In line with the global trend, hospitals in the Kingdom of Saudi Arabia, including tertiary medical care centers, have increasingly adopted comprehensive electronic medical record (EMR) systems in the past twenty years. However, knowledge of these systems and the extent of their impact on performance is still limited in the Kingdom due to the lack of studies researching in this field. Accordingly, this study aims to investigate the impact of implementing a comprehensive EMR system in King Abdullah Medical City (KAMC) on hospital performance and to test the assumed hypotheses which propose that implementing a comprehensive EMR significantly improves the clinical effectiveness, patient-centeredness, patients’ safety and production efficiency in an advanced tertiary care setting in Saudi Arabia. To achieve this, a quantitative cross-sectional survey was conducted, using a valid questionnaire, on a random representative sample of 150 participants from healthcare professionals working in KAMC who experienced the upgrade towards the comprehensive EMR. The data collected was analyzed and the results showed the existence of statistically significant relationships between the implementation of comprehensive EMR as an independent variable and the four investigated dependent variables which are clinical effectiveness, patient-centeredness, patients’ safety and production efficiency in an advanced tertiary care setting in Saudi Arabia at significance level p=0.000 < 0.05. The study concluded the necessity of implementing comprehensive EMR to the point where tertiary care hospitals should pay attention to the application of such advanced electronic system because of their role in improving health care performance. Eventually, the study recommends the need to build an integrated EMR system at the level of the Kingdom that ensures the safe exchange of information between hospitals and health national centers which would enhance the provision of more distinguished health service for each patient, increase administrative efficiency and reduce the use of traditional means of recording like paper.
There has been a revolution in information technology in nearly every aspect of our life and has altered drastically throughout the last two decades, specifically in the healthcare system. Alterations in the healthcare system have resulted in significant shifts in the provision of healthcare, encouraging ambulatory treatment over hospital care, elementary care over specialized care and guidance care over independent decision-making 1, 2.
An electronic medical record (EMR) system is defined as a systematic electronic collection of health-related information about patients that can be created, gathered, managed and consulted by authorized clinicians and staff within one health care organization 3. Some researchers in spite of some disputes argue that EMR has the potential to provide substantial benefits to physicians, clinic practices and health care organizations 4, 5, 6.
Based on expert consensus, EMR systems can be classified as basic or comprehensive depending on the included system's functionalities. A key difference between the two categories is that the basic EMR systems lack some functions that might include but not limited to physician notes and nursing assessments in addition to decision support system (DSS) that provides up-to-date medical knowledge, reminders or other actions that aid health professionals in decision making 7. In Saudi Arabia, most tertiary care hospitals have some sort of basic EMR system with some examples that switched recently to a comprehensive system.
Although several studies on the effects of EMR implementation have been published with mixed results 8, 9, there is little information that compares basic and comprehensive EMR systems in terms of their impact on hospital performance, especially in the advanced tertiary care setting 10, 11, 12. Moreover, the impact of such information technology is not enough studied in hospitals in Saudi Arabia. Understanding whether a relationship exists or not can help decision makers decide or plan which type of EMR system would be more appropriate and worth considering, taking into account the economic cost of each system. In this research, health care professionals' perception of the newly implemented EMR in terms of hospital performance in King Abdullah Medical City (KAMC), Saudi Arabia will be studied in comparison to the previous basic EMR, trying to find some answers regarding the better option that tertiary care hospitals should implement.
Of note, KAMC has recently switched its basic record system into a comprehensive one as part of its vision to cope with the latest development in electronic services. Therefore, this study focuses on determining whether a relationship between a comprehensive EMR system and hospital performance exists when implemented in an advanced Saudi tertiary care center. Perception of health care professionals was measured on multiple dimensions including clinical effectiveness, patient-centeredness, production efficiency and patient safety in order to answer the following question:
What is the impact of comprehensive EMR system on hospital performance in KAMC?
1.1. Research Aim and ObjectivesThe aim of this study is to assess the impact of comprehensive EMR system in KAMC on hospital performance. In a more detailed setting, the objectives of this research are as follows:
1. To highlight the changes related to clinical effectiveness after applying the new EMR system in the perception of KAMC health care professionals.
2. To assess the changes related to the patient-centeredness after applying the new EMR system in the perception of KAMC health care professionals.
3. To assess the changes related to the patients' safety after applying the new EMR system in the perception of KAMC health care professionals.
4. To evaluate the changes related to production efficiency after applying the new EMR system in the perception of KAMC health care professionals.
1.2. Research Hypothesis- There is a significant positive relationship between comprehensive EMR and clinical effectiveness in an advanced tertiary care setting in Saudi Arabia.
- There is a significant positive relationship between comprehensive EMR and patient-centeredness in an advanced tertiary care setting in Saudi Arabia.
- There is a significant positive relationship between comprehensive EMR and patients' safety in an advanced tertiary care setting in Saudi Arabia.
- There is a significant positive relationship between comprehensive EMR and production efficiency in an advanced tertiary care setting in Saudi Arabia.
1.3. Variables in ResearchIndependent variable in this study is the comprehensive EMR system, which was recently implemented, whereas the dependent variables that will measure the hospital performance include clinical effectiveness, patient-centeredness, patient safety and production efficiency.
1.4. Research TerminologyThe definition of each variable is as follows:
- Comprehensive EMR System: The Electronic Medical Record System (EMR) is one of the important components in Hospital Information System 13. EMRs are seen as a way to simplify the management of patient information, increase productivity and lower costs associated with medical information management 14. The comprehensive type of EMR is an advanced version with additional functions that might include but not limited to physician notes and nursing assessments in addition to decision support system (DSS) that provides up-to-date medical knowledge, reminders or other actions that aid health professionals in decision making 7.
- Clinical effectiveness: it was defined by the DH in 1996 as “the extent to which specific clinical interventions, when deployed in the field for a particular patient or population, do what they are intended to do - that is, maintain and improve health and secure the greatest possible health gain from the available resources” 15. Thus, clinical efficacy can be defined as one of the dimensions of performance, whereby the hospital, in line with the existing state of knowledge, provides appropriate and efficient clinical care or services to reach the desired results for all patients who are probable to advantage the most.
- Patient centeredness: The Institute of Medicine (IOM) defines patient centeredness as: “Providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions” 16. Patient-centeredness is a consistency of family, professional, and business connections. Therefore, patient-centered treatment programs would consider the patient-centeredness of patients (and their families), physicians, and health-care structures.
- Patient’s safety: The clearest definition of patient safety is to prevent errors and adverse health care-related impacts on patients. Although health care has become more successful it has also become more complex, with increased utilization of modern technology, medicines, and treatments 17. Patient safety as a means of preventing patient harm. Focus is put on the healthcare system that avoids errors; learns from the mistakes that occur; and builds on a safety culture that includes health care staff, institutions, and patients.
- Production efficiency: it is “an economic term describing a level in which an economy or entity can no longer produce additional amounts of a good without lowering the production level of another product” 18. Production efficiency is one of the most significant issues for performance organizations, both strategic and operational. In several cases, the output efficiency can be increased.
A quantitative method is applied. The quantitative approach primarily emphasizes on analyzing and collecting data using structured surveys to collect data from a large sample. This technique is also deemed the most suitable strategy when the researcher tries to examine and grasp the thoughts and motivations of the actions. Through collecting and analyzing data this approach utilizes deductive reasoning to test the proposed hypotheses 19. A quantitative approach as it aims to examine the connection between variables is deemed reasonable 20. The main objective of this method is to define the possible relationship between two or more variables 21, as in this research case.
2.1. Study PopulationThe study population includes all the employees of the tertiary care center in KAMC who experienced the upgrade towards the comprehensive EMR system. They were estimated to be around 1,000 employees. The reason for choosing this population is that they are most closely related to assessing the impact of comprehensive EMR system on hospital performance in KAMC in terms of clinical effectiveness, patient-centeredness, patients' safety and production efficiency.
2.2. Sampling ProcedureBecause of the vast size of population, scientists and researchers frequently cannot test each person in the population as long as it is excessively costly and time consuming. Therefore, the researchers tend to depend on sampling techniques. Hence, simple random sampling method was applied in selecting sample from the population of this study 22. Simple random sampling procedure is appropriate for research since hospitals receive patients at different times, and there are no scheduled appointments, and therefore, this approach is more suitable for obtaining a random sample from staff who dealt with these cases 23.
A random representative sample was selected from employees of the tertiary care center in KAMC in Saudi Arabia to apply the primary data collection tool for this study to them. Respondents chosen from the population were provided with a letter of participation at the beginning of the survey explaining the purpose of the survey in addition to ensuring their confidentiality and anonymity before starting to complete the questionnaire. Consequently, completed questionnaires indicate the consent of their respondents to participate.
2.3. Sampling CriteriaA sampling frame criterion was adopted to select the random sample from the population, where only staff with knowledge and experience with the newly implemented EMR at KAMC was included in the study sample. The researcher assured that any participant included in this study has at least 3 years of experience and is at least 20 years old, to ensure the validity and reliability of the obtained data.
2.4. Sample SizeA sample size of 150 participants (n=150) from the physicians, nurses, pharmacists, lab technicians, administration staff as well as medical records management professionals working in the selected KAMC, who follow the previously mentioned sampling criteria, was included in the study. The Sample size is adequate and sufficient for this study as it was calculated using Krejcie and Morgan’s 24 formula for detecting sample size of a known population size, assuming a prevalence of 50% satisfactory level of knowledge of EMR among staff, a confidence interval of 95%, and a margin of error of 5%. This would lead to a statistical significance results with minimum errors.
2.5. Data Collection Tool and ProcessAs the quantitative approach is adopted in this study, the questionnaire is the most appropriate study tool to collect data. Hartas 25 showed that the questionnaire is the simplest tool to collect data on a specific topic and that it is suitable for collecting a large amount of data in a short time and with the required efficiency. Due to the questionnaire's accuracy, speed and ease of use, it was used in this study as a tool for primary data collection as indicated previously.
The study tool (questionnaire) is designed based on previous relevant studies and literature 26, 27, 28. The questionnaire consists of two different parts with a set of closed statements directed towards collecting data on the different study variables. The first part of the questionnaire consists of questions covering the sociodemographic information of the selected sample participating in this study. The second section includes a group of 32 sentences; 5 of them are asking about the independent variable implementation of comprehensive EMR in KAMC) and 27 of them are asking about the dependent variables related to the hospital tertiary care centers’ performance including (clinical effectiveness, patient centeredness, patients’ safety and production efficiency). Before evaluating the hypotheses and obtaining results, it was necessary to verify the reliability and validity of the measurement tool before its implementing on the study sample. In this study, the content validity of the tool (questionnaire) was confirmed by presenting it to a group of specialists in the science of management and economics in hospitals and universities of Saudi Arabia to validate its correctness and freedom of errors. He was also asked to amend, add, or delete any of the statements.
Moreover, the reliability of the questionnaire was verified by conducting a pilot study on a sample of 30 healthcare professionals working in KAMC other than the members of the original sample. The reliability of the tool and its components was determined by SPSS’ Alpha Cronbach test before distributing the tool to the study sample members and conducting the real study. Table 1 shows the Cronbach alpha values for the overall questionnaire and its different parts.
As shown in Table 1, Cronbach’s alpha was determined to be (0.878) for elements of the first variable (implementation of comprehensive EMR in KMAC), (0.889) for elements of the second variable (clinical effectiveness), (0.921) for elements of the third variable (patient-centeredness), (0.909) for elements of the fourth variable (patients’ safety) and (0.826) for elements of the fifth variable (production efficiency). However, it was (0.920) for the overall instrument elements, which means that the reliability of the instrument is acceptable as long as Cronbach's Alpha values for each of the variables as well as the whole questionnaire’s elements are higher than (0.7) 29.
The five-point Likert Scale was utilized to collect the questionnaire's items responses. This scale utilized the five following responses: strongly disagree, disagree, neutral, agree and strongly agree where participants were required to express the level of their agreement according to this scale. The questionnaires were distributed and collected between August 2020 and December 2020 and the last responses were collected on December 15th, 2020. Participants had the option to complete the questionnaire in Arabic and English. In addition, an online link has been provided to all participants, and sent to them by e-mail so that they can fill out a copy of the questionnaire online.
2.6. Data AnalysisData analysis and interpretation is the method of assigning value to the information gathered and evaluating the assumptions, importance, and implications of the results. It represents a significant and exciting stage in the design process. The study approaches data collection in all scientific studies. Data analysis methods in the absence of primary data collection can involve discussing common patterns, as well as, controversies within secondary data directly related to the research area. Data analysis will be done following the descriptive method using SPSS. Charts will analyze data as percentages to show the relationships.
2.7. Statistical MethodsThe data plays a crucial role in pursuing the objectives of studies and scientific research, as it is used to examine facts in addition to checking the validity or fallacy of theories, as well as presenting answers to the questions and inquiries the researcher addresses. Following the process of gathering and processing primary and secondary data from its sources, the research attempts to turn these data into facts and information which can be reported and used by applying a collection of statistical methods. Therefore, after review and analysis, the outcomes developed on the basis of the study's preliminary data in an appropriate manner accomplish the study's objectives and reflect its effects. The Statistical Package Program (SPSS) is used in this study. There will be a variety of statistical tools used which are classified as follows:
1- Descriptive Statistics Metrics:
- Frequencies and percentages for specific (demographic) variables to demonstrate sample population features, divided by categories.
- Standard mean and deviations to determine the level of both the independent and dependent variable and the order of the dimensions of the study variables.
2. Analytical Statistics Metrics:
- Alpha Cronbach test to test the stability of the study tool.
- Pearson correlation to test the relationship between the dependent and independent variables.
- Simple regression analysis to test the study’s hypotheses.
2.8. Ethical ConsiderationsThe participation was voluntary, and the staff of KAMC was assured of no consequences of failing to participate. The study was approved by IRB of the same institution. All the willing participants was provided with a letter of participation at the beginning of the survey clarifying the purpose of the survey and ensuring that their identity and the confidentiality of the data they provide are not disclosed. Confidentiality of the findings was upheld while ethical approval was obtained from the institution. The informed consent illustrated the researchers name and the name of the supervisor from the research office. It is also clear that the participants do not need to sign approval to choose their agreement or disagreement. Their approval to complete the questionnaire was understood as informed agreement.
2.9. Data SecurityThe researcher was keen to maintain the confidentiality of the information obtained, so he worked to keep the identity of the study participants anonymous. Moreover, a copy of the data provided by them was kept with the researcher and the supervisor only. The researcher emphasized during data collection that the data will only be used for research and academic purposes, so he used it in the statistical analysis of this study to obtain the required results, and he kept it to return to it when he needs to check or review the results that have been reached.
In the previous section, the research discussed and explained the quantitative descriptive method used in this study to collect and analyze data. Accordingly, the current part seeks to analyze the data collected from the quantitative questionnaires applied to a sample of 150 healthcare professionals working in KAMC in order to obtain a comprehensive and influential conclusion regarding the impact of comprehensive EMR system in KAMC on hospital performance.
3.1. Sample Socio-demographic CharacteristicsAfter the questionnaires were distributed and filled out by the 150 randomly selected respondents, a descriptive statistical analysis was performed by SPSS to determine the social and demographic characteristics of the sample members. The analysis of the demographic characteristics of the sample is important, because it helps in knowing the characteristics of the sample community and the nature of the characteristics of the people participating in the completion of the questionnaire, the extent of their experience and their connection with the subject, as well as identifying the personal differences between them and whether they affect the nature of the answers submitted by them or not 30. The sample of this study consists of both gender (males and females). Majority of the sample were male (74.7%), while the female category constitutes (25.3%) of the total sample. Moreover, the most participated age category in this survey was 31-40 years old with a percentage of 56% followed by 22% participants of 41-50 years old and 15% of health care professionals participated in this study were in the age of 20-30 years old.
It is also noteworthy that the whole members of the study sample were well-educated in which the vast majority of participants (36%) were holders of a bachelor's degree, while 29% of the study sample were postgraduate medical education recipients and the remaining participants had either a master or doctorate degree. In regards to job position, there was a diversity in the job title of the individuals participating in this questionnaire, but the largest percentage of it were physicians who accounted for 68% of the sample followed by nurses at 10%. The other categories of job title such as pharmacists, lab technicians, administration staff and individuals working with medical records management constituted around 22% of the whole sample. Finally, regarding years of experience, the vast majority of participants were healthcare professionals who had 10-20 years of experience (43%), followed by individuals who had 5-10 years of experience (27%). This indicates that the study sample consists of healthcare professionals with various experiences, which gives the impression that they possess extensive knowledge in the field of study and that their answers will be representative and trustworthy.
3.2. The Descriptive Data Analysis ResultsIn order to descriptively identify the impact of upgrading towards a comprehensive EMR system on KAMC hospital performance indicators (clinical effectiveness, patient centeredness, patients’ safety and production efficiency), the descriptive statistics (means and standard deviation) of the responses and their ranks, which were elicited using a five-point Likert scale were calculated via SPSS, where means ranging from (1-1.80) were considered very low, from (1.81 to 2.60) were considered low, from (2.61-3.40) were considered moderate, from (3.41-4.20) were considered high and from (4.21-5.00) were considered very high.
In this part, the descriptive analysis of the collected data focuses on investigating the independent factor of this study which is the characteristics and degree of implementation of advanced EMR technology from the perceptions of KAMC health care professionals. So, in order to evaluate this variable, descriptive summary (means & standard deviation) of the responses to the variable items were calculated as shown in the following Table 2:
It can be noticed from Table 2 above that the arithmetic means that measure the implementation of comprehensive EMR system in KMAC are high and ranging from (3.913-4.120). It can be noticed that item (1), which states that: "The specialist care services at KAMC use comprehensive electronic system that helps in recording doctor notes and nursing assessments precisely", represents the highest agreed statement (4.120, Std. = 0.904) and was followed by item (5) secondly in which it stated that: "The new comprehensive EMR system provides complete information about the medical care plan and patient history in the health facility while protecting the patient’s confidentiality and privacy" with a mean (4.040, Std.= 0.933), thirdly item (4) in which it stated that: "The hospital’s new EMR systems are comprehensive and with which patient records are arranged and captured quickly and accurately" with a mean (4.013, Std.= 0.955), fourthly item (3) which stated that: "The tertiary care center of KAMC applies comprehensive EMR systems that contain patients’ progress assessments, problems, medications, vital signs, laboratory statements, radiological reports and more" with a mean (3.926, Std.= 1.010) and finally with the least mean value, item (2) which stated that: "The basic EMR system in the hospital’s complex medical and surgical intervention services have been replaced by comprehensive system that provides the possibility to document consultation requests and those related to decision support such as reminders and alerts" with a mean (3.913, Std.= 1.104).
The overall mean for this section was (4.002) which shows that most of the study sample highly agrees with the items of this part of the study, which indicates their agreement on the availability and effectiveness of comprehensive EMR systems in specialized care services in KAMC, and that the tertiary care centre of the city has a comprehensive EMR that helps in accurately recording doctor's notes and nursing evaluations, as the basic EMR system in complex medical and surgical intervention services in the hospital has been replaced by a comprehensive system that provides the possibility of documenting consultation requests and those related to decision support such as reminders and alerts, in addition to arranging and capturing patient records quickly and accurately, while protecting patient privacy and confidentiality.
In this part, the descriptive analysis of the collected data focuses on investigating the first dependent indicator of performance which is the changes related to clinical effectiveness after replacing the old EMR system with an advanced comprehensive EMR from the perceptions of KAMC health care professionals. So, in order to evaluate this variable, descriptive summary (means & standard deviation) of the responses to the variable items were calculated as shown in the following Table 3:
It can be noticed from Table 3 that the arithmetic means that measure the clinical effectiveness in the tertiary care setting in KAMC are high and ranging from (3.85-4.15). It can be noticed that item (3), which states that: "The newly implemented EMR system allows better guideline- or protocol-based care", represents the highest agreed mean statement (4.150, Std. = 0.833) and was followed by item (7) secondly in which it stated that: "The new EMR captures point-of-care data that inform and improve practice through quality improvement projects, practice-level interventions, and informative research" with a mean (4.120, Std.= 0.897), thirdly item (5) in which it stated that: "The new EMR system helps to enhance preventive health care including disease surveillance and monitoring" with a mean (4.080, Std.= 0.952), fourthly item (2) which stated that: "Using the new EMR system has resulted in a positive effect on patient care and provided clinical services" with a mean (3.990, Std.= 1.030) and finally with the least mean value, item (1) which stated that: "I think the new EMR System is more useful in exchanging meaningful clinical information among professional healthcare teams" with a mean (3.850, Std.= 0.968).
The overall mean for this section was (4.015) which shows that there is a high agreement from respondents on the clinical effectiveness of using the comprehensive EMR in KAMC in terms of the ability to easily exchange useful clinical information between professional health care teams, making a positive impact on patient care and clinical services provided, enhancing preventive health care, including disease surveillance, and facilitating the process of communication between various care providers, doctors, nurses, medical residents and other interested parties in the medical field, in a way that improves the quality of services.
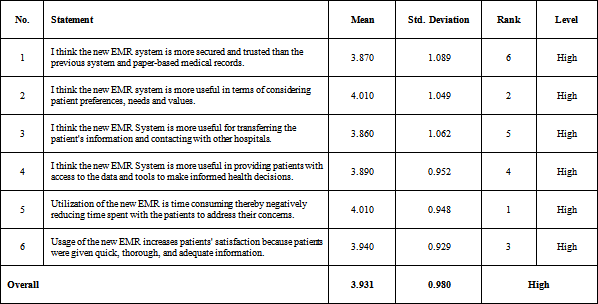
In this part, the descriptive analysis of the collected data focuses on investigating the second dependent indicator of performance which is the changes related to patient-centeredness after replacing the old EMR system with an advanced comprehensive EMR from the perceptions of KAMC health care professionals. So, in order to evaluate this variable, descriptive summary (means & standard deviation) of the responses to the variable items were calculated as shown in the following Table 4:
It can be noticed from Table 4 above that the arithmetic means that measure the the patient-centeredness in the tertiary care setting in KAMC are high and ranging from (3.87-4.01). It can be noticed that item (5), which states that: "Utilization of the new EMR is time consuming thereby negatively reducing time spent with the patients to address their concerns", represents the highest agreed mean statement (4.010, Std. = 0.948) and was followed by item (2) secondly in which it stated that: "I think the new EMR system is more useful in terms of considering patient preferences, needs and values" with a mean (4.010, Std.= 1.049), thirdly item (6) in which it stated that: "Usage of the new EMR increases patients' satisfaction because patients were given quick, thorough, and adequate information" with a mean (3.940, Std.= 0.929), fourthly item (4) which stated that: " I think the new EMR System is more useful in providing patients with access to the data and tools to make informed health decisions" with a mean (3.890, Std.= 0.952), fifthly item (3) which stated that: "I think the new EMR System is more useful for transferring the patient's information and contacting with other hospitals" with a mean (3.860, Std.= 1.062) and finally with the least mean value, item (1) which stated that: "I think the new EMR system is more secured and trusted than the previous system and paper-based medical records" with a mean (3.870, Std.= 1.089).
The overall mean for this section was (3.931) which indicates that most of the study sample members strongly agree with the items of this part of the study and indicates that there is great agreement on the ability of the new comprehensive EMR system to focus on the patient (patient-centeredness) in KAMC in terms of being safer and reliable than the previous basic medical records systems, and more sensitive to patient preferences, needs and values, as well as the great benefit of it regarding the facilitation of accessing data and tools needed to make informed health decisions.
In this part, the descriptive analysis of the collected data focuses on investigating the third dependent indicator of performance which is the changes related to patients’ safety after replacing the old EMR system with an advanced comprehensive EMR from the perceptions of KAMC health care professionals. So, in order to evaluate this variable, descriptive summary (means & standard deviation) of the responses to the variable items were calculated as shown in the following Table 5:
It can be noticed from Table 5 above that the arithmetic means that measure the patients’ safety in the tertiary care setting in KAMC are high and ranging from (3.760-4.090). It can be noticed that item (2), which states that: "The new EMR system provides fast access to patient information whenever it is needed for prompt life-saving health care", represents the highest agreed mean statement (4.090, Std. = 1.006) and was followed by item (5) secondly in which it stated that: "Using the new EMR system improves safety through improved management" with a mean (4.030, Std.=0.944), thirdly item (3) in which it stated that: "I think the new EMR System is more useful in providing medication reconciliation" with a mean (3.930, Std.= 0.991), fourthly item (6) which stated that: "Decision support feature included in the new EMR system in the form of computerized reminders is a significant tool that contributes to better patient safety" with a mean (3.910, Std.= 1.038) and finally with the least mean value, item (7) which stated that: "The new EMR could jeopardize patient care through the usage of "copy and paste" syndrome" with a mean (3.760, Std.= 1.091).
The overall mean for this section was (3.918) which indicates that most of the study sample members strongly agree with the items of this part of the study and indicates that there is great agreement on the ability of the new comprehensive EMR system to enhance patients’ safety in KAMC in terms of reducing medication errors and hospitalization complications compared to the previous basic system and medical record, as well as providing rapid access to patient information whenever the need arises and thus the ability to provide life-saving healthcare.
In this part, the descriptive analysis of the collected data focuses on investigating the fourth dependent indicator of performance which is the changes related to production efficiency after replacing the old EMR system with an advanced comprehensive EMR from the perceptions of KAMC health care professionals. So, in order to evaluate this variable, descriptive summary (means & standard deviation) of the responses to the variable items were calculated as shown in the following Table 6:
It can be noticed from Table 6 above that the arithmetic means that measure production efficiency in the tertiary care setting in KAMC are high and ranging from (3.84-4.01). It can be noticed that item (1), which states that: "Utilization of the new EMR reduces time spent retrieving records thereby allowing faster delivery of patient care", represents the highest agreed mean statement (4.010, Std. = 0.934) and was followed by item (2) secondly in which it stated that: "The use of new EMR system enables clinicians to assess more patients within a shorter period of time" with a mean (3.990, Std.= 1.030), thirdly item (7) in which it stated that: "Implementing such a new EMR in healthcare will improve efficiency and positively affect patient flow" with a mean (3.879, Std.= 0.964), fourthly item (6) which stated that: "Utilization of the new EMR system reduces the pressure on the health staff thereby enhancing production efficiency" with a mean (3.870, Std.= 0.964) and finally with the least mean value, item (5) which stated that: "The new EMR system results in a significant decrease of unnecessary health services utilization" with a mean (3.840, Std.= 1.069).
The overall mean for this section was (3.897) which indicates that most of the study sample members strongly agree with the items of this part of the study and indicates that there is great agreement on the ability of the new comprehensive EMR system to enhance the production efficiency in KAMC in terms of reducing the time it takes to retrieve records, which allows to speed up patient care, in addition to enabling doctors to examine and diagnose a larger number of patients within a shorter period of time, and its contribution to speeding up drug delivery, laboratory tests, radiological examinations and other health care services, and improving efficiency and impact positively on patient flow.
3.3. Hypotheses TestingThis part is concerned with testing the study's hypotheses related to the impact of upgrading towards comprehensive EMR on the hospital performance indicators including clinical effectiveness, patient-centeredness, patients' safety and clinical effectiveness in an advanced tertiary care setting in KMAC. Accordingly, the Pearson correlation and multiple linear regression analysis were utilized to test the existence of relationships (hypotheses) between independent variable (IV) (comprehensive EMR) and the dependent variables (DVs) (clinical effectiveness, patient-centeredness, patients' safety and clinical effectiveness) and the significance of those relationships.
The correlation between comprehensive EMR (IV) and clinical effectiveness (DV), indicated as the first hypothesis of this study: H1: There is a significant positive relationship between comprehensive EMR and clinical effectiveness in an advanced tertiary care setting in Saudi Arabia, was tested through Pearson correlation and simple linear regression analysis, where Table 7 represents the resulted model summary for this regression and correlation test:
From the above Table 7, the model summary and overall fit statistics indicates that there is a statistically significant positive impact of the implementation of comprehensive EMR on the clinical effectiveness in an advanced tertiary care setting in Saudi Arabia, where the coefficient of Pearson correlation R (0.988) at (α≤ 0.05). The coefficient of determination R2 amounted to (0.977), this means that (97.7%) of the positive changes in the clinical effectiveness in KAMC are because of the replacing of the old EMR system with an advanced EMR technology. Moreover, the degree of impact (β) for the implementation of comprehensive EMR on the clinical effectiveness in an advanced tertiary care setting of KAMC in Saudi Arabia is (0.943). This means that a one-step increase in the level of implementation of comprehensive EMR in KAMC improves the clinical effectiveness by (0.943). The significance of this effect is the value of the calculated (F) which reached (6172.260) and is significant at the level of (α <0.05) (sig. =0.000). This confirms the validity of the acceptance of the first hypothesis which states: “There is a significant positive relationship between comprehensive EMR and clinical effectiveness in an advanced tertiary care setting in Saudi Arabia”.
The correlation between comprehensive EMR (IV) and patient-centeredness (DV), indicated as the second hypothesis of this study: H2: There is a significant positive relationship between comprehensive EMR and patient-centeredness in an advanced tertiary care setting in Saudi Arabia, was tested through Pearson correlation and simple linear regression analysis, where Table 8 represents the resulted model summary for this regression and correlation test:
From the above Table 8, the model summary and overall fit statistics indicates that there is a statistically significant positive impact of the implementation of comprehensive EMR on the patient-centeredness in an advanced tertiary care setting in Saudi Arabia, where the coefficient of Pearson correlation R (0.951) at (α≤ 0.05). The coefficient of determination R2 amounted to (0.904), this means that (90.4%) of the positive changes in the patient-centeredness in KAMC are because of the replacing of the old EMR system with an advanced EMR comprehensive technology. Moreover, the degree of impact (β) for the implementation of comprehensive EMR on the patient-centeredness in an advanced tertiary care setting of KAMC in Saudi Arabia is (0.908). This means that a one-step increase in the level of implementation of comprehensive EMR in KAMC improves the patient-centeredness by (0.908). The significance of this effect is the value of the calculated (F) which reached (5813.766) and is significant at the level of (α <0.05) (sig. =0.000). This confirms the validity of the acceptance of the second hypothesis which states: “There is a significant positive relationship between comprehensive EMR and patient-centeredness in an advanced tertiary care setting in Saudi Arabia”.
The correlation between comprehensive EMR (IV) and patients' safety (DV), indicated as the third hypothesis of this study: H3: There is a significant positive relationship between comprehensive EMR and patients' safety in an advanced tertiary care setting in Saudi Arabia, was tested through Pearson correlation and simple linear regression analysis, where Table 9 represents the resulted model summary for this regression and correlation test:
From the above Table 9, the model summary and overall fit statistics indicates that there is a statistically significant positive impact of the implementation of comprehensive EMR on the patients’ safety in an advanced tertiary care setting in Saudi Arabia, where the coefficient of Pearson correlation R (0.978) at (α≤ 0.05). The coefficient of determination R2 amounted to (0.956), this means that (95.6%) of the positive changes in the patients’ safety in KAMC are because of the replacing of the old EMR system with an advanced EMR comprehensive technology. Moreover, the degree of impact (β) for the implementation of comprehensive EMR on the patients’ safety in an advanced tertiary care setting of KAMC in Saudi Arabia is (1.038). This means that a one-step increase in the level of implementation of comprehensive EMR in KAMC improves the patients’ safety by (1.038). The significance of this effect is the value of the calculated (F) which reached (6569.231) and is significant at the level of (α <0.05) (sig. =0.000). This confirms the validity of the acceptance of the third hypothesis which states: “There is a significant positive relationship between comprehensive EMR and patients’ safety in an advanced tertiary care setting in Saudi Arabia”.
The correlation between comprehensive EMR (IV) and production efficiency (DV), indicated as the fourth hypothesis of this study: H4: There is a significant positive relationship between comprehensive EMR and production efficiency in an advanced tertiary care setting in Saudi Arabia, was tested through Pearson correlation and simple linear regression analysis, where Table 10 represents the resulted model summary for this regression and correlation test:
From the above Table 10, the model summary and overall fit statistics indicates that there is a statistically significant positive impact of the implementation of comprehensive EMR on the production efficiency in an advanced tertiary care setting in Saudi Arabia, where the coefficient of Pearson correlation R (0.983) at (α≤ 0.05). The coefficient of determination R2 amounted to (0.967), this means that (96.7%) of the positive changes in the production efficiency in KAMC are because of the replacing of the old EMR system with an advanced EMR comprehensive technology. Moreover, the degree of impact (β) for the implementation of comprehensive EMR on the patients’ safety in an advanced tertiary care setting of KAMC in Saudi Arabia is (1.018). This means that a one-step increase in the level of implementation of comprehensive EMR in KAMC improves the patients’ safety by (1.018). The significance of this effect is the value of the calculated (F) which reached (4315.960) and is significant at the level of (α <0.05) (sig. =0.000). This confirms the validity of the acceptance of the fourth hypothesis which states: “There is a significant positive relationship between comprehensive EMR and production efficiency in an advanced tertiary care setting in Saudi Arabia”.
EMRs are widely believed to have a powerful and significant impact in improving the safety, efficiency and quality of care while protecting patient privacy and personal rights. Therefore, EMR has become an essential part of our modern healthcare field as it is concerned with the complete management of various patient information, including the retrieval of test results, prescription of medicines, patient history, etc., which is expected to increase the quality of healthcare, enhance skills of making clinical decision, and reduce long-term medical expenses.
On the other hand, there are few studies that underestimate the importance of EMR in terms of their effects on hospital performance. Yanamadala et al. 31 have conducted observational research by utilizing State Inpatient Databases connected to the American Hospital Association survey. Their research findings show that patients who received medical and surgical treatment in facilities without an EMR program had similar outcomes compared to patients receiving care in hospitals with such a system when accounting for significant confounders. A study by Kaneko et al. conducted to evaluate the impact of EMRs on hospital productivity in Japan showed no significant association found between EMR implementation and labor productivity growth 32. It concluded that EMR implementation has an adverse effect on the productivity and profitability of municipal hospitals in Japan and this finding should be considered when developing future healthcare policies promoting the implementation of IT. Based on these finding, EMRs can perform a lesser role in patient outcome and total quality of healthcare than anticipated.
The literature indicates that implementation of comprehensive EMRs is limited and in some cases sporadic in developing as well as low-income countries, largely due to the financial and implementation challenges these countries face. These challenges are likely due to technological, organizational, financial, or human resource barriers. However, the Kingdom of Saudi Arabia is trying to adapt to global developments and technologies in order to improve the health of its citizens and increase the efficiency of its health-care centers. So, in order to achieve the vision of the Kingdom of Saudi Arabia 2030 in the health sector, the Kingdom is heading to face these technical and organizational challenges, and to support its health organizations and hospitals with modern health information systems (HIS) and other technologies that contribute to raising the level of public health of its citizens and contribute to achieving its leadership.
In the Kingdom of Saudi Arabia, several initiatives have been taken to implement comprehensive EMR systems over the past two decades. It should be noted that KAMC recently, last year, transformed its basic EMR into a comprehensive system as part of its vision to cope with the latest developments in electronic services. Therefore, this study, which might be the first of its kind in the kingdom, was made to evaluate the effectiveness of this new system and determine whether there was a relationship between the comprehensive EMR and the hospital's performance when applying this system at the Saudi tertiary center (KAMC). Furthermore, the implementation and use of comprehensive EMR have some barriers, such as economic costs and the lack of availability of staff with adequate IT expertise. Accordingly, the presented study should help the decision-makers in the healthcare sector get an insight into whether comprehensive EMR would be worth implementing and considering when looking at hospital performance indicators on multiple dimensions.
The results of the analyzed questionnaires of the 150 from the physicians, nurses, pharmacists, lab technicians, administration staff as well as medical records management professionals working in KAMC, who represented the study sample, showed the availability and effectiveness of comprehensive EMR systems in specialized care services in KAMC, and that the tertiary care centre of the city has a comprehensive EMR that helps in accurately recording doctor's notes and nursing evaluations. It has been revealed that the basic EMR system in complex medical and surgical intervention services in the hospital has been replaced by a comprehensive system that provides the possibility of documenting consultation requests and those related to decision support such as reminders and alerts, in addition to arranging and capturing patient records quickly and accurately, while protecting patient privacy and confidentiality. This is consistent with Hasanain, Vallmuur and Clark’s study 33, which confirmed the adoption and direction of many health care organizations in Saudi Arabia such as the National Guard Health Affairs (NGHA) in strengthening many Saudi hospitals and providing them with comprehensive EMR systems. It was indicated that according to an initiative by the NGHA, the capacity of the EMR system and the quality of its services was expanded to include all primary ambulatory care, secondary and tertiary care centres. Those centres were provided with the latest systems to organize medical records starting from 2008, and work is still underway to update them every period and replace them with modern and more effective ones.
Furthermore, the study revealed the existence of statistically significant relationships between comprehensive EMR as an independent variable and the four investigated dependent variables which are clinical effectiveness, patient-centeredness, patients’ safety and production efficiency in an advanced tertiary care setting of KAMC in Saudi Arabia at significance level p=0.000 < 0.05. The following is an explanation of these relationships:
In regards to the outcome that showed a positive significant relationship between comprehensive EMR and clinical effectiveness in an advanced tertiary care setting in Saudi Arabia, this result can be explained by the fact that the utilization of comprehensive EMR in KAMC increases the ability to easily exchange useful clinical information between professional healthcare teams, making a positive impact on patient care and clinical services provided, and enhancing preventive healthcare, including disease surveillance, facilitating the process of communication between different caregivers, doctors, nurses, medical residents and other parties interested in the medical field, in a way that improves the quality of services and clinical effectiveness, which was emphasized in the study of Gardner et al. 5. Moreover, there is a consistency between this result and the studies of Kwan et al. and Adler-Milstein et al. 1, 34 who showed that the utilization of EMRs including the comprehensive system, has an positive impact on many medical fields, and the most important of these areas is preparing statistical reports related to work and transferring laboratory results between different departments and its ability to give alert signals in case the values exceed the normal rates. It additionally facilitates access to the medical record and stores data related to patients, facilitates the process of filling out results and completing the necessary information for auditors electronically, and facilitates the process of linking medical information in order to conduct medical surveys and research, as well as facilitating the process of communication and coordination between the internal departments in the hospital and enabling the ease refer to the medical records and information related to patients electronically by electronic archiving at any time, in a way that improves the quality of services and clinical effectiveness.
The second result of this study which showed a positive significant relationship between comprehensive EMR and patient-centeredness in an advanced tertiary care setting in Saudi Arabia can be explained by the fact that the utilization of comprehensive EMR in KAMC increases the ability to focus on patients and provide care that respects and responds to the patient's preferences, needs and individual values, as it focuses on providing accurate information about the patient, whether it is personal information, information about the diagnosis of his disease, or information about the results of medical tests and examinations, or information about the treatment and its scheduled program and the extent of the patient's response to this treatment and other things that contribute to raising the efficiency of medical care, which was emphasized in the study of Kalra, Baruah and Unnikrishnan 16 and Aldosari et al. 27. Furthermore, there is a consistency between this result and the studies of Adler-Milstein et al. and Aldebasi et al. 34, 35 which indicated that the use of comprehensive EMR is related to improving performance and increasing the ability to focus on patients, as it facilitates the process of entering patient information and helps them in improving the quality of health care service. The system also contributes to increasing the effectiveness of communications between doctors and other departments, as well as speeding up and developing procedures, and maintaining high standards in services.
The third outcome that showed a positive significant relationship between comprehensive EMR and patients’ safety in an advanced tertiary care setting in KAMC Saudi Arabia can be clarified by the fact that the utilization of comprehensive EMR in KAMC contributes to reducing medication errors and hospitalization complications compared to the previous statute and traditional medical record, as well as providing quick access to patient information whenever needed, thus being able to provide life-saving healthcare and patients’ safety, which was emphasized in the study of Kalra, Baruah and Unnikrishnan 16 and Aldosari et al. 27. Moreover, this is in line with Ariffin et al. and Lin et al. 36, 37 studies who showed that the use of the comprehensive EMR system helps to enhance the security, performance and effectiveness of the health care system, as it contributes to enhancing patient safety by reducing the number of harmful drug adverse events, and choosing the safest treatment that is appropriate to the patient’s history.
The final fourth result which showed the significant positive relationship between comprehensive EMR and production efficiency in an advanced tertiary care setting in KAMC Saudi Arabia can be demonstrated by the fact that the utilization of comprehensive EMR in KAMC contributes to reducing the costs as it enables healthcare workers to have many access to records from various sites and organizational units, which means that the time for presenting the patient's medical report will be reduced, which will be enhanced in corresponding efficiency, enhances the level of service, and improves patient flow in the hospital, which was emphasized in the study Gastaldi et al. 38. Furthermore, there is a consistency between this result and the study of Lin et al. 37 and Waithera et al. 6 who showed that comprehensive EMR implementation in hospitals has contributed to reducing stay time and mortality, and it also contributes in increasing healthcare efficiency, improving clinical decision-making, and enhancing cooperation between healthcare providers, which demonstrates the strong relationship between the use of comprehensive records and production efficiency.
In light of the positive results shown in thus study, a number of recommendations are felt to be worth considering. Firstly, public and private hospitals in the Kingdom of Saudi Arabia must pay attention to the necessity of activating and adopting modern EMR systems because of their role in developing hospital performance and improving patients' health. A multi-level confidentiality EMR system is highly recommended so that health service providers can access patient information related to their responsibilities while preventing access to confidential data that is not supposed to be seen by other stakeholders. Moreover, health policy makers should consider a higher level strategy that involves connecting hospitals with each other through a computerized health information system and building an integrated comprehensive EMR system at the level of the Kingdom that ensures safe exchange of information between hospitals and various health and national centers through a unified health number for each patient. This will raise the value of health services as a whole and will provide a more distinguished health service for each patient, increase administrative efficiency, facilitates the transfer of patients between hospitals and reduce the use of traditional means of recording like paper. Finally, there should be a regular maintenance checkup of the EMR to ensure its reliability and accuracy in addition to a well-documented contingency plan that prevents frustrating scenarios in cases where the systems fail. Therefore, the government should invest in comprehensive training for both information technology (IT) professionals and clinicians to allow for the successful integration of systems and healthcare.
The study concluded that there is a significant positive relationship between comprehensive EMR and clinical effectiveness in an advanced tertiary care setting in Saudi Arabia. There was also increase in the level of patient-centeredness and patient safety after the implementation of such an advanced EMR. Moreover, the production efficiency significantly improved in KAMC after replacing the old EMR with the new comprehensive technology.
The study also revealed that the implementation of EMR in KAMC came with a number of advantages. The EMR system makes the doctor's workflow very simplified through automation and increase in efficiency as one avoids the difficulty of fumbling through paper medical records that do not provide consistent information on patients' medical history. It monitors, records, and creates accurate information about patients' progress while proposing feasible solutions to recurrent or persistent symptoms which consequently leads to the achievement of clinical effectiveness, patient-centeredness, patients’ safety and production efficiency.
This study may benefit policy-makers in the Saudi government by contributing to the development of policies, systems and frameworks that motivate hospitals to implement and adopt modern information technologies, including comprehensive EMR, because of their role in ensuring the efficiency of clinical care and patient safety, eliminating medical errors, and raising the quality of healthcare outputs. This study will draw the attention of officials in the Saudi Ministry of Health to the need to increase budget allocations for public hospitals to support the implementation of comprehensive EMR, In addition to supporting and creating a wide environment that encourages private hospitals to implement such a system.
Although this study took an important step towards a deeper understanding about the relationship between comprehensive EMR application and its impact on hospital performance especially in the advanced tertiary care setting, there are some limitations of the research which are illustrated as follows:
- This research is a single case study within one hospital in the Kingdom of Saudi Arabia, which is King Abdullah Medical City, and this may reduce the possibility of generalizing these results to all hospitals in the Kingdom.
- The quantitative approach only was relied upon in this study. This approach does not give clarification or deep details about the research topic or give an impression of the respondents’ feelings and perspectives related to it as is the case in the qualitative research. Therefore, for getting deeper and more detailed results, the mixed (triangulation) method is preferable for future.
Based on the findings and limitations of this research, there are opportunities for future research including:
1) Future research may look at multiple case studies and include hospitals in different governorates in the Saudi Kingdom, such as Riyadh, Dammam, and others, in a manner that ensures validation and generalization of the proposed methodology and results.
2) Conducting studies of a comparative nature, for example, to compare health services institutions in different environments and countries and investigate the extent of their reliance and benefiting from comprehensive EMR.
3) It is recommended to conduct a similar study on a government hospital and its branches, and a private hospital and its branches to compare the extent of each of them to implement electronic health (e-health) system and the size of the gap between the two sectors in the application of EMRs.
4) Researching the obstacles and factors that prevent all hospitals and health care departments in the Kingdom from adopting EMRs.
| [1] | Kwan J, Lo L, Ferguson J, Goldberg H, Diaz-Martinez J, Tomlinson G et al. Computerised clinical decision support systems and absolute improvements in care: meta-analysis of controlled clinical trials. BMJ. 2020; 370 :m3216. | ||
| In article | View Article PubMed | ||
| [2] | Mahmoudi E, Kamdar N, Kim N, Gonzales G, Singh K, Waljee A et al. Use of electronic medical records in development and validation of risk prediction models of hospital readmission: systematic review. BMJ. 2020; 369: m958. | ||
| In article | View Article PubMed | ||
| [3] | The National Alliance for Health Information Technology (NAHIT). | ||
| In article | |||
| [4] | Lee J, Kuo YF, & Goodwin J. The effect of electronic medical record adoption on outcomes in US hospitals. BMC Health Services Research. 2013; 13:39. | ||
| In article | View Article PubMed | ||
| [5] | Gardner J, Boyer K, & Gray J. Operational and strategic information processing: Complementing healthcare IT infrastructure. Journal of Operations Management. 2015; 33-34: 123-129. | ||
| In article | View Article | ||
| [6] | Waithera L, Muhia, J, & Songole R. Impact of Electronic Medical Records on Healthcare Delivery in Kisii Teaching and Referral Hospital. Medical & Clinical Reviews. 2017; 03(04): 1-7. | ||
| In article | View Article | ||
| [7] | Jha A, DesRoches C, Campbell E, Donelan K, Rao S, Ferris T, et al. Use of electronic health records in US hospitals. New England Journal of Medicine. 2009; 360(16): 1628-1638. | ||
| In article | View Article PubMed | ||
| [8] | Campanella P, Lovato E, Marone C, & Fallacara L. The Impact of Electronic Health Records on Healthcare Quality: A Systematic Review and Meta-analysis. The European Journal of Public Health. 2016; 26(1): 60-64. | ||
| In article | View Article PubMed | ||
| [9] | Colicchio T, Fiol G, Stoddard G & Narus S. Evaluation of a systematic methodology to detect in near real-time performance changes during electronic health record system implementations: a longitudinal study. AMIA Annu Symp Proc. 2018; 2017: 595-604. | ||
| In article | |||
| [10] | Appari A, Johnson M & Anthony D (2013). Meaningful Use of Electronic Health Record Systems and Process Quality of Care: Evidence From a Panel Data Analysis of U.S. Acute-Care Hospitals. Health Services Research. 2013; 48(2 Pt 1): 354-375. | ||
| In article | View Article PubMed | ||
| [11] | Adler-Milstein J, Scott K, Jha A. Leveraging EHRs to improve hospital performance: the role of management. Am J Manag Care. 2014; 20(11 Spec No. 17):SP511-SP519. | ||
| In article | |||
| [12] | DesRoches C, Campbell E, Vogeli C, Zheng J, Rao S, Shields A, et al. Electronic Health Records’ Limited Successes Suggest More Targeted Uses. Health Affairs. 2010; 29(4): 639-646. | ||
| In article | View Article PubMed | ||
| [13] | Noraziani K, Ain A, Azhim M, Eslami S, Drak B, WP S, et al. An Overview of Electronic Medical Record Implementation in Healthcare System: Lesson to Learn. World Applied Sciences Journal. 2013; 25(2): 323-332. | ||
| In article | |||
| [14] | Bain C. The Implementation of the Electronic Medical Records System in Health Care Facilities. Procedia Mnufacturing. 2015; 3: 4629-4634. | ||
| In article | View Article | ||
| [15] | NHS Executive (1996) Promoting Clinical Effectiveness: A Framework for Action in and Through the Nhs. | ||
| In article | |||
| [16] | Kalra S, Baruah M & Unnikrishnan A. Responsible Patient-centered Care. Indian J Endocrinol Metab. 2017; 21(3): 365-366. | ||
| In article | View Article PubMed | ||
| [17] | World health organization. (2018). Patient safety Global action on patient safety Report by the Director-General of world health organization. | ||
| In article | |||
| [18] | Chappelow J (2019). Production Efficiency. Investopedia. | ||
| In article | |||
| [19] | Bryman A & Bell E (2007). Business research methods. Oxford university press. | ||
| In article | |||
| [20] | Rawbone R. Doing a Successful Research Project—Using Qualitative or Quantitative Methods. Occupational Medicine. 2015; 65(2): 169-170. | ||
| In article | View Article | ||
| [21] | Leedy P & Ormrod J (2005). Practical Research: Planning and Design. Prentice Hall, Upper Saddle River, NJ. | ||
| In article | |||
| [22] | Gupta S & Shabbir J. On improvement in estimating the population mean in simple random sampling. Journal of Applied Statistics. 2008; 35(5): 559-566. | ||
| In article | View Article | ||
| [23] | Martínez-Mesa J, González-Chica D, Duquia R , Bonamigo R & Bastos J. Sampling: how to select participants in my research study?. Anais brasileiros de dermatologia. 2016; 91(3): 326-330. | ||
| In article | View Article PubMed | ||
| [24] | Krejcie R & Morgan D. Determining sample size for research activities. Educational and psychological measurement. 1970; 30(3):607-610. | ||
| In article | View Article | ||
| [25] | Karen Lowing (2011) Educational Research and Inquiry: Qualitative and Quantitative Approaches. Edited by D. Hartas, British Journal of Educational Studies. 2011; 59(3): 350-351. | ||
| In article | View Article | ||
| [26] | Al-Mujaini A, Al-Farsi Y, Al-Maniri A & Ganesh A. Satisfaction and perceived quality of an electronic medical record system in a tertiary hospital in Oman. Oman medical journal. 2011; 26(5): 324-328. | ||
| In article | View Article PubMed | ||
| [27] | Aldosari B, Al-Mansour S, Aldosari H & Alanazi A. Assessment of factors influencing nurses acceptance of electronic medical record in a Saudi Arabia hospital. Informatics in Medicine Unlocked. 2018; 10: 82-88. | ||
| In article | View Article | ||
| [28] | Otieno O, Toyama H, Asonuma M, Kanai‐Pak M & Naitoh K. Nurses’ views on the use, quality and user satisfaction with electronic medical records: questionnaire development. Journal of Advanced Nursing. 2007; 60(2): 209-219. | ||
| In article | View Article PubMed | ||
| [29] | Graham J. Congeneric and (essentially) tau-equivalent estimates of score reliability: What they are and how to use them. Educational and psychological measurement. 2006; 66(6): 930-944. | ||
| In article | View Article | ||
| [30] | Dobronte A (2013). The importance of socio-demographics in online surveys. Check Market. | ||
| In article | |||
| [31] | Yanamadala S, Morrison D, Curtin C, McDonald K & Hernandez-Boussard T. Electronic Health Records and Quality of Care. Medicine. 2016; 95(19): e3332. | ||
| In article | View Article PubMed | ||
| [32] | Kaneko K, Onozuka D, Shibuta H & Hagihara A. Impact of electronic medical records (EMRs) on hospital productivity in Japan. International Journal of Medical Informatics. 2018; 118: 36-43. | ||
| In article | View Article PubMed | ||
| [33] | Hasanain R, Vallmuur K, and Clark M. “Electronic Medical Record Systems in Saudi Arabia: Knowledge and Preferences of Healthcare Professionals”, Health Informatics Journal. 2015; 9(1): 23-31. | ||
| In article | |||
| [34] | Adler-Milstein J, Everson J, Lee SY. EHR Adoption and Hospital Performance: Time-Related Effects. Health Serv Res. 2015; 50(6): 1751-1771. | ||
| In article | View Article PubMed | ||
| [35] | Aldebasi B, Alhassan A, Al-Nasser S & Abolfotouh M. Level of awareness of Saudi medical students of the internet-based health-related information seeking and developing to support health services. BMC Medical Informatics and Decision Making. 2020; 20(1): 1-8. | ||
| In article | View Article PubMed | ||
| [36] | Ariffin N, Ismail A, Kadir I & Kamal J (2018). Implementation of Electronic Medical Records in Developing Countries: Challenges & Barriers. International Journal of Academic Research in Progressive Education and Development. 2018; 7(3): 187-199. | ||
| In article | View Article | ||
| [37] | Lin HL, Wu DC, Cheng SM, Chen CJ, Wang MC, Cheng CA. Association between Electronic Medical Records and Healthcare Quality. Medicine (Baltimore). 2020; 99(31):e21182. | ||
| In article | View Article PubMed | ||
| [38] | Gastaldi L, Lettieri E, Corso M & Masella C. Performance improvement in hospitals: leveraging on knowledge asset dynamics through the introduction of an electronic medical record. Measuring Business Excellence. 2012; 16 (4): 14-30. | ||
| In article | View Article | ||
Published with license by Science and Education Publishing, Copyright © 2021 Mohammad Mahal Alrehaili and Omar Zayyan Alsharqi
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Kwan J, Lo L, Ferguson J, Goldberg H, Diaz-Martinez J, Tomlinson G et al. Computerised clinical decision support systems and absolute improvements in care: meta-analysis of controlled clinical trials. BMJ. 2020; 370 :m3216. | ||
| In article | View Article PubMed | ||
| [2] | Mahmoudi E, Kamdar N, Kim N, Gonzales G, Singh K, Waljee A et al. Use of electronic medical records in development and validation of risk prediction models of hospital readmission: systematic review. BMJ. 2020; 369: m958. | ||
| In article | View Article PubMed | ||
| [3] | The National Alliance for Health Information Technology (NAHIT). | ||
| In article | |||
| [4] | Lee J, Kuo YF, & Goodwin J. The effect of electronic medical record adoption on outcomes in US hospitals. BMC Health Services Research. 2013; 13:39. | ||
| In article | View Article PubMed | ||
| [5] | Gardner J, Boyer K, & Gray J. Operational and strategic information processing: Complementing healthcare IT infrastructure. Journal of Operations Management. 2015; 33-34: 123-129. | ||
| In article | View Article | ||
| [6] | Waithera L, Muhia, J, & Songole R. Impact of Electronic Medical Records on Healthcare Delivery in Kisii Teaching and Referral Hospital. Medical & Clinical Reviews. 2017; 03(04): 1-7. | ||
| In article | View Article | ||
| [7] | Jha A, DesRoches C, Campbell E, Donelan K, Rao S, Ferris T, et al. Use of electronic health records in US hospitals. New England Journal of Medicine. 2009; 360(16): 1628-1638. | ||
| In article | View Article PubMed | ||
| [8] | Campanella P, Lovato E, Marone C, & Fallacara L. The Impact of Electronic Health Records on Healthcare Quality: A Systematic Review and Meta-analysis. The European Journal of Public Health. 2016; 26(1): 60-64. | ||
| In article | View Article PubMed | ||
| [9] | Colicchio T, Fiol G, Stoddard G & Narus S. Evaluation of a systematic methodology to detect in near real-time performance changes during electronic health record system implementations: a longitudinal study. AMIA Annu Symp Proc. 2018; 2017: 595-604. | ||
| In article | |||
| [10] | Appari A, Johnson M & Anthony D (2013). Meaningful Use of Electronic Health Record Systems and Process Quality of Care: Evidence From a Panel Data Analysis of U.S. Acute-Care Hospitals. Health Services Research. 2013; 48(2 Pt 1): 354-375. | ||
| In article | View Article PubMed | ||
| [11] | Adler-Milstein J, Scott K, Jha A. Leveraging EHRs to improve hospital performance: the role of management. Am J Manag Care. 2014; 20(11 Spec No. 17):SP511-SP519. | ||
| In article | |||
| [12] | DesRoches C, Campbell E, Vogeli C, Zheng J, Rao S, Shields A, et al. Electronic Health Records’ Limited Successes Suggest More Targeted Uses. Health Affairs. 2010; 29(4): 639-646. | ||
| In article | View Article PubMed | ||
| [13] | Noraziani K, Ain A, Azhim M, Eslami S, Drak B, WP S, et al. An Overview of Electronic Medical Record Implementation in Healthcare System: Lesson to Learn. World Applied Sciences Journal. 2013; 25(2): 323-332. | ||
| In article | |||
| [14] | Bain C. The Implementation of the Electronic Medical Records System in Health Care Facilities. Procedia Mnufacturing. 2015; 3: 4629-4634. | ||
| In article | View Article | ||
| [15] | NHS Executive (1996) Promoting Clinical Effectiveness: A Framework for Action in and Through the Nhs. | ||
| In article | |||
| [16] | Kalra S, Baruah M & Unnikrishnan A. Responsible Patient-centered Care. Indian J Endocrinol Metab. 2017; 21(3): 365-366. | ||
| In article | View Article PubMed | ||
| [17] | World health organization. (2018). Patient safety Global action on patient safety Report by the Director-General of world health organization. | ||
| In article | |||
| [18] | Chappelow J (2019). Production Efficiency. Investopedia. | ||
| In article | |||
| [19] | Bryman A & Bell E (2007). Business research methods. Oxford university press. | ||
| In article | |||
| [20] | Rawbone R. Doing a Successful Research Project—Using Qualitative or Quantitative Methods. Occupational Medicine. 2015; 65(2): 169-170. | ||
| In article | View Article | ||
| [21] | Leedy P & Ormrod J (2005). Practical Research: Planning and Design. Prentice Hall, Upper Saddle River, NJ. | ||
| In article | |||
| [22] | Gupta S & Shabbir J. On improvement in estimating the population mean in simple random sampling. Journal of Applied Statistics. 2008; 35(5): 559-566. | ||
| In article | View Article | ||
| [23] | Martínez-Mesa J, González-Chica D, Duquia R , Bonamigo R & Bastos J. Sampling: how to select participants in my research study?. Anais brasileiros de dermatologia. 2016; 91(3): 326-330. | ||
| In article | View Article PubMed | ||
| [24] | Krejcie R & Morgan D. Determining sample size for research activities. Educational and psychological measurement. 1970; 30(3):607-610. | ||
| In article | View Article | ||
| [25] | Karen Lowing (2011) Educational Research and Inquiry: Qualitative and Quantitative Approaches. Edited by D. Hartas, British Journal of Educational Studies. 2011; 59(3): 350-351. | ||
| In article | View Article | ||
| [26] | Al-Mujaini A, Al-Farsi Y, Al-Maniri A & Ganesh A. Satisfaction and perceived quality of an electronic medical record system in a tertiary hospital in Oman. Oman medical journal. 2011; 26(5): 324-328. | ||
| In article | View Article PubMed | ||
| [27] | Aldosari B, Al-Mansour S, Aldosari H & Alanazi A. Assessment of factors influencing nurses acceptance of electronic medical record in a Saudi Arabia hospital. Informatics in Medicine Unlocked. 2018; 10: 82-88. | ||
| In article | View Article | ||
| [28] | Otieno O, Toyama H, Asonuma M, Kanai‐Pak M & Naitoh K. Nurses’ views on the use, quality and user satisfaction with electronic medical records: questionnaire development. Journal of Advanced Nursing. 2007; 60(2): 209-219. | ||
| In article | View Article PubMed | ||
| [29] | Graham J. Congeneric and (essentially) tau-equivalent estimates of score reliability: What they are and how to use them. Educational and psychological measurement. 2006; 66(6): 930-944. | ||
| In article | View Article | ||
| [30] | Dobronte A (2013). The importance of socio-demographics in online surveys. Check Market. | ||
| In article | |||
| [31] | Yanamadala S, Morrison D, Curtin C, McDonald K & Hernandez-Boussard T. Electronic Health Records and Quality of Care. Medicine. 2016; 95(19): e3332. | ||
| In article | View Article PubMed | ||
| [32] | Kaneko K, Onozuka D, Shibuta H & Hagihara A. Impact of electronic medical records (EMRs) on hospital productivity in Japan. International Journal of Medical Informatics. 2018; 118: 36-43. | ||
| In article | View Article PubMed | ||
| [33] | Hasanain R, Vallmuur K, and Clark M. “Electronic Medical Record Systems in Saudi Arabia: Knowledge and Preferences of Healthcare Professionals”, Health Informatics Journal. 2015; 9(1): 23-31. | ||
| In article | |||
| [34] | Adler-Milstein J, Everson J, Lee SY. EHR Adoption and Hospital Performance: Time-Related Effects. Health Serv Res. 2015; 50(6): 1751-1771. | ||
| In article | View Article PubMed | ||
| [35] | Aldebasi B, Alhassan A, Al-Nasser S & Abolfotouh M. Level of awareness of Saudi medical students of the internet-based health-related information seeking and developing to support health services. BMC Medical Informatics and Decision Making. 2020; 20(1): 1-8. | ||
| In article | View Article PubMed | ||
| [36] | Ariffin N, Ismail A, Kadir I & Kamal J (2018). Implementation of Electronic Medical Records in Developing Countries: Challenges & Barriers. International Journal of Academic Research in Progressive Education and Development. 2018; 7(3): 187-199. | ||
| In article | View Article | ||
| [37] | Lin HL, Wu DC, Cheng SM, Chen CJ, Wang MC, Cheng CA. Association between Electronic Medical Records and Healthcare Quality. Medicine (Baltimore). 2020; 99(31):e21182. | ||
| In article | View Article PubMed | ||
| [38] | Gastaldi L, Lettieri E, Corso M & Masella C. Performance improvement in hospitals: leveraging on knowledge asset dynamics through the introduction of an electronic medical record. Measuring Business Excellence. 2012; 16 (4): 14-30. | ||
| In article | View Article | ||