Background: Ministry of Health in Kenya National STEPS survey observed, 56% of Kenyans had never been checked for blood pressure, 90% of those on treatment still had their blood pressure uncontrolled and of major concern is complications of hypertension account for over 50% hospitalization and 40% of hospital mortalities [1]. Objective: This study determines Medication adherence health information needs among patients on hypertensive management at Kenyatta National Hospital; Nairobi County, Kenya. Methods: Random sampling was used to select 259 study participants. Systematic sampling was used so that every 2nd patient from the sampling frame was interviewed, the Morisky Medication adherence scale - 8 scale was used. A descriptive cross-sectional design was used and chi-square test and logistic regression were used to analyze the data. Results: Most patients with difficulty in adhering to medication plan had raised blood pressure on clinic day. 88.7% forgot taking medicine the previous day, 71.9% stopped or changed medication dosage without consulting the doctors, 66.7% stopped or skipped using medicine whenever blood pressure was well or controlled, 57.6% feel harassed adhering to treatment plan, and 55.9% forget taking medication when travelling. Conclusion: Health Information on adherence to medication plan was found to be inadequate. Patient factors affect adherence to medication plan, patients with adherence challenges had their blood pressure outside normal ranges on the clinic day. It is recommended that the Kenya Ministry of Health and Kenyatta National hospital improve medication adherence through provision of health information on medication adherence.
Hypertension, is a global public health problem. It contributes to the problem of heart disorders, stroke and renal failure and early mortality and disability. It disproportionately affects populations in low- and middle-income countries where health systems are weak. Globally, according to WHO - World Hypertension Day (2019), hypertension is a grave medical disorder that continues to significantly increase heart ailment, cardiovascular accidents, renal complications, and blindness, and it is projected that 1.13 billion people are living with hypertension, about 1 in 5 have the condition under control. It was observed that the main modifiable contributors to the increase in High blood pressure are unhealthy diets, physical sedentariness and the taking of alcohol and tobacco, and being overweight or obese. In 2016, the WHO and the Centers for Disease Control and Prevention setup a global undertaking to support governments to advance in the prevention and management of cardiac diseases, including hypertension detection and management. According to World Health Organization (WHO), 120/80 mmHg is considered normal blood pressure, and one is contemplated hypertensive when it gets to 140/90 mm Hg. In Sub Saharan Africa, one of the most prevalent non-Communicable diseases that is complex and chronic is Hypertension. It is commonly known as “silent killer” and is a key contributor to cardiac and cerebrovascular disorders 2. The number of people with raised blood pressure in Sub Saharan region is projected to rise from 74.7 million to 125.5 million by 2025, a 68% rise. Lack of adherence to treatment and follow-up for hypertension management is a common occurrence in many resource-limited settings.
Hypertension is the most common cardiac disease, is rapidly becoming Kenya’s prime public health worry, accounting for over 50 per cent of the hospital’s admissions and 40 per cent of hospital mortalities. Latest data from the Ministry of Health in Kenya National STEPS survey for Non-Communicable Disorders Risk Factors, indicate that 56 per cent of Kenyans have never been checked for raised blood pressure 1. The survey disturbingly observed that over 90% of those on treatment for hypertension, had not achieved control of the disease and recommended the establishment of wellness clinics in public hospitals to encourage early recognition and screening of hypertension, and to serve as sources of information for prevention and health promotion. The Council of Governors Health Committee (Kenya) noted that, “The impact of non-communicable disorders (NCDs) on the Kenyan economy could be devastating and pose a serious setback to the attainment of the Government’s Big 4 Agenda and the vision 2030 if no serious interventions are implemented” 3. The Kenyatta National Hospital had four thousand (4000) admissions due to hypertension between 2016 to February 2019. In 2018, the incidences of hypertension in KNH according to hospital health information statistics office were 4000, out of which 15% were attended to in General Medical outpatient clinic. World over, several health guidelines recognize the need to grow patient-centered and patient -directed services that positions the patient central in-service planning and delivery, a tactic encouraged by World Health Organization. It is therefore important to determine the influence of health information needs of patients on hypertension management that could have effect on their care with an objective of improving quality of service delivery for better health outcomes.
A cross-sectional descriptive study was conducted at the medical outpatient clinic at Kenyatta National Hospital in order to examine the relationship between patients’ adherence health Information, and hypertension management at that point in time. Kenyatta National Hospital (KNH) is located along hospital road, off Ngong road, Nairobi, Kenya. KNH is a national teaching and referral hospital serving patients from East and Central Africa, and has a bed capacity of 1800 inpatients. The hospital’s legal mandate includes; Provision of Specialized Quality healthcare, Teaching, Research, and Participation in National policy formulation. It is the apex referral health facility in Kenya which attends to approximately 1850 outpatients each day. The Hospital is a teaching hospital of the College of Health Sciences, University of Nairobi and works in collaborations with other institutions in the provision of clinical services. This design was considered for its appropriateness of assessing the prevalence of health information needs among the patients on hypertensive management and knowledge among the patients and healthcare providers. The target population was hypertensive patients without any co-morbidities, aged 18 years and above and must have been attending the clinic for at least six months. The cross-sectional data collected was used for analytical purposes to determine relationship between the exposure (Information gap) and the outcome (High blood pressure). The use of random sampling in this study provides a valid snapshot of the characteristics among this group of hypertensive patients.
2.2. VariablesThe dependent variable was Health Information need and was categorized as present and absent. The Medication adherence Health information need was present if the hypertensive patient lacked information on the aspects of medication taking behaviour outlined in the Morisky Medication Adherence scale (MMAS-8) and other information they considered important in enabling them manage their condition better. The Pearson chi-square and Fisher's Exact tests were used to measure the dependent variable, where a p-value equal or less than 0.05 was used to determine if the health information needs predict the blood pressure levels among patients on hypertensive managements.
The independent variables were:
Age, Gender, Level of education, missed medication, stopped taking medication, Affordability of treatment prescribed, Information on risks of non-adherence, Information of side-effects of medication
2.3. Sampling, Data Collection and Data AnalysisSystematic random sampling was used for this study. The patients who met the inclusion criteria during the desk review of the medical records were included in the population frame (600). The sampling frame was not arranged in any order and all the members in the sampling frame were randomized in order to obtain a truly representative sample. Systematic Random sampling was continuously used to pick every 2nd patient from the list for inclusion in the study until the required sample size of 259 was attained. Where the kth patient was not available, the subsequent available was picked for inclusion in the study. All patients who consented to participate were included in the study. The patients were recruited on the clinic days and after obtaining consent, the questionnaires were administered to them. Because the population was below 10,000, a sample of 235 was determined using Fisher’s et al., (1998) for population below 10,000. Where; nf = The anticipated final sample size (If the target population is below 10,000), n = The desired sample size (when the target population is greater than 10,000, where confidence interval = 1.96), and N is the target population (600). After adjusting for the declines by 10% the final sample size be 259. The researcher employed data collection tools that had both structured and semi-structured questions. Contingency questions were used so that incase certain questions were not applicable to some respondents, there were follow-up questions to probe the respondents further for more information. The Likert scale was used in the questionnaires to measure adherence to hypertensive medication, Morisky medication adherence scale-8 (MMAS-8) was used in the questionnaire. The arrangement of the items in the data collection tool was done in a logical manner so the respondents were able find their way around the tool without difficulty. The brief and clear instructions were included in the questionnaire to enable the respondent to follow and the pages in the questionnaire were numbered. Data was checked, verified, and corrected for missing data, logical errors, and legibility problems before data entry and analysis was done.
A predesigned data entry format was made for data entry using SPSS for data entry and Version 21 for analysis. The template had inbuilt range checks, skip rules and flag/halt on error during data entry. The double data entry format was employed for data verification to eliminate data entry errors. Open-ended data was assigned codes. Data analysis was done in two steps: Univariate statistics was used to quantitatively describe and summarize all the data collected and the summaries are presented in form of tables and figures. Pearson, and fisher’s exact chi-square tests were performed to test for associations between dependent and independent variables. The variables with a statistically significant association were subjected to logistic regression to generate odds ratio. A p-value equal to 0.05 or less was considered as a significant statistical association.
2.3. Ethical ConsiderationsEthical approval was sought from The Board of Postgraduate studies of Kenyatta University, Ethical clearance from KNH-University of Nairobi ethical review committee, permit for data collection from National Commission for science, Technology, and Innovation (NACOSTI), approval letter from the Head of Medicine Departments (KNH) and a study certificate from KNH Research and Programs. A written informed consent was obtained from the participant after information on purpose and process of data collection of the study was given. Participants were also made aware of their involvement being voluntary and could decline participation at any stage of the interview. The privileges and well-being of the participants was ensured by underscoring to them that their medical care was not going to be affected in any way should they decline to participate in the study. The participants were issued with a duplicate informed consent for their records.
A total of 259 participants were recruited into the study. Their social demographic characteristics evaluated in this study included the respondents’ gender, age, level of education, marital status, employment status and medical insurance cover. Majority 193 (74.5%) of the participants were female, the most common age group was 41 to 50 years old accounting for 32.4%. Most participants 204 (78.8%) were married. A significant number of participants 128 (49.4%) had attained secondary level of education. More than half of the study population was employed, 148 (57.1%), 44 (17.0%) being in formal employment and 104 (40.2%) being self-employed. Many study participants 137 (52.9%) did not have a health insurance cover.
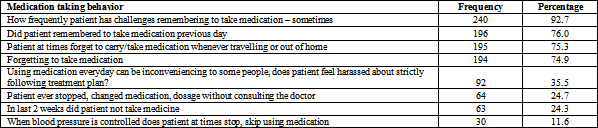
3.2. Medication Adherence Health InformationThe study sought to establish the existence of medication adherence information needs among the hypertensive patients enrolled in the study and how the presence or absence of the same is associated with their blood pressure levels at the time of recruitment in to the study. A total of 259 study participants were evaluated using the Morisky Medication adherence scale - 8 scale (MMAS-8) on the various aspects of medication taking behaviors. A significant number of study participants 240 (92.7%) (Table 1) admitted that they had challenges remembering to take medication sometimes.
The biggest challenge to sticking to medication plan as indicated by the study participants was forgetting to take the medication as indicted by 197 (77.0%), (Table 2).
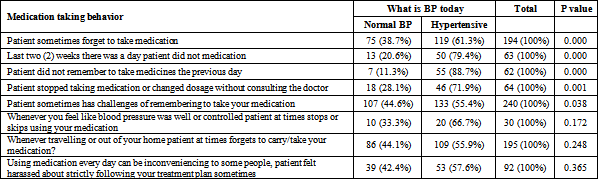
A higher proportion of patients who had a challenge sticking to their medication plan were found to be hypertensive on the day of recruitment, and there was a statistically significant association between their medication taking behaviour and their blood pressure levels with p-values of less than 0.05 (Table 3).
Doctor: “Some patients stop medication once their blood pressure is controlled since they assume they are healed and it is important for them to know the importance of taking medications even when their blood pressure is normal. When you interrogate some, they are not aware of basic things like what drugs they are taking, and even the importance of adherence and the complications of non-adherence”
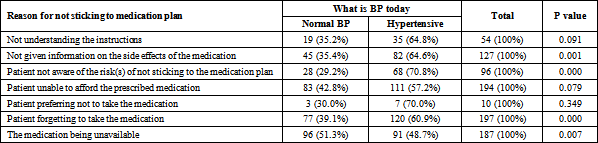
A very significant number 70.8% of patients who indicated not being aware of the risks of not sticking to the medication plan as a cause of non-adherence were outside normal blood pressure ranges. Not remembering to take medication and not getting information on the medication side effects were indicated by 60.9% and 64.6% (Table 4) of the study participants respectively.
Pharmacist: “There should be no break during the treatment even if the drug is not available in KNH pharmacy”. There is need “to avail the drugs all the time and prescribers should adhere to the KNH formulary. Most of the patients do not understand the instructions of taking medicines correctly, some do not know their medicines.” Nutritionist: “The importance or consequence of adherence or non-adherence to medication”
Pharmacy technologist: “Most medications are taken at different times of the day and it’s a challenge since most patients tend to forget and the consistency of taking medication is also a challenge.” “Other information I consider important for a hypertensive patient include; Patient to keep to appointments, Causes of Blood pressure should be explained to the client, information on how to relapse in blood pressure, the doctor should emphasis on medication adherence and advise of physical exercise and change in lifestyle, education on the mode of action of the drug, the time specified to be used (morning or evening), there should be Medication Therapy Management (MTM) services for the patients.”
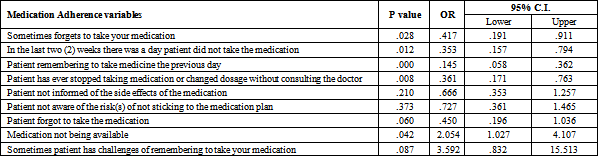
3.4. Logistic RegressionThe study found out that there was a strong statistically significant association between high blood pressure levels and unavailability of medication and patients having challenges remembering to take your medication. Unavailability of medication and patients having challenges remembering to take your medication increased the likelihood of uncontrolled blood pressure by 2.05 and 3.59 times respectively (Table 5).
Medication adherence health information need in this study was found to be present. This may be attributed to heavy workload and limited time with the patient or even patient missing of appointment and thus loss of continuity in management. In this study 92.7% of the study participants had challenges remembering to take their medication. Top amongst the challenges in medication taking plan was forgetting to take the medication, followed by affordability of the prescription. This compares to a study conducted among 7,498 adult patients in United States that concluded that; only those patients without cost-related medication issues were likely to adhere to antihypertensive treatment prescribed and have a normal blood pressure than those with cost-related medication challenges 4.
Patient factors were seen to have a big influence on adherence to medication plan in this study. Most patients with adherence challenges being outside normal blood pressure ranges on the day of clinic. A higher percentage (88.7%) of patients did not remember to take medicine the day prior to their recruitment in the study, while 71.9% of patients reported to have stopped or changed medication dosage without consulting the doctors. Consequently, a significant number of patients admitted not having taken their medicine in the last 2 weeks prior to clinic day and this was significantly associated with uncontrolled blood pressure among such patients where p=0.000. The findings of the study indicate that there was a strong association (p=0.000) between abnormal blood pressure levels in patients who reported skipping or stopping medication taking whenever their blood pressure levels were normal or controlled or forgot to take their medication. More than half of the patients who reported that they felt harassed about strictly following treatment plan, forgot to carry/take their medication whenever they were away from home or sometimes had challenges of remembering to take their medication resulting to poor medication adherence had their blood pressure levels outside normal blood pressure ranges on the day of clinic. These findings indicate that it is important that hypertensive patients are provided with information on medication instruction, including side effects and the consequences of not adhering to the treatment plan, the consequences of dosage changes without consulting the doctor, and stopping medication when they deemed the blood pressure was well or controlled without doctor’s advice. This finding concurs to a great extend with the findings in a systematic review of Randomized Controlled Trials, to ascertain pharmacist involvements in improving hypertension control and adherence among people with raised blood pressure which concluded that; pharmacist interventions through education, counselling or both had an impact on the blood pressure control and medication adherence 5. Therefore, the presence of this informational gap is likely to have a negative effect of the patients’ blood pressure levels due to poor adherence to medication.
When asked whether they thought patients seeking medical attention for high blood pressure at KNH were well informed of their condition, majority of the health workers, that is; doctors, nurses and laboratory technologists indicated that the patients were not well informed. The health care workers sited that most patients were unaware of their drugs and lacked information on adherence to treatment. They observed that the health workers lack time to give adequate treatment information due to heavy workload and patient literacy levels, and this tends to deny the patients’ time and opportunity to ask questions or express any concerns regarding their medication or treatment of the condition.
This study found presence of medication adherence health information need among patients on hypertensive management and this was associated with uncontrolled blood pressure levels. It is therefore recommended that the Kenyan Ministry of Health increases awareness of medication adherence health information through enhanced health education programmes.
The findings of this study indicate that Unavailability of medicines was strongly associated with uncontrolled blood pressure. It therefore recommends that the Ministry of Health, healthcare facilities, ministry departments and all the stakeholders develop strategies to enhance availability of hypertensive medicines.
Further research should be done on information needs for other conditions complicated by high blood pressure
The study found out that there was a strong statistically significant association between high blood pressure levels and unavailability of medication and patients having challenges remembering to take your medication. Unavailability of medication and patients having challenges remembering to take your medication increased the likelihood of uncontrolled blood pressure by 2.05 and 3.59 times respectively. These factors were seen to have a strong influence on adherence to medication plan in this study with most of the patients with adherence challenges being outside normal blood pressure ranges on the day of clinic.
I give all the glory to God Almighty for this achievement. The development of this thesis incorporated an intellectual journey that would not have been successful without the guidance, training, mentorship, and the support of my supervisors; Dr. Joyce C. Kirui and Dr. Eliphas Gitonga for whom I sincerely thank for their invaluable contribution to this work. I am forever grateful to Kenyatta National Hospital Board of Management and The Chief Executive Officer (KNH) for the release for training and sponsorship, The Director Diagnostics and Health Information, The HOD Health Information Department, The HOD Medicine Department (KNH) and all healthcare staff for their support during data collection, to Janet Musia (University of Nairobi, Paediatrics Department) for the data management, my wife Lilian and family and Cynthia Cherono Ruto for their immense support and encouragement. I am grateful to Kenyatta University Graduate School, The Chairperson, Department of Health Management and Informatics, Kenyatta National Hospital/University of Nairobi Ethics and Research Committee (KNH/UoN-ERC), National Council for Science, Technology, and Innovation for granting the necessary clearance for the study.
BMI: Body mass index
BP: Blood Pressure
CKD: Chronic kidney disease
CVA: Cardiovascular Accident
ECG: Echocardiogram
EHR: Electronic Health Records
ESH: European Society of Hypertension
HTN: Hypertension
ISH: International Society of Hypertension
KNH: Kenyatta national Hospital
MMAS-8: Morisky Medication Adherence Scale-8
MOH: Ministry of Health
MTM: Medication Therapy management
NACOSTI: National Science Technology and Innovation review committee
NCD: Non-communicable diseases
WHO: World Health Organization
| [1] | STEPS. The STEPS survey report, Kenya, 2015. Available at http://aphrcorg/wp-content/uploads/2016/04/Steps-Report-NCD-2015pdf.Accessed on 30th July 2019. | ||
| In article | |||
| [2] | Helena L, Aliya N, Asita de Silva H, Imtiaz J, Victoria H, Benjamin C, Saeideh T, Nantu C, et al. Patients’ experience on accessing health care services for management of hypertension in rural Bangladesh, Pakistan and Sri Lanka: A qualitative study. PLOS one.2019; 14(1): e0211100. | ||
| In article | View Article PubMed | ||
| [3] | Muthoni, W. (2018, November). Hypertension fast becoming Kenya’s biggest public health concern. Capital News. | ||
| In article | |||
| [4] | Fang J, Chang T, Wang G, Loustalot F. (2020). Association between cost-related medication nonadherence and hypertension management among US adults. Am J Hypertens. 2020 May 5: hpaa072. | ||
| In article | |||
| [5] | Reeves L, Robinson K, McClelland T, Adedoyin CA, Broeseker A, AdunlinG.Pharmacist Interventions in the Management of Blood Pressure Control and Adherence to Antihypertensive Medications: A Systematic Review of Randomized Controlled Trials. J Pharm Pract. 2020 Feb 18: 897190020903573. | ||
| In article | View Article PubMed | ||
| [6] | Abbas H, Kurdi M, de Vries F, van Onzenoort HAW, Driessen JHM, Watfa M, Karam R. Factors Associated with Antihypertensive Medication Non-Adherence: A Cross- Sectional Study Among Lebanese Hypertensive Adults. Patient Prefer Adherence. 2020. Apr 1; 14: 663-673. | ||
| In article | View Article PubMed | ||
| [7] | Aboyan, I., Grachev, S., Pakus, S., Pakus, D., &Shiranov, K. (2016). Mini-percutaneous nephrolithotomy. Specificities of surgical technique. Urology And Andrology, 4(3), 41-44. | ||
| In article | View Article | ||
| [8] | Allen B, Thorwarth WT. (2014). Comments from the American College of Radiology. Washington, DC: 2014. (Input submitted to the Committee on Diagnostic Error in Health Care, November 5 and December 29, 2014). | ||
| In article | |||
| [9] | AMA (American Medical Assocation) (2014). Improving care: Priorities to improve electronic health record usability. 2014. [February 9, 2015]. www.ama-assn.org/ama/pub/about-ama/strategic-focus/enhancing-professional-satisfaction-and-practice-sustainability.page. | ||
| In article | |||
| [10] | Briganti EM, Shaw JE, Chadban SJ, Zimmet PZ, Welborn TA, McNeil JJ, Atkins RC. Untreated hypertension among Australian adults: The 1999-2000 Australian diabetes, obesity and lifestyle study (AusDiab). MJA 2003; 179: 135-139. | ||
| In article | View Article PubMed | ||
| [11] | Carayon P, Faye H, Hundt AS, Karsh BT, T. Wetterneck T. Handbook of Healthcare Delivery Systems. Yuehwern Y, editor. Boca Raton, FL: Taylor & Francis; 2011. pp. 12-1–12-15. (Patient safety and proactive risk assessment). | ||
| In article | |||
| [12] | Chappell, F. (2015). Medication adherence in children remains a challenge. Prescriber, 26(12), 31-34. | ||
| In article | View Article | ||
| [13] | Espeche W, Salazar MR, Sabio R, Diaz A, LeivaSisnieguez C, Olano D, Balbin E, Renna N, Grosse P, Flores RA, Lagos AC, Ferrer P, Poppe S, Risso Patron F, SotnieczukStasiuk VD, Valentini E, Cardozo JR, Romano JR, Parodi R, Carbajal H. Adherence to antihypertensive drug treatment in Argentina: A multicenter study. J ClinHypertens (Greenwich). 2020 Apr; 22(4): 656-662. | ||
| In article | View Article PubMed | ||
| [14] | Frantz, R. (2018). Treatment Considerations for Pulmonary Arterial Hypertension and Assessment of Treatment Response. Advances In Pulmonary Hypertension, 16(3), 120-124. | ||
| In article | View Article | ||
| [15] | Gabb GM, Mangoni A, Anderson CS, Cowley D, Dowden JS, Golledge J, et al. (2017). Guideline Hamrahian SM. Management of Hypertension in Patients with Chronic Renal Disease. Curr Hypertens Rep. 2017 May; 19(5): 43. | ||
| In article | View Article PubMed | ||
| [16] | Garrison L, Mestre-Ferrandiz J, Zamora B. The Value of Knowing and Knowing the Value: Improving the Health Technology Assessment of Complementary Diagnostics. London, UK: Office of Health Economics; 2016 | ||
| In article | View Article | ||
| [17] | Huffman MD and Lloyd-Jones DM. Global burden of raised blood pressure: Coming into focus. JAMA 2017 Jan 10; 317: 142. | ||
| In article | View Article PubMed | ||
| [18] | Hussein A, Awad MS, Mahmoud HEM. Patient adherence to antihypertensive medications in upper Egypt: a cross-sectional study. Egypt Heart J. 2020 May 25; 72(1): 29. | ||
| In article | View Article PubMed | ||
| [19] | Institute for Health Metrics and Evaluation and the International Centre for Humanitarian Affairs. The Global Burden of Disease: Generating Evidence, Guiding Policy in Kenya. Nairobi, Kenya; 2016. | ||
| In article | |||
| [20] | Jankowska-Polańska B, Uchmanowicz I, Dudek K, Mazur G. Relationship between patients & rsquo; knowledge and medication adherence among patients with hypertension [Internet]. Patient Preference and Adherence. 2016 [cited 2018 Dec 10]. Available from: https://www.dovepress.com/relationship-between-patientsrsquo-knowledge-andmedication-adherence--peer-reviewed-fulltext-article-PPA. | ||
| In article | View Article PubMed | ||
| [21] | Macquart de Terline D, Kramoh KE, Bara Diop I, Nhavoto C, Balde DM, Ferreira B, Houenassi MD, Hounsou D, Ikama MS, Kane A, Kimbally-Kaki SG, Kingue S, Koffi F, Kouam Kouam C, Limbole E, Mfeukeu Kuate L, Mipinda JB, N'goran Y, Sesso Z, SidiAly A, Toure IA, Plouin PF, Azizi M, Perier MC, Narayanan K, Empana JP, Jouven X, Antignac M (2020). Poor adherence to medication and salt restriction as a barrier to reaching blood pressure control in patients with hypertension: Cross- sectional study from 12 sub- Saharan countries. Arch Cardiovasc Dis. 2020 May 17: S1875-2136(20)30101-7. | ||
| In article | |||
| [22] | MOH. Kenya National Guidelines for Cardiovascular Diseases management; Division of Non-Communicable Diseases, Nairobi-Kenya (2018). | ||
| In article | |||
| [23] | Nishigaki N, Shimasaki Y, Yoshida T, Hasebe N. Physician and patient perspectives on hypertension management and factors associated with lifestyle modifications in Japan: results from an online survey. Hypertens Res. 2020 May; 43(5): 450-462. | ||
| In article | View Article PubMed | ||
| [24] | Nishimura S, Kumamaru H, Shoji S, Sawano M, Kohsaka S, Miyata H. Adherence to antihypertensive medication and its predictors among non-elderly adults in Japan. Hypertens Res. 2020 Jul; 43(7): 705-714. | ||
| In article | View Article PubMed | ||
| [25] | Odedosu T, Schoenthaler A, Vieira DL, Agyemang C, Ogedegbe G. Overcoming barriers to hypertension control in African Americans. Cleve Clin J Med 2012; 79:46-56. | ||
| In article | View Article PubMed | ||
| [26] | Rasmussen JN, Chong A & Alter DA (2017). Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA. 2007; 297: 177-186. | ||
| In article | View Article PubMed | ||
| [27] | Sanii Y, Torkamandi H, Gholani K, Hadavand N, Javadi M. Role of pharmacist counseling in pharmacotherapy quality improvement. J Res Pharm Pract. 2016; 5(2): 132-7. | ||
| In article | View Article PubMed | ||
| [28] | Schmieder RE. Goebel M. Bramlage P. Barriers to cardiovascular risk prevention and management in Germany—an analysis of the EURIKA study. Vasc Health Risk Manag 2012; 8: 177-186. | ||
| In article | View Article PubMed | ||
| [29] | Shukri, F.M., Martin, K.M, Richard, W., Fredrick, W., Tilahun, H., Pamela, J., Loise, N., Catherine, K., & Elijah, O. (2018). Prevalence, awareness, treatment and control of hypertension and their determinants.BMC Public Health, 18 (Suppl 3). | ||
| In article | View Article PubMed | ||
| [30] | Sokol MC, McGuigan KA, Verbrugge RR & Epstein RS (2015). Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005; 43: 521-530. | ||
| In article | View Article PubMed | ||
| [31] | Tadesse M A, Shehab A, Eyob A G, Akshaya S. B, Ahmed A. E. Nonadherence to antihypertensive drugs; A systematic review and meta-analysis, Medicine (Baltimore). 2017 Jan: 96(4): e5641. | ||
| In article | View Article PubMed | ||
| [32] | Wang K, Li Y, Liu G, Rimm E, Chan AT, Giovannucci EL, Song M. Healthy Lifestyle for Prevention of Premature Death Among Users and Nonusers of Common Preventive Medications: A Prospective Study in 2 US Cohorts. J Am Heart Assoc. 2020 Jul 7; 9(13): e016692. | ||
| In article | View Article PubMed | ||
| [33] | White F, Wang L, Jelinek H. Awareness, and pharmacotherapy of hypertension in a rural community. Med Princ Pract 2009; 18: 261-265. | ||
| In article | View Article PubMed | ||
| [34] | WHO. Raised blood pressure. Situation and trends. Available at http://www.who.int/gho/ncd/risk_factors/blood_pressure_prevalence_text/en/. Last acc. | ||
| In article | |||
Published with license by Science and Education Publishing, Copyright © 2023 Alembi Osanya Ayub, Dr Joyce C. Kirui and Dr. Eliphas Gitonga
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | STEPS. The STEPS survey report, Kenya, 2015. Available at http://aphrcorg/wp-content/uploads/2016/04/Steps-Report-NCD-2015pdf.Accessed on 30th July 2019. | ||
| In article | |||
| [2] | Helena L, Aliya N, Asita de Silva H, Imtiaz J, Victoria H, Benjamin C, Saeideh T, Nantu C, et al. Patients’ experience on accessing health care services for management of hypertension in rural Bangladesh, Pakistan and Sri Lanka: A qualitative study. PLOS one.2019; 14(1): e0211100. | ||
| In article | View Article PubMed | ||
| [3] | Muthoni, W. (2018, November). Hypertension fast becoming Kenya’s biggest public health concern. Capital News. | ||
| In article | |||
| [4] | Fang J, Chang T, Wang G, Loustalot F. (2020). Association between cost-related medication nonadherence and hypertension management among US adults. Am J Hypertens. 2020 May 5: hpaa072. | ||
| In article | |||
| [5] | Reeves L, Robinson K, McClelland T, Adedoyin CA, Broeseker A, AdunlinG.Pharmacist Interventions in the Management of Blood Pressure Control and Adherence to Antihypertensive Medications: A Systematic Review of Randomized Controlled Trials. J Pharm Pract. 2020 Feb 18: 897190020903573. | ||
| In article | View Article PubMed | ||
| [6] | Abbas H, Kurdi M, de Vries F, van Onzenoort HAW, Driessen JHM, Watfa M, Karam R. Factors Associated with Antihypertensive Medication Non-Adherence: A Cross- Sectional Study Among Lebanese Hypertensive Adults. Patient Prefer Adherence. 2020. Apr 1; 14: 663-673. | ||
| In article | View Article PubMed | ||
| [7] | Aboyan, I., Grachev, S., Pakus, S., Pakus, D., &Shiranov, K. (2016). Mini-percutaneous nephrolithotomy. Specificities of surgical technique. Urology And Andrology, 4(3), 41-44. | ||
| In article | View Article | ||
| [8] | Allen B, Thorwarth WT. (2014). Comments from the American College of Radiology. Washington, DC: 2014. (Input submitted to the Committee on Diagnostic Error in Health Care, November 5 and December 29, 2014). | ||
| In article | |||
| [9] | AMA (American Medical Assocation) (2014). Improving care: Priorities to improve electronic health record usability. 2014. [February 9, 2015]. www.ama-assn.org/ama/pub/about-ama/strategic-focus/enhancing-professional-satisfaction-and-practice-sustainability.page. | ||
| In article | |||
| [10] | Briganti EM, Shaw JE, Chadban SJ, Zimmet PZ, Welborn TA, McNeil JJ, Atkins RC. Untreated hypertension among Australian adults: The 1999-2000 Australian diabetes, obesity and lifestyle study (AusDiab). MJA 2003; 179: 135-139. | ||
| In article | View Article PubMed | ||
| [11] | Carayon P, Faye H, Hundt AS, Karsh BT, T. Wetterneck T. Handbook of Healthcare Delivery Systems. Yuehwern Y, editor. Boca Raton, FL: Taylor & Francis; 2011. pp. 12-1–12-15. (Patient safety and proactive risk assessment). | ||
| In article | |||
| [12] | Chappell, F. (2015). Medication adherence in children remains a challenge. Prescriber, 26(12), 31-34. | ||
| In article | View Article | ||
| [13] | Espeche W, Salazar MR, Sabio R, Diaz A, LeivaSisnieguez C, Olano D, Balbin E, Renna N, Grosse P, Flores RA, Lagos AC, Ferrer P, Poppe S, Risso Patron F, SotnieczukStasiuk VD, Valentini E, Cardozo JR, Romano JR, Parodi R, Carbajal H. Adherence to antihypertensive drug treatment in Argentina: A multicenter study. J ClinHypertens (Greenwich). 2020 Apr; 22(4): 656-662. | ||
| In article | View Article PubMed | ||
| [14] | Frantz, R. (2018). Treatment Considerations for Pulmonary Arterial Hypertension and Assessment of Treatment Response. Advances In Pulmonary Hypertension, 16(3), 120-124. | ||
| In article | View Article | ||
| [15] | Gabb GM, Mangoni A, Anderson CS, Cowley D, Dowden JS, Golledge J, et al. (2017). Guideline Hamrahian SM. Management of Hypertension in Patients with Chronic Renal Disease. Curr Hypertens Rep. 2017 May; 19(5): 43. | ||
| In article | View Article PubMed | ||
| [16] | Garrison L, Mestre-Ferrandiz J, Zamora B. The Value of Knowing and Knowing the Value: Improving the Health Technology Assessment of Complementary Diagnostics. London, UK: Office of Health Economics; 2016 | ||
| In article | View Article | ||
| [17] | Huffman MD and Lloyd-Jones DM. Global burden of raised blood pressure: Coming into focus. JAMA 2017 Jan 10; 317: 142. | ||
| In article | View Article PubMed | ||
| [18] | Hussein A, Awad MS, Mahmoud HEM. Patient adherence to antihypertensive medications in upper Egypt: a cross-sectional study. Egypt Heart J. 2020 May 25; 72(1): 29. | ||
| In article | View Article PubMed | ||
| [19] | Institute for Health Metrics and Evaluation and the International Centre for Humanitarian Affairs. The Global Burden of Disease: Generating Evidence, Guiding Policy in Kenya. Nairobi, Kenya; 2016. | ||
| In article | |||
| [20] | Jankowska-Polańska B, Uchmanowicz I, Dudek K, Mazur G. Relationship between patients & rsquo; knowledge and medication adherence among patients with hypertension [Internet]. Patient Preference and Adherence. 2016 [cited 2018 Dec 10]. Available from: https://www.dovepress.com/relationship-between-patientsrsquo-knowledge-andmedication-adherence--peer-reviewed-fulltext-article-PPA. | ||
| In article | View Article PubMed | ||
| [21] | Macquart de Terline D, Kramoh KE, Bara Diop I, Nhavoto C, Balde DM, Ferreira B, Houenassi MD, Hounsou D, Ikama MS, Kane A, Kimbally-Kaki SG, Kingue S, Koffi F, Kouam Kouam C, Limbole E, Mfeukeu Kuate L, Mipinda JB, N'goran Y, Sesso Z, SidiAly A, Toure IA, Plouin PF, Azizi M, Perier MC, Narayanan K, Empana JP, Jouven X, Antignac M (2020). Poor adherence to medication and salt restriction as a barrier to reaching blood pressure control in patients with hypertension: Cross- sectional study from 12 sub- Saharan countries. Arch Cardiovasc Dis. 2020 May 17: S1875-2136(20)30101-7. | ||
| In article | |||
| [22] | MOH. Kenya National Guidelines for Cardiovascular Diseases management; Division of Non-Communicable Diseases, Nairobi-Kenya (2018). | ||
| In article | |||
| [23] | Nishigaki N, Shimasaki Y, Yoshida T, Hasebe N. Physician and patient perspectives on hypertension management and factors associated with lifestyle modifications in Japan: results from an online survey. Hypertens Res. 2020 May; 43(5): 450-462. | ||
| In article | View Article PubMed | ||
| [24] | Nishimura S, Kumamaru H, Shoji S, Sawano M, Kohsaka S, Miyata H. Adherence to antihypertensive medication and its predictors among non-elderly adults in Japan. Hypertens Res. 2020 Jul; 43(7): 705-714. | ||
| In article | View Article PubMed | ||
| [25] | Odedosu T, Schoenthaler A, Vieira DL, Agyemang C, Ogedegbe G. Overcoming barriers to hypertension control in African Americans. Cleve Clin J Med 2012; 79:46-56. | ||
| In article | View Article PubMed | ||
| [26] | Rasmussen JN, Chong A & Alter DA (2017). Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA. 2007; 297: 177-186. | ||
| In article | View Article PubMed | ||
| [27] | Sanii Y, Torkamandi H, Gholani K, Hadavand N, Javadi M. Role of pharmacist counseling in pharmacotherapy quality improvement. J Res Pharm Pract. 2016; 5(2): 132-7. | ||
| In article | View Article PubMed | ||
| [28] | Schmieder RE. Goebel M. Bramlage P. Barriers to cardiovascular risk prevention and management in Germany—an analysis of the EURIKA study. Vasc Health Risk Manag 2012; 8: 177-186. | ||
| In article | View Article PubMed | ||
| [29] | Shukri, F.M., Martin, K.M, Richard, W., Fredrick, W., Tilahun, H., Pamela, J., Loise, N., Catherine, K., & Elijah, O. (2018). Prevalence, awareness, treatment and control of hypertension and their determinants.BMC Public Health, 18 (Suppl 3). | ||
| In article | View Article PubMed | ||
| [30] | Sokol MC, McGuigan KA, Verbrugge RR & Epstein RS (2015). Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005; 43: 521-530. | ||
| In article | View Article PubMed | ||
| [31] | Tadesse M A, Shehab A, Eyob A G, Akshaya S. B, Ahmed A. E. Nonadherence to antihypertensive drugs; A systematic review and meta-analysis, Medicine (Baltimore). 2017 Jan: 96(4): e5641. | ||
| In article | View Article PubMed | ||
| [32] | Wang K, Li Y, Liu G, Rimm E, Chan AT, Giovannucci EL, Song M. Healthy Lifestyle for Prevention of Premature Death Among Users and Nonusers of Common Preventive Medications: A Prospective Study in 2 US Cohorts. J Am Heart Assoc. 2020 Jul 7; 9(13): e016692. | ||
| In article | View Article PubMed | ||
| [33] | White F, Wang L, Jelinek H. Awareness, and pharmacotherapy of hypertension in a rural community. Med Princ Pract 2009; 18: 261-265. | ||
| In article | View Article PubMed | ||
| [34] | WHO. Raised blood pressure. Situation and trends. Available at http://www.who.int/gho/ncd/risk_factors/blood_pressure_prevalence_text/en/. Last acc. | ||
| In article | |||