Persons diagnosed with a terminal illness are faced with a panoply of arduous challenges and decisions that intrinsically affect their quality of life. Terminal patients have the option to end their life under the auspices of Physician-assisted suicide (PAS) in ten states and the District of Columbia. Physician-assisted suicide can be described as a physician facilitating a patient’s death by providing the necessary means and/or information to enable the patient to perform the life ending act. States that allow PAS include California, Colorado, Hawaii, Maine, Montana, New Jersey, New Mexico, Oregon, Vermont, and Washington. A logistic regression study was conducted to investigate factors that may impact PAS laws including Catholicism, cancer mortality rate, pancreatic cancer rate, cervical cancer rate, colon cancer rate, brain cancer rate, leukemia, and liver cancer rate. The unit of analysis was state. Statistical significance was found with the liver cancer and cervical cancer rates (P<.05). This paper delineates PAS state laws and provides insight for the origins of laws, timelines, and moral discourse.
Physician-assisted suicide (PAS) can be described as a physician facilitating a patient’s death by providing the necessary means and/or information to enable the patient to perform the life-ending act 1. Origins of state laws codifying PAS begin with the landmark Supreme Court case Washington v. Glucksberg (1997). In this case, four physicians and three terminally ill patients challenged the state of Washington’s ban on PAS claiming it was unconstitutional toward the Fourteenth Amendment’s Due Process Clause in denying terminally ill adults who are competent the liberty of choosing death over life 2. At the time, the state of Washington deemed PAS a felony. The court ruled unanimously in favor of Washington state positing that PAS is not a fundamental liberty interest protected by the Due Process Clause as PAS is offensive to national traditions and practices; in addition, the ban was rationally related to the state’s legitimate interest in the protection of medical ethics and patients who may be influenced from outside parties to end their life. This decision promulgated PAS policies at the state's discretion.
The first state to pass a law allowing PAS was Oregon in 1997. The Death with Dignity Act passed with fifty-one percent of the electorate voting in favor of PAS. An adult (≥18 years) who is a suffering from a terminal disease and has consulted with a physician expressing their wish to end their life may voluntarily make a written request for medication for the purpose of ending his or her life in a humane manner. At least two witnesses must attest that the adult is capable of making an informed decision, and acting voluntarily 3. Washington state passed its PAS law in 2008. The Death with Dignity Act passed with over fifty-seven percent of the electorate in favor of the law 4. Montana does not have a law on PAS however a physician cannot be prosecuted for participating in PAS due to a Supreme Court ruling in Baxter v. Montana (2009). This case involved Robert Baxter who was diagnosed with terminal lymphocytic leukemia. Mr. Baxter wished to end his life by self-administration of a lethal dose of medication prescribed by his physician. His physicians filed suit against the state of Montana to protect themselves against criminal prosecution. The Court ruled in favor of the physicians asserting that a physician(s) aiding their terminally ill patient in ending their life does not violate public policy, and further that terminally ill patients are entitled to autonomous end-of-life decisions 5. In 2013, Vermont enacted the Patient Choice and Control at End-of-Life Act 6. In New Mexico, Morris v. Brandenburg 7 was brought before the District Court to adjudicate a person’s right to die. The case plaintiffs (Dr. Katherine Morris, Dr. Aroop Mangalik, Aja Riggs) filed suit against the state to avoid criminal liability of physicians who provided aid to Aja Riggs in assisted suicide; the patient, Aja Riggs, was diagnosed with terminal uterine cancer. The state’s case rested on a statute [NM 30-2-4] that charged persons with a fourth-degree felony for assisting in suicide. The District Court ruled in favor of the plaintiffs referencing the New Mexico Constitution’s clause of life, liberty, and seeking and obtaining happiness. The Court of Appeals reversed the District Courts decision. The plaintiffs proceeded with filing a Writ of Certiorari in 2016 to the New Mexico Supreme Court who upheld the Court of Appeals decision. In 2021, the New Mexico legislature passed the Elizabeth Whitfield End-of-Life Options Act 8 making medical aid available for terminally ill patients who chose to end their life.
In 2015, California legalized PAS through the End of Life Option Act 9. Citizens of California and legislators were persuaded to favor a policy of providing medical aid in assisted suicide when a 29-year-old woman with brain cancer moved from California to Oregon to end her life legally through PAS. Brittany Maynard learned she had a fatal brain tumor on New Year's Day 2014. Her story and fervor for change in laws elicited vigorous civic action among Californians toward support of a PAS law 10. The End of Life Options Act 11 was passed in Colorado in 2016. In 2017, the District of Columbia’s Death with Dignity Act 12 was adopted. Voters in Hawaii voted in favor of Our Care Our Choice Act 13 in 2018, and a year later New Jersey 14 and Maine 15 passed legislation legalizing PAS, adopting many of the same guidelines in other state laws. There are many similar characteristics of laws across the states and District of Columbia such as patients can rescind their request at any time, physicians are not required to participate in PAS, and patients must be assessed for being competent and devoid of psychological disorders in making their decision. Differences are evident in Colorado, Hawaii, New Mexico, and Maine where two medical opinions for the patient’s terminal illness are required; in addition, New Mexico is the only state in which a physician assistant or nurse practitioner may serve as one of the two clinicians to confirm the diagnosis; New Mexico also does not require witnesses. Characteristics of laws are depicted in Table 1 and an example request for PAS is illustrated in Figure 1.
Factors that may lead a person to choose PAS include debilitating manifestations of their illness, perpetual pain and suffering, depression, diminished quality of life, and financial strain. The aim of this study is to identify factors linked to medicine and religion that impact PAS laws in the United States. Catholicism, cancer mortality rate, and a multitude of different types of cancer rates were variables selected in determining an effect on PAS policies. Information gleaned from this study may provide insight into what factors may be directly associated or inversely associated with PAS.
A binary logistic regression analysis was conducted using PAS laws as the dependent variable, coded 1 for states legalizing PAS and 0 for states devoid of a law. Montana was coded 1 from the perspective that a physician cannot be prosecuted for facilitating PAS. All fifty states were included in the sample. The independent variables were liver cancer rate, cervical cancer rate, pancreatic cancer rate, brain cancer rate, leukemia rate, colon cancer rate, cancer mortality rate, and percent of Catholics in each state. The source used for the select cancer rates was the NIH National Cancer Institute (2015-2019), and data for the cancer mortality rate was accessed from the CDC (2020). Data for the percentage of Catholics in each state was retrieved from the Pew Research Center (2014). Statistical significance is evident with P<.05. Binary logistic regression performed using SPSS (v26).
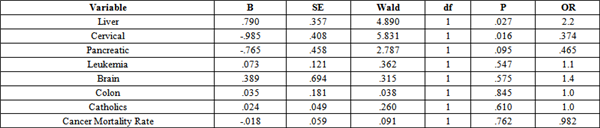
Statistical significance was found with the liver cancer rate and cervical cancer rate variables; the former represented a direct relationship and the latter an inverse relationship. The odds ratio (OR) for the liver cancer rate variable was 2.2, and 0.374 for cervical cancer rate. These findings can further be interpreted as the odds of a state having a law allowing PAS increases by a factor of 2.2 with a one unit increase in the liver cancer rate, and the odds of a state having a law allowing PAS decreases by a factor of .376 with a one unit increase in the cervical cancer rate. All other independent variables were not statistically significant (Table 2).
This study analyzed select cancer rates, cancer mortality rates, and Catholicism effect on PAS Policies in the United States. Variables that were determined to be statistically significant were liver cancer and cervical cancer rates. For the states that permit PAS the range and mean of liver cancer rates was 5.4 to 10.6, mean 8.23, and range of cervical cancer rates was 3.9 to 8.5, mean 6.7. In 2015, Le Strat et al conducted a cross-sectional study evaluating data from the National Epidemiologic Survey of Alcohol and Related Conditions (NESARC). This survey represented 43,093 adults aged 18 and over who participated in a face-to-face survey assessing liver disease, major depression, and suicide attempts. Responses from the survey were checked against the participant's medical records. Their findings included a significant association between liver disease and major depression, and a strong odds ratio, 3.1, between liver disease and attempting suicide employing multivariate logistic regression 16. In 2010, Karaivazoglou et al, assessed quality of life indicators in patients with chronic viral hepatitis. They found statistical significance with depression, higher inflammation grade, higher fibrosis stage, and fatigue 17. Fang et al (2010) evaluated data from more than six million persons in Sweden between 1991 and 2006, and found that 26,335 citizens had a diagnosis of liver cancer, esophageal cancer, or pancreatic cancer. The relative risk of suicide for this aggregate within 1 to 12 weeks, 13 to 52 weeks, or more than 52 weeks of diagnosis was 16, 5.2, and 4.5, respectively 18. Violette et al (2019) evaluated characteristics of women with gynecological malignancies who committed suicide through a retrospective study from 1973 to 2013 using the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results Program) database. Malignancies included cervical, ovarian, and uterine cancer. During the study period there were 87,151 women diagnosed with cervical cancer, 133,481 diagnosed with ovarian cancer, and 246,736 diagnosed with uterine cancer; investigators found a decrease in suicide rates across the three malignancies over time, 78.1%, 73.6%, and 88.2%, respectively 19. It was posited that improvements in treatment and clinicians being more aware of the mental illness associated with gynecological malignancies may help to explain the decrease in suicide rates. These studies illuminate reasons why patients with liver cancer may choose PAS, and in addition show, there has been a downward trend in suicide for patients with cervical cancer employing the largest population-based tumor registry in the United States [SEER].
A person’s religious affiliation may serve as their moral compass in formulating an opinion on PAS. In 2020, the United States Conference of Catholic Bishops Secretariat of Pro-Life Activities published Samaritanus bonus outlining the Roman Catholic Church’s position on PAS and euthanasia. The bishops emphasize that the first responsibility of physicians is to care for the life of their patients even when faced with an incurable disease; “therapeutic art, clinical procedures, and ongoing care are in separately interwoven in the practice of medicine” 20. They also reference Christ’s pain and how his suffering [an unwavering hope] resonates with every sick person in combating their illness. John Paul II framed euthanasia and PAS as a culture of death serving as erroneous solutions to the human and Christian act of caring for terminally ill patients. Pope Francis described PAS as a ‘false compassion’ diverting from a person’s dignity and a person’s freedom; in essence physicians are discarding the patient. Moreover, he stated in reference to the definition of medicine “is service to human life, and as such it involves an essential and inalienable reference to the person in his spiritual and material integrity, in his individual and social dimension.” 21
In Judaism, the Torah exclaims that people are not the owners of their body, but that it belongs to God 22. Taking a human life is forbidden regardless if it is someone else’s or a person’s own life. In the Jewish culture, practicing medicine is viewed as being an agent of God, imparting great reverence to the medical profession. Shimon Glick, a physician, and professor at Ben-Gurion University of the Negev, stated the nexus of autonomy [respective of competence], patient-centered care, and community may be the most salient entities that sway the pendulum on PAS 23. Autonomy can be viewed as moving away from authority and rendering the best decisions on one’s life with thorough deliberation, particularly in the medical sphere where clinicians provide current knowledge on treatments [evidenced-based] and patients make their own decision on whether to undergo such treatment (s). Patient-centered medicine as opposed to physician-centered medicine can be interpreted as patient’s wishes superseding the paradigm that the physician is the sole arbiter of the patient’s course of treatment. Society today is well aware that not all physicians are competent leading patients to investigate on their own advantages and disadvantages of various treatment modalities. On the topic of community, the Talmud states that all Jews are responsible for each other. In Jewish communities the Rabbi can have an equivocal role on medical-ethical issues, offering halachic guidance and pastoral support to both the patient and physician (s) in deliberating end-of-life decisions 23. Hence, in Jewish culture, many persons, factors, and entities may play a role in a person’s decision on PAS.
Protestants may be characterized as conservative, moderate, or liberal. Conservative Protestants have been described as biblical literalists holding the posture that PAS is a direct contraindication to biblical scripture on the sanctity of life. In contrast, moderate and liberal Protestants deviate from viewing the Bible as the literal word of God and have more understanding of societal undulations and human suffering. In 2005, Burdette et al conducted a study assessing differences in attitudes toward PAS and terminal palliative care. The latter can be described as treatment given to the patient, typically in a hospice facility, to control symptoms of the terminal illness, without addressing the underlying cause of the illness 24. In this study, the 1998 General Social Survey data was employed to make comparisons on attitudes of religious affiliates (Protestant and Catholic) to nonaffiliates. Their findings revealed that all groups exhibited a greater opposition to PAS compared to terminal palliative care; conservative Protestants exhibited the highest degree of opposition to PAS followed by moderate Protestants, Catholics, and liberal Protestants. They also posited that the degree of opposition to PAS may be predicated on church attendance and stronger religious involvement on the part of parishioners 24. While religion in the current study was limited to the Catholic denomination, the variable was not statistically significant. It is unlikely the Pope, Bishops, and other clergies will change their position on PAS. In reference to parishioners, recent polls have indicated that Catholics have been more accepting of other polarizing social and moral issues such as same-sex marriage and abortion, and moreover that the church does not imbue great influence over their political views. This trend could extend to acceptance of PAS or at a minimum not being critical of PAS 25. Other variables that were not statistically significant included pancreatic cancer, brain cancer, leukemia, colon cancer, and cancer mortality rate.
In 1996, Weiss et al conducted a study analyzing attitudes of college students using multiple regression 26. The sample consisted of 200 full-time students attending a liberal arts college. Variables included religiosity, gender, GPA, interaction, discussion, media, and autonomy. Religiosity and autonomy were statistically significant, with the former demonstrating an inverse relationship and the latter a direct relationship. Students who identified as being very religious were not supportive of PAS compared to students who were not very religious. Students who were supportive of autonomy tended to be in favor of PAS. In 2016, Frey and Hans conducted a study where 272 persons were interviewed to assess six variables (gender, age, type of illness, relationship status, parenthood status, and family support) in a logistic regression analysis 27. A patient vignette was articulated to participants and then asked if they would be in favor of PAS in that medical circumstance. Results indicated that respondents were twice as likely to be in favor of PAS when the patient was elderly and suffering from physical pain as opposed to depression. The specific type of illness such as liver cancer or leukemia was not assessed, only physical pain as a result of the illness. In 2008, Curlin et al conducted a study investigating the association between objections to PAS by US physicians and their religious preference 28. A 12-page questionnaire was sent to 2000 US practicing physicians in a variety of specialties. Respondents (n = 1144) identified as 38 percent Protestant, 24 percent Catholic, 16 percent Jewish, 5 percent Hindu, 3 percent Muslim, and 10 percent specified no affiliation. Results showed that physicians with high intrinsic religiosity were more than four times more likely to object to PAS compared to those with low intrinsic religiosity. Moreover, physicians that identified as Catholics were more opposed to PAS than any other religious denomination.
Arguments for the legalization of PAS include a duty to ease a person’s pain and respect their autonomy. Pain can involve not only physical pain but also emotional pain, depression, and anxiety. A person that once was self-sufficient finds themselves dependent on others, and dealing with unimaginable financial strain, interpersonal conflicts, and hopelessness; for most patients, this can be seen as existential suffering. Being prescribed medication that the patient administers themselves can be seen as an act of compassion that respects the patient’s choice with reverence for their autonomy for making the personal and private decision to end their life, without harming anyone else 29. In addition, legalization espouses standardization, transparency, and monitoring of PAS policies as well as the ability to gather data that may be used to revise policy and help patients.
Arguments against legalizing PAS relate to the clinicians’ ethos to ‘first do no harm’. When a patient is suffering from a debilitating incurable illness the physician should do everything they can medically to relieve symptoms; suffering with their patients engenders compassion and honors the Hippocratic Oath. Aiding a patient in suicide compromises the patient-physician relationship as well as undermines the ethos of the medical profession; the duty of beneficence and nonmaleficence is usurped for prescribing a medication that will end a patient’s life. From the medical profession’s perspective, physicians are moral agents with a purview that extends well beyond providers of service. Physicians don’t order tests or procedures that are not medically indicated, they don’t write illegal prescriptions, and they decline to engage in futile care 30. Death certificate requirements for PAS laws list the cause of death as the primary illness, e.g., cancer, not the ingestion of a lethal dose of medicine 31; this practice is an affront to medical accuracy and only adds to the ethical discourse. According to the American College of Physicians (ACP) if a patient is considering PAS the physician should first reassess how well the treatment plan is meeting the patient’s medical, social, psychological, and spiritual needs and fears; they should explore the reasons for the PAS option, work with the patient in understanding the meaning of PAS, keep dialogue open, and affirm that they will not abandon their patient. Additionally, discuss options for hospice care including care at home 32.
Balancing patient autonomy with medical beneficence in patients with a terminal disease is an arduous undertaking. Organizations like the ACP stand firm on their position against PAS that medicalization of death is not the answer and controlling the timing of a patient’s death has never been a goal of medicine. Physicians must examine all aspects of patient care end-of-life options and continue to cultivate the patient-physician relationship. Community resources, advances in treatment modalities, spiritual guidance, and patient family support should collectively be considered in navigating end-of-life issues. A physician’s decision to participate in PAS may be predicated on their religion, moral compass, state laws, and their own interpretation of the Hippocratic oath.
The limitation of this study was excluding the District of Columbia from the sample. The rationale for this was many of the independent variables did not include data for the District of Columbia.
This study assesses specific cancer rates and Catholicism's effects on the dependent variable, operationalized as a state having a law legalizing PAS or allowing PAS due to a court ruling or not having a law. The liver cancer rate and cervical cancer rate yielded statistically significant results with the former exhibiting a direct relationship and the latter an inverse relationship. In the sphere of politics, religion, and social mores PAS is wrought with controversy. The autonomy and dignity of persons with a terminal illness are cogent and reverent entities in navigating the pernicious path of end-of-life care. Palliative care in hospice centers is a formidable and vital service in the United States in aiding terminal patients in prioritizing comfort and reducing pain and suffering as well as tending to their emotional and spiritual needs. Through the legislative and judicial process, ten states and the District of Columbia have legalized PAS where strict medical and procedural criteria must be met for a patient to make the autonomous decision to end their life. The PAS laws are very similar in scope regarding physician responsibilities, psychological assessments, patient criteria for eligibility, witnesses, and documentation. The requirement of State health authorities to assimilate data on patient demographics, number of prescriptions written, hospice enrollment, and illness, and present it in a transparent manner engenders sharing of knowledge that can be shared and hopefully utilized by all persons and entities that are dedicated to serving patients, in all facets, of end-of-life care. Going forward investigators should consider analyzing PAS data from state health agencies to identify demographics and diseases that are associated with a preference for PAS over palliative care.
| [1] | https://www.ama-assn.org/delivering-care/ethics/physician-assisted-suicide. | ||
| In article | |||
| [2] | Washington v. Glucksberg, 521 U.S. 702 (1997). | ||
| In article | |||
| [3] | https://www.oregon.gov/oha/ph/providerpartnerresources/evaluationresearch/deathwithdignityact/pages/index.aspx. | ||
| In article | |||
| [4] | https://app.leg.wa.gov/rcw/default.aspx?cite=70.245. | ||
| In article | |||
| [5] | Baxter v. Montana. 224 P.3d 1211, 2009 MT 449. 354. Mont. 234, 2009. | ||
| In article | |||
| [6] | https://legislature.vermont.gov/statutes/fullchapter/18/113. | ||
| In article | |||
| [7] | Morris v. Brandenburg (2014). | ||
| In article | |||
| [8] | Elizabeth Whitefield End-of-Life Options Act 2021 HB47 New Mexico. | ||
| In article | |||
| [9] | AB-15 California End-of-Life Option Act 2015. | ||
| In article | |||
| [10] | https://www.nbcnews.com/health/health-news/death-dignity-advocate-brittany. | ||
| In article | |||
| [11] | https://leg.colorado.gov/bills/hb16-1054. | ||
| In article | |||
| [12] | https://dchealth.dc.gov/page/death-dignity-act-2016. | ||
| In article | |||
| [13] | https://health.hawaii.gov/opppd/ococ/. | ||
| In article | |||
| [14] | https://www.nj.gov/health/advancedirective/maid. | ||
| In article | |||
| [15] | https://legilature.maine.gov/legis/bills/bills_129th/chapters/PUBLIC271asp. | ||
| In article | |||
| [16] | Le Strat Y, Le Foll B, Dubertret C (2015). Major depression and suicide attempts in patients with liver disease in the United States. Liver Intl 35:7, 1910-1916. | ||
| In article | View Article PubMed | ||
| [17] | Karaivazoglou et al (2010). Fatigue and depressive symptoms associated with chronic viral hepatitis patients’ health-related qualify of life (HRQOL). Ann Hepatol 9(4):419-427. | ||
| In article | View Article PubMed | ||
| [18] | Fang, F et al (2012). Suicide and Cardiovascular Death after a cancer diagnosis. N Eng J Med 366 (14), 1310-1318. | ||
| In article | View Article PubMed | ||
| [19] | Violette CJ et al (2019). Temporal trends and characteristics of suicide among women with gynecologic malignancies in the United States. Gynecol Oncol Rep, 30:100510. | ||
| In article | View Article PubMed | ||
| [20] | https://www.usccb.org/resources/samaritanus-bonus-compendium.pdf. | ||
| In article | |||
| [21] | Brockhaus, H (2019).Pope Francis to doctors: Assisted suicide in ‘false compassion’. Catholic News Agency Sept 20. | ||
| In article | |||
| [22] | Lipner A. Of Life and Death: A Jewish response to Doctor Assisted Suicide. Institut for Jewish Medical Ethics of the Hebrew Academy of San Francisco. | ||
| In article | |||
| [23] | Glick SM (2001). Who decides- the patient, the physician, or the Rabbi? JAMA. | ||
| In article | |||
| [24] | Burdette AM, Hill TD, Moulton BC (2005). Religion and attitudes toward Physician Assisted Suicide and Terminal Palliative Care. J Sci Study Rel 44(1):79-93. | ||
| In article | View Article | ||
| [25] | Sullivan RD (2022). No confusion about a new poll: most US Catholics disagree with church leaders on abortion and LGBT issues. America The Jesuit Review. | ||
| In article | |||
| [26] | Weiss GL (1996). Attitudes of college students about physician-assisted suicide: the influence of life experiences, religiosity, and belief in autonomy. Death Stud 20(6):587-99. | ||
| In article | View Article PubMed | ||
| [27] | Frey LM, Hans JD (2016). Attitudes toward assisted suicide: Does family context matter? Arch Suicide Res 20(6):250-264. | ||
| In article | View Article PubMed | ||
| [28] | Curlin FA, Nwodim C, Vance JL, Chin MH, Lantos JD (2008). To Die to Sleep: US Physicians religious and other objections to Physican-assisted suicide, terminal sedation, and withdrawal of life support. Am J Hosp Palliat Care 25 (2):112-120. | ||
| In article | View Article PubMed | ||
| [29] | Brock DW (1992). Euthanasia. Yale J Biol Med 65:121-9. | ||
| In article | |||
| [30] | Snyder L, Sulmasy DP (2001). Physician-assisted suicide. Ann Intern Med 135(3): 209-16. | ||
| In article | View Article PubMed | ||
| [31] | Callahan D. Self-extinction: the morality of the helping hand, in Weir RF eds Physician Assisted Suicide. Bloomington IN: Univ Indiana 1997. | ||
| In article | |||
| [32] | Snyder L, Sulmasy DP (2017). Ethics and the legalization of Physician-Assisted Suicide: An American College of Physicians Position Paper. Ann Intern Med 167(8):576-578. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2023 Virginia C. Hughes
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | https://www.ama-assn.org/delivering-care/ethics/physician-assisted-suicide. | ||
| In article | |||
| [2] | Washington v. Glucksberg, 521 U.S. 702 (1997). | ||
| In article | |||
| [3] | https://www.oregon.gov/oha/ph/providerpartnerresources/evaluationresearch/deathwithdignityact/pages/index.aspx. | ||
| In article | |||
| [4] | https://app.leg.wa.gov/rcw/default.aspx?cite=70.245. | ||
| In article | |||
| [5] | Baxter v. Montana. 224 P.3d 1211, 2009 MT 449. 354. Mont. 234, 2009. | ||
| In article | |||
| [6] | https://legislature.vermont.gov/statutes/fullchapter/18/113. | ||
| In article | |||
| [7] | Morris v. Brandenburg (2014). | ||
| In article | |||
| [8] | Elizabeth Whitefield End-of-Life Options Act 2021 HB47 New Mexico. | ||
| In article | |||
| [9] | AB-15 California End-of-Life Option Act 2015. | ||
| In article | |||
| [10] | https://www.nbcnews.com/health/health-news/death-dignity-advocate-brittany. | ||
| In article | |||
| [11] | https://leg.colorado.gov/bills/hb16-1054. | ||
| In article | |||
| [12] | https://dchealth.dc.gov/page/death-dignity-act-2016. | ||
| In article | |||
| [13] | https://health.hawaii.gov/opppd/ococ/. | ||
| In article | |||
| [14] | https://www.nj.gov/health/advancedirective/maid. | ||
| In article | |||
| [15] | https://legilature.maine.gov/legis/bills/bills_129th/chapters/PUBLIC271asp. | ||
| In article | |||
| [16] | Le Strat Y, Le Foll B, Dubertret C (2015). Major depression and suicide attempts in patients with liver disease in the United States. Liver Intl 35:7, 1910-1916. | ||
| In article | View Article PubMed | ||
| [17] | Karaivazoglou et al (2010). Fatigue and depressive symptoms associated with chronic viral hepatitis patients’ health-related qualify of life (HRQOL). Ann Hepatol 9(4):419-427. | ||
| In article | View Article PubMed | ||
| [18] | Fang, F et al (2012). Suicide and Cardiovascular Death after a cancer diagnosis. N Eng J Med 366 (14), 1310-1318. | ||
| In article | View Article PubMed | ||
| [19] | Violette CJ et al (2019). Temporal trends and characteristics of suicide among women with gynecologic malignancies in the United States. Gynecol Oncol Rep, 30:100510. | ||
| In article | View Article PubMed | ||
| [20] | https://www.usccb.org/resources/samaritanus-bonus-compendium.pdf. | ||
| In article | |||
| [21] | Brockhaus, H (2019).Pope Francis to doctors: Assisted suicide in ‘false compassion’. Catholic News Agency Sept 20. | ||
| In article | |||
| [22] | Lipner A. Of Life and Death: A Jewish response to Doctor Assisted Suicide. Institut for Jewish Medical Ethics of the Hebrew Academy of San Francisco. | ||
| In article | |||
| [23] | Glick SM (2001). Who decides- the patient, the physician, or the Rabbi? JAMA. | ||
| In article | |||
| [24] | Burdette AM, Hill TD, Moulton BC (2005). Religion and attitudes toward Physician Assisted Suicide and Terminal Palliative Care. J Sci Study Rel 44(1):79-93. | ||
| In article | View Article | ||
| [25] | Sullivan RD (2022). No confusion about a new poll: most US Catholics disagree with church leaders on abortion and LGBT issues. America The Jesuit Review. | ||
| In article | |||
| [26] | Weiss GL (1996). Attitudes of college students about physician-assisted suicide: the influence of life experiences, religiosity, and belief in autonomy. Death Stud 20(6):587-99. | ||
| In article | View Article PubMed | ||
| [27] | Frey LM, Hans JD (2016). Attitudes toward assisted suicide: Does family context matter? Arch Suicide Res 20(6):250-264. | ||
| In article | View Article PubMed | ||
| [28] | Curlin FA, Nwodim C, Vance JL, Chin MH, Lantos JD (2008). To Die to Sleep: US Physicians religious and other objections to Physican-assisted suicide, terminal sedation, and withdrawal of life support. Am J Hosp Palliat Care 25 (2):112-120. | ||
| In article | View Article PubMed | ||
| [29] | Brock DW (1992). Euthanasia. Yale J Biol Med 65:121-9. | ||
| In article | |||
| [30] | Snyder L, Sulmasy DP (2001). Physician-assisted suicide. Ann Intern Med 135(3): 209-16. | ||
| In article | View Article PubMed | ||
| [31] | Callahan D. Self-extinction: the morality of the helping hand, in Weir RF eds Physician Assisted Suicide. Bloomington IN: Univ Indiana 1997. | ||
| In article | |||
| [32] | Snyder L, Sulmasy DP (2017). Ethics and the legalization of Physician-Assisted Suicide: An American College of Physicians Position Paper. Ann Intern Med 167(8):576-578. | ||
| In article | View Article PubMed | ||





{kind=link}