the 13 positive PET/CT patients 4/13 (31%) had false positive results, 1 related to inflammatory uptake, 1 had post-therapy thymus hyperplasia, and remaining 2 had non specific uptake in digestive tract, which mimic tumor relapse. The sensitivity, specificity, positive p predictive value and negative predictive value of 95% and 91%, 90% and 98%, respectively. (Table 4, Figure 4-Figure 6)




 Download as
Download as
 Download as
Download as
 Download as
Download as
 Download as
Download as
4. Discussion
Despite attempts to increase the efficacy of conventional chemotherapy, less than 50% of high-grade lymphoma patients will experience prolonged disease-free survival and the remaining patients needs more intensive multidrug combinations and treatment intensification to improve outcome [1]. Outcome of malignant lymphomas which are a heterogeneous group of diseases = depend on accurate staging and early response to treatment [4]. The latter has been established as an important prognostic parameter in numerous malignancies and an important predictor of outcome, which has the advantage of guiding the management decision [6, 9].
Conventional methods for treatment response monitoring are based on morphologic criteria, and a reduction in tumor size on (MRI, CT, and ultrasound), is the most important determinant [6, 7, 8]. However, this is not an accurate predictor of outcome, possibly because the malignant cells in lymphoma make up only a small fraction of the tumor volume [6]. Furthermore, the shrinkage of the tumor takes time and thus can not form the basis for adjustment of therapy until late during treatment. Positron emission tomography (PET) is a non invasive, quantitative imaging technique that can visualize biochemical, physiological, and biologic processes invivo. It is the most specific and sensitive molecular imaging technique used to day [7, 8, 9, 10, 11].
Positron emission tomography (PET) with 2-[fluorine-18] fluoro-2- deoxy-d-glucose(FDG) may play an important role in only for diagnosis and staging but also for response assessment in lymphoma patients. Molecular imaging reflects the metabolic activity rather than the size of tissue masses [7, 9, 11]. Furthermore, metabolic changes during therapy tend to precede the anatomical changes and this allows for earlier and perhaps more effective changes of therapy [10, 11, 12, 13].
In the current study the aim was to assess the role of PET-CT is monitoring of remission status and relapse of lymphoma, Casasnovas RO et al [14] recommend PET-CT for mid treatment assessment in place of CT alone, if imaging is clinically indicated, and for remission assessment. Christian F. et al [15] concluded that early and late therapy response assessment by FDG-PET helps to identify patients with an excellent prognosis. Lavely WC et al , and Zinzani PL et al [16, 17] recommended the use of FDG-PET in hematologic malignancies for identification of disease extension, and response to the ongoing therapy, residual disease at therapy completion. Our study strongly supports the conclusions of previous studies.
In our study we used pretreatment PET/CT as a base line to which PET follow up evaluations were scored as negative or positive. Lin C at al [18], reported that baseline scans will decrease false positive results, as relapses typically occur in the region of previous disease seen on the baseline study.
In the current study, we used combining metabolic activity and anatomic size or volume to explored remission status. SUVmax values and international harmonization project criteria were used for assessment of response to therapy for each enlarged nodes or mass and comparison of values was done in the follow up studies respecting the ROI position as much as possible. This go on line with many studies Casasnovas RO et al, Wahl RL et al, , Boellaard R and Kostakoglu L et al [14, 19, 20, 21] who concluded that the use of measure proposed ported to improve response prediction volume containing the hottest area of tumor, is SUVpeak,a1-cm which may be less sensitive to noise and resolution and possibly more reproducible. Sally F. et al [22] recommended using visual ( quantitave) assessment of residual mass size and location should be recorded only at end of treatment. Casasnovas RO [14] et al reported that SUVmax at two and four cycles was predictive of treatment response, where as visual analysis was not. Others Yang DH et al and Fuertes S et al [23, 24] concluded that SUVmax predicts response, but with thresholds ranging from 66% to 91%. In our study inspite we used a blind fashion for data analysis we experienced that it remains necessary to integrate with clinical and laboratory information to exclude confounding variables.
In coordination with Hoffmann M eta al and Bishu S et al [25, 26], our study founded that most subtypes of HD showed high SUV max specially nodular sclerosis and mixed cellularity , in NHL cases we found that most cases of large B cell lymphoma shows high SUV value in contrast to indolent follicular and marginal zone lymphoma.
In our study, splenic and bone marrow infiltration were the main involved extranodal sites. Wu LM et al [27] concluded that PET/CT was a highly sensitive and specific modality in diagnosing patients with bone marrow involvement in lymphoma compared with MRI and PET alone.
In our study PET/CT were true positive in 9, true negative in 25 nd flase negative in 5 patients. The latter 1 related to inflammatory uptake, 1 had post-therapy thymus hyperplasia, and remaining 2 had non specific uptake in digestive tract, which mimic tumor relapse. According to Martin R et al [28] data, false positive FDG uptake seems to be a problem in HD patients. The characteristics of the patients with a false-positive result suggest a younger age. Jerusalem et al, Rhodes et al [29, 30] in an adult and pediatric groups respectively founded relatively similar PET CT false positive rustles. In contrast to these and or findings Zinzani PL et al [31] reported that the overall incidence of false-positive cases in their series is limited (16/1789 scans), differences in results are likely related to criteria for PET positivity and to a minor extent to the reader’s experience.
Our major finding was the capability of FDG-PET to identify unsuspected relapse with our true-positive PET responses is clearly related to the like lihood of relapse, where as false-positive findings were almost stable. In the current study, we calculate a sensitivity, specificity, positive p redictive value and negative predictive value of 95% and 91%, 98% and 96%, respectively negative predictive value.
Weak points includes, high cost, relatively small number of patients and relative short median follow up period.
5. Conclusion
PET/CT had significant implications in terms of early and delayed assessment of treatment response and allows accurate characterization of residual masses, identifies viable active tumor tissue within residual mass with subsequent detection of relapsing lymphoma. PET/CT offers new prognostic information in the prospective studies. All Guidelines recommend Chemoimmunotherapy treatment, PET/CT distinguishes prognosis among high-burden lymphoma with visual interpretation methods. Role of Post-treatment PET/CT and its potentiality to surveillance or decision making. Therefor PET/CT is beneficial in clinical assessment, use of standardized interpretation ways and confirmatory open or laparoscopic biopsies are required. Through prescence of non-cytotoxic treatments for lymphomas, the role of PET/CT requires reassessment in contuity. We recommended further multicentric prospective studies that incorporates a larger number of patients should be implemented to define the exact relation between certain clinical, pathological, laboratory and PET factors and fate of the disease.
References
| [1] | Younes A: Early-stage Hodgkin’s lymphoma: In pursuit of perfection. J Clin Oncol 30: 895-896, 2012. | ||
 In article In article | View Article PubMed | ||
| [2] | Rosenwald A, Wright G, Chan WC, et al: The use of molecular profiling to predict survival after chemotherapy for diffuse large-B-cell lymphoma. N Engl J Med 346:1937-1947, 2002. | ||
| In article | View Article PubMed | ||
| [3] | Cheson BD: Role of functional imaging in the management of lymphoma. J Clin Oncol 29: 1844-1854, 2011. | ||
| In article | View Article PubMed | ||
| [4] | Hutchings M, Loft A, Hansen M, et al: Position emission tomography with or without computed tomography in the primary staging of Hodgkin’s lymphoma. Haematologica 91: 482-489, 2006. | ||
| In article | PubMed | ||
| [5] | Rigacci L, Vitolo U, Nassi L, et al: Positronemission tomography in the staging of patients with Hodgkin’s lymphoma: A prospective multicentric study by the Intergruppo Italiano Linfomi. Ann Hematol 86: 897-903, 2007. | ||
| In article | View Article PubMed | ||
| [6] | Raanani P, Shasha Y, Perry C, et al: Is CT scan still necessary for staging in Hodgkin and non-Hodgkin lymphoma patients in the PET/CT era? Ann Oncol 17: 117-122, 2006 | ||
| In article | View Article PubMed | ||
| [7] | Elstrom R, Leonard JP, Coleman M, et al: Combined PET and low-dose, noncontrast CT scanning obviates the need for additional diagnostic contrast-enhanced CT scans in patients undergoing staging or restaging for lymphoma. Ann Oncol 19: 1770-1773, 2008 | ||
| In article | View Article PubMed | ||
| [8] | Pelosi E, Pregno P, Penna D, et al: Role of whole-body [18F] fluorodeoxyglucose positron emission tomography/computed tomography (FDGPET/ CT) and conventional techniques in the staging of patients with Hodgkin and aggressive non Hodgkin lymphoma [in English, Italian]. Radiol Med 113: 578-590, 2008 | ||
| In article | View Article PubMed | ||
| [9] | Karam M, Novak L, Cyriac J, et al: Role of fluorine-18 fluoro-deoxyglucose positron emission tomography scan in the evaluation and follow-up of patients with low-grade lymphomas. Cancer 107: 175-183, 2006 | ||
| In article | View Article PubMed | ||
| [10] | Janikova A, Bolcak K, Pavlik T, et al: Value of [18F]fluorodeoxyglucose positron emission tomography in the management of follicular lymphoma: The end of a dilemma? Clin Lymphoma Myeloma 8: 287-293, 2008. | ||
| In article | View Article PubMed | ||
| [11] | Wirth A, Foo M, Seymour JF, et al: Impact of [18f] fluorodeoxyglucose positron emission tomography on staging and management of early-stage follicular non-hodgkin lymphoma. Int J Radiat Oncol Biol Phys 71:213-219, 2008. | ||
| In article | View Article PubMed | ||
| [12] | Le Dortz L, De Guibert S, Bayat S, et al: Diagnostic and prognostic impact of 18F-FDG PET/CT in follicular lymphoma. Eur J Nucl Med MolImaging 37: 2307-2314, 2013. | ||
| In article | View Article PubMed | ||
| [13] | Juweid ME, Stroobants S, Hoekstra OS, etal: Use of positron emission tomography for response assessment of lymphoma: Consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J Clin Oncol 25: 571-578, 2007. | ||
| In article | View Article PubMed | ||
| [14] | Casasnovas RO ,Meignan M, Riedinger A, etal: SUV max reduction improves early Prognosis value of interim positron emission tomography scans in diffuse large B-cell lymphoma. Blood 118: 37-43, 2011. | ||
| In article | View Article PubMed | ||
| [15] | Christian F, Ingo G. S, Holger A, Juri R, Daniel M, et al: Early and Late Therapy Response Assessment With [18F] Fluorodeoxyglucose Positron Emission Tomography in Pediatric Hodgkin's Lymphoma: Analysis of a Prospective Multicenter Trial. | ||
| In article | |||
| [16] | Lavely WC, Delbeke D,Creer JP, et al: FDC PET in the follow up management of patients with newly diagnosed Hodgkin and non-Hodgkin Iymphoma after first line chemotherapy. Int J Radiat Oncol Biol Phys 57:307-315, 2003. | ||
| In article | View Article | ||
| [17] | Zinzani PL, Vittorio S, Monica T, Stefano F, Gerardo M, et al . Role of [18F]Fluorodeoxyglucose Positron Emission Tomography Scan in the Follow-Up of Lymphoma. J Clin Oncol 2009; 27:1781-1787. | ||
| In article | View Article PubMed | ||
| [18] | Lin C, Itti E, Haioun C, et al: Early 18F-FDG PET for prediction of prognosis in patients with diffuse large B-cell lymphoma: SUV-based assessment versus visual analysis. J Nucl Med 48: 1626-2014. | ||
| In article | View Article PubMed | ||
| [19] | Wahl RL, Jacene H, Kasamon Y, etal: From RECIST to PERCIST: Evolving considerations for PET response criteriain solid tumors. J Nucl Med 139. | ||
| In article | |||
| [20] | Boellaar dR: Need for standardization of 18F-FDG PET/CT for treatment response assessments. J Nucl Med 52:93S-100S, 2011. | ||
| In article | View Article PubMed | ||
| [21] | Kostakoglu L,Scho¨derH, Johnson JL, etal: Interim [(18)F] fluorodeoxy glucose positron emission tomography imaging in stage I-II non-bulky Hodgkin lymphoma: Would using combined positron emission tomography and computed tomography criteria better predict response than each test alone? Leuk Lymphoma53: 2143-2150, 2012. | ||
| In article | View Article PubMed | ||
| [22] | Sally F. B , George M., Lale K, Michel M, Martin H, et al : Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. JCO. 2013. 53: 5229-5236. JCO 2009; 27: 4385-4391. | ||
| In article | |||
| [23] | Yang DH, Ahn JS, Byun BH, etal: Interim PET/CT-based prognostic model for the treatment of diffuse large B- cell lymphoma in the postrituximabera. AnnHemato l92: 471-479, 2013. | ||
| In article | View Article PubMed | ||
| [24] | Fuertes S, Setoain X, Lopez-Guillermo A, et al: Interim FDGPET/CT as a prognosticf actor in diffuse large B-cell lymphoma. Eur J Nucl Med Mol Imaging 40: 496-504, 2013. | ||
| In article | View Article PubMed | ||
| [25] | Hoffmann M, Kletter K, Becherer A, Jager U, Chott A, Raderer M. 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) for staging and follow-up of marginal zone B-cell lymphoma. Oncology. 2003; 64(4): 336-40. | ||
| In article | View Article PubMed | ||
| [26] | Bishu S, Quigley JM, Schmitz J, Bishu SR, Stemm RA, Olsasky SM, et al. F-18-fluoro-deoxy-glucose positron emission tomography in the assessment of peripheral T-cell lymphomas. Leuk Lymphoma. 2007 Aug; 48(8): 1531-8. | ||
| In article | View Article PubMed | ||
| [27] | Wu LM, Chen FY, Jiang XX, Gu HY, Yin Y, Xu JR. 18F-FDG PET, combined FDG-PET/CT and MRI for evaluation of bone marrow infiltration in staging of lymphoma: a systematic review and meta-analysis. Eur J Radiol. 2012 Feb; 81(2): 303-11. | ||
| In article | View Article PubMed | ||
| [28] | Martin R. Weihrauch, Daniel Re, Klemens Scheidhauer, Sascha Anse´ n, Markus Dietlein, Stefanie Bischoff, Thoracic positron emission tomography using 18F-fluorodeoxyglucose for the evaluation of residual mediastinal Hodgkin disease. Blood. 2001; 98: 2930-2934. | ||
| In article | View Article | ||
| [29] | Jerusalem G, Beguin Y, Fassotte MF, Najjar F, Paulus P, Rigo P, et al. Whole-body positron emission tomography using 18F- fluorodeoxyglucose for posttreatment evaluation in Hodgkin's disease and non-Hodgkin's lymphoma has higher diagnostic and prognostic value than classical computed tomography scan imaging. Blood. 1999 Jul 15; 94(2): 429-33. | ||
| In article | PubMed | ||
| [30] | Rhodes MM, Delbeke D, Whitlock JA, et al: Utility of FDG-PET/CT in follow-up of children treatedfor Hodgkin and non-Hodgkin lymphoma. J Pediatr Hematol Oncol 28: 300-306, 2006. | ||
| In article | View Article PubMed | ||
| [31] | Zinzani PL, Musuraca G, Alinari L, etal: Pre dictiverole of positron emission tomography in the outcome of patients with follicular lymphoma. Clin Lymphoma Myeloma 7: 291-295, 2007. | ||
| In article | View Article PubMed | ||
 CiteULike
CiteULike Delicious
Delicious



){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 denoting complete remission){kind=link}
{kind=link}
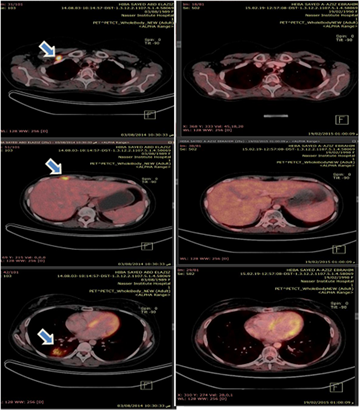
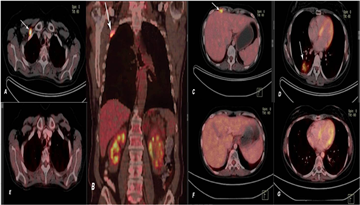
 . PET CT images at end of therapy : E, F, G, showed total resolution of the previously seen 18-FDG avid lesions denoting complete remission){kind=link}
{kind=link}
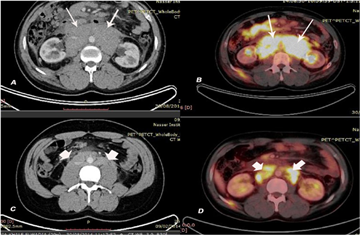
. Interterm Axial CT and axial PET CT images: C axial CT showed minimal changes in the size of the previously noted amalgamated LN mass ( CT overstating) , on the other hand PET-CT showed SUV ~ 25 recorded at the aortic bifurcation site (max. SUV ~ 12.6). denoting partial remission){kind=link}
{kind=link}
{kind=link}
{kind=link}