 OPEN ACCESS
OPEN ACCESS PEER-REVIEWED
PEER-REVIEWEDA Comparison of Three Age-based Formulae of Estimating Weight in Nigerian Children
Ilori Iniabasi Udoh1, , Ikobah Joanah Moses2
, Ikobah Joanah Moses2
1Department of Anaesthesiology, University of Calabar / University of Calabar Teaching Hospital, Calabar, Nigeria
2Department of Paediatrics, University of Calabar Teaching Hospital, Calabar, Nigeria
Abstract
In children drug doses, fluid therapy and other treatment modalities are calculated on the basis of weight. In some clinical situations weight measurement becomes impracticable and estimation has to be made. The aim of the study was to compare the accuracy of the Advance Paediatric Life Support(APLS), Luscombe and Argall formulae in estimating the weight of children in developing environment of Southern Nigerian. Children who fulfilled the inclusion criteria in the Children Outpatient Clinic of the University of Calabar Teaching Hospital, Calabar were recruited into the study. The weights of these children were measured using standard procedure. These were then compared with the values obtained by the Advanced Paediatric Life Support, Luscombe and Argall formulae. One hundred and fourteen (114) children (63 males and 51 females) were recruited. There was no significant difference between the sexes in regards to their mean age, measured weight and estimated weights differences. The APLS formula under estimated the weights while Luscombe and Argall formulae overestimated the weights. However the mean percentage difference between the measured weight was least with the Argall formula in children above five years while children one to five years had the least mean percentage weight difference with APLS formula. Conclusion The APLS formula significantly underestimated the weight in children above five years while Luscombe formula significantly overestimated the weights in all age groups. The Argall formula minimally overestimated the weight in all the age groups but had the least mean weight difference in children above five years. In our environment, the APLS formula might be more accurate for weight estimation in children 1-5 years and Argall formula for 6-14 years.
Keywords: age based; weight estimation; developing environment.
Received June 09, 2015; Revised June 29, 2015; Accepted July 03, 2015
Copyright © 2015 Science and Education Publishing. All Rights Reserved.Cite this article:
- Ilori Iniabasi Udoh, Ikobah Joanah Moses. A Comparison of Three Age-based Formulae of Estimating Weight in Nigerian Children. American Journal of Medical Sciences and Medicine. Vol. 3, No. 2, 2015, pp 24-27. http://pubs.sciepub.com/ajmsm/3/2/4
- Udoh, Ilori Iniabasi, and Ikobah Joanah Moses. "A Comparison of Three Age-based Formulae of Estimating Weight in Nigerian Children." American Journal of Medical Sciences and Medicine 3.2 (2015): 24-27.
- Udoh, I. I. , & Moses, I. J. (2015). A Comparison of Three Age-based Formulae of Estimating Weight in Nigerian Children. American Journal of Medical Sciences and Medicine, 3(2), 24-27.
- Udoh, Ilori Iniabasi, and Ikobah Joanah Moses. "A Comparison of Three Age-based Formulae of Estimating Weight in Nigerian Children." American Journal of Medical Sciences and Medicine 3, no. 2 (2015): 24-27.
| Import into BibTeX | Import into EndNote | Import into RefMan | Import into RefWorks |
1. Introduction
In clinical practice drug dosages, fluid therapy, ventilator tidal volumes setting and electric cardiac counter shock are calculated based on a child’s weight [1, 2] Measurement of a child’s weight using a calibrated scale is the gold standard. This is not always possible due to the clinical scenario or urgency of treatment. In developing countries it is sometimes difficult to obtain an accurate weight as many medical clinics lack suitable and accurately calibrated scales. [3, 4] Many formulae have been developed in attempt to accurately estimate a child’s weight using age (Advance Paediatric Life Support, APLS) [5], Luscombe) [6], total body length (Broselow Tape) [7], parental or nurse estimation. [8], some physical features like mid upper arm circumference and humeral length which are added together get the estimated weight (Mercy Method). These measurements which could be cumbersome and time consuming in a sick child, Mercy Tape was developed to ease the process and the estimated weight can be read directly from the tape [4]. The method was reported to accurately estimate the weight of children, however, this device (Mercy Tape) is not easily accessible as it is patented. The age –based formulae which do not cause any discomfort to the critically ill child in that it just involved simple arithmetic calculation. The Advance Paediatric Life Support (APLS) formula, weight = 2(age in years + 4) which is age based was initially advocated for use in children one to ten years. With improvement in economic status, the weights of children in richer countries have been increasing, thus there have been documentation by some authors that the APLS formula underestimates a child’s weight while Luscombe’s formula (weight(kg) = 3(age)+7) was reported to be more accurately in estimating the weight of the child. [1, 2, 6, 10, 11, 12]. The APLS formula underestimates the weight of children in UK by 18.8% [6], New Zealand by 24.7% [2], in Korean children by 11% [11] and in Kenyan children by 5.2%[12]. With this evidence, the Advance Life Support Group (ALSG) advised that health professionals decide locally what method provides the easiest and best method of weight estimation in children for their own use. Furthermore it recommended that the APLS formula should be used to estimate weight in one to five years, while Luscombe [6] formula is used for older children. [5] This recommendation might not be applicable to a developing environment where poor nutritional status is rife. Sebanjo et al [13] in their study of a rural community in Osun state in Nigeria documented a 20.5 % prevalence of malnutrition. In Nigeria, the APLS formula is what is commonly used to estimate weight of children. The Luscombe formula has been widely validated especially in developed countries while Argall formula 3(age +2) was reported by Nguyen et al [14] in Australia to have failed validation by significantly underestimating the weight of their children. On the contrary, they reported that Argall was more accurate in the Asian than the white children The aim of the study is to assess the reliability of the APLS, Luscombe and Argall formulae in estimating weight in Nigerian children
2. Materials and Methods
It was a prospective study. Data was collected from patients aged 1-14 years attending Children Outpatient Clinic(CHOP) at University of Calabar Teaching Hospital in June and July 2014.The parameters collected were the age in years rounded up to the nearest year, sex, weight in kilogram measured on a calibrated scale without shoe and minimal clothing, The estimated weight based on APLS, 2(age in years + 4), Luscombe (3xage in years)+7 and Argall( 3(age in years +2) formulae were calculated for each child and documented. Children with conditions that could affect the weight (amputation, dwarfism, severe joint contractures, or neurologic defects known to affect growth eg,cerebral palsy, oedema); children with any chronic disease, uncooperative children and those whose age could not be accurately determined by their parents or caregiver were excluded. The mean percentage weight difference between the measured weight and the estimated weight was also determined.
Data Analysis: The patients were grouped into three based on their ages for analysis. The groupings were 1(ages 1 -5), 2(ages 6 -10) and 3(ages 11-14). Categorical data are presented as figures, mean with standard deviation. The mean percentage weight difference between the measured weight and the estimated weight was calculated by the formula: [measured weight – estimated weight / measured weight] x 100. Paired t-test was used to determine the statistical significance of any variation between the measured and estimated weights. Data was analyzed using SPSS software version 14
3. Results
Data was collected from one hundred and fourteen (114) children. There were 63 males and 51 females giving a male to female ratio of 1.2:1. Table 1 shows that there was no significant difference between sexes in regard to their mean age, measured weight and estimated weights. The APLS formula under estimated the weights while Luscombe and Argall formulae overestimated the weights.

 Download as
Download as
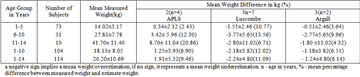
Analysis of the age groups and their measured weights in comparison with the estimated weights formulae is shown in Table 2. The APLS formula underestimated the weight in all the age groups. The least underestimation was 2.43% which was in the age group 1-5yrs and highest in the 11-14 years with the value of 20.86%.. The overall underestimation with APLS formula was 9.46%. Luscombe and Argall formulae overestimated the weights in all the age groups. The formula with the least weight difference among the different age groups was the Argall formula (3n+6). The range was - 0.51kg (3.64%) in group 1 and -2.77(9.96%) in the 6-10years group overestimation. The Luscombe formula significantly overestimated the weight in all the age group.
 Download as
Download as
4. Discussions
The need to know the actual weight of a child during an emergency care cannot be over emphasised as all treatment ranging from drug dosages to equipment size is dependent on the child’s weight. The APLS formula had been the most widely used age based formulae for weight estimation until it was demonstrated by Luscombe to underestimates the weight of children which could result in poor outcome during resuscitation as a result inadequate therapy. [6] The APLS formula has been reported by several authors to underestimate the weight of children. This study has also shown that the APLS formula underestimated the weight in the 1-10years by 6.9%. This is comparable to a number of other reports. A percentage underestimation of 5.6% was found in Kenya [12], 3.3% in Western Cape, South Africa [15], 7.6% in Singapore [16]. In Trinidad, an underestimation of 1.4kg was reported among children 1- 5 years old, though the percentage difference was not reported to make for comparison. These countries with single digit underestimation may be classified as developing countries. The degree of underestimation reported in developed countries has been relatively high. Luscombe [2] reported in UK a 21.9% underestimation in 1-10years, a 24.7% was reported in New Zealand. An 11.5% was reported in Korean children [11]. These documented findings in developed countries of underestimation of weight by APLS formula prompted the Advanced Paediatric Life Support Group to update its recommendation. It suggested that the APLS formula of 2 (age in years+4) should be used for age group 1-5years and Luscombe formula (3 x age in years)+7 for 6-12years. The Luscombe formula has been validated by several authors in developed countries to accurately estimate the weight of children with minimum error from the measured weight. Luscombe et al in Uk reported an over estimation of 2.0% [2]. Kelly et a l[3] in Australia reported a mean weight difference of 0.66kg. Seddon et al [17] in a study of multiethinic population in Europe and Ali [8] in Trinidad concluded that the Luscombe formula provides a better estimation of weight in children they studied. On the contrary, the finding in this study is that the Luscombe formula significantly overestimated the weight in all the age groups. It overestimated the weight in the 1-10yrs by 12.02 %.and in 6-10years by 13.56% This is similar to 12.4% documented by Geduld et al [15] in South Africa. In Singaporean children it overestimated the weight by 7.4%. Therefore Luscombe formula may not be accurate in estimating weight in a developing environment
The formula (age in years +2) x 3, proposed by Argall et al in 2003 [1] has not been widely validated by researchers as Luscombe’s. In this study the Argall formula had the least percentage mean weight differences in all the age groups studied though it was an overestimation. In the 1-10years, it overestimated the weight by 6.51% compared to 12.02% by Luscombe. Seddon et al reported a 6.6% overestimation in 1-5yrs and 3.5% in 6-10years. [17] The reverse was observed in this study with 9.96% in 6-10years and 3.64% in 1-5years. Argall reported a mean bias of -0.52kg as this is not in percentage, comparison could be misleading. Nevertheless, the mean negative bias of 0.52kg indicates minimal deviation from the measured weight. The APLS formula in this study significantly underestimated the weights in 6-10years by 12.30% and 20.86% in 11-14years. Thus APLS formula is inaccurate for weight estimation in Nigerian children above 5years. The Argall formula 3(age in years +2) might be more accurate for weight estimation in Nigerian children 6-14yrs. The APLS formula underestimated the weight in 1-5yrs by 2.43% and Argall formula overestimated by 3.64%. Anderson [18] in his commentary suggested that overestimation is potentially dangerous. He further commented that the current maintenance fluid therapy is based on the supposition that energy expenditure is linked to body weight. Energy expenditure in sick children is at its resting state and is closely linked to lean body mass and blood volume. Therefore using the current Luscombe formula which is reported to be accurate in weight estimation in children in developed countries could result in excessive and dangerous amount of fluid being given during resuscitation [18] The APLS significantly underestimated the weight in children above five years in Nigeria. Its use in determining therapy in children during resuscitation might therefore result in grossly inadequate therapy which could increase morbidity and mortality. The implication is that the use of a single formula to estimate weight in children may result in a wide error. From this study, it could be suggested that the APLS formula 2(age in years +4) may be used to estimated weight in Nigerian children 1-5years in line with the Advanced Paediatric Life Support Group update [5] and Argall formula 3(age in years +2) for 6-14years.
5. Conclusions
The APLS formula significantly underestimated the weight in children above five years while Luscombe formula significantly overestimated the weights in all age groups. The Argall formula minimally overestimated the weight in all the age groups but had the least mean weight difference in children above five years. In our environment the APLS formula might be more accurate for weight estimation in children 1-5years and Argall formula for 6-14years.
Acknowledgement
Professor E.E Ekanem of Department of Paediatrics, University of Calabar Teaching Hospital is being acknowledged for proof reading the manuscript and making some useful suggestions.
Disclosure
No funding was received for this study by any of the authors and the authors have no competing interests.
References
| [1] | Argall JAW, Wright N, Mackway-Jones K, Jackson R. A comparison of two commonly used methods of weight estimation. Arch Dis Child, 88:789-790, 2003. | ||
 In article In article | View Article PubMed | ||
| [2] | Luscombe MD, Owens BD, Burke D. Weight estimation in paediatrics: a comparison of the APLS formula and the formula ‘Weight =3(age)+7’ Emerg Med J 28:590- 593, 2011. | ||
| In article | View Article PubMed | ||
| [3] | Kelly A, Nguyen K, Krieser D. Validation of the Luscombe weight formula for estimating children’s weight. Emergency Medicine Australasia, 23: 59-62, 2011. | ||
| In article | View Article PubMed | ||
| [4] | Abdel-Rahman SM, Ridge AL. An improved pediatric weight estimation strategy. The Open Medical Devices Journal, 4: 87-97, 2012. | ||
| In article | View Article | ||
| [5] | APLS 5e: FAQ: Weight Estimation. APLS Update 2013; University Hospital Coventry and Warwickshire. | ||
| In article | |||
| [6] | Luscombe M, Owens B. Weight estimation in resuscitation: is the current formula still valid? Arch Dis Child, 92:412-415. 2007. | ||
| In article | View Article PubMed | ||
| [7] | Lubitz DS, Seidel JS, Chameides L, Luten RC, Zaritsky AL, Campbell FW. A rapid method for estimating drug dosages from length in the pediatric age group. Ann Emerg Med, 17:576-81, 1988. | ||
| In article | View Article | ||
| [8] | Leffler S, Hayes M. Analysis of Parental Estimates of Children's Weights in the ED. Annals of Emergency Medicine, 30(2): 167-170.1997. | ||
| In article | |||
| [9] | Partridge RL, Abramo TJ, Haggarty KA, , Hearn R, Sutton KL, An AQ. Analysis of parental and nurse weight estimates of children in the pediatric emergency department. Pediatr Emerg Care. 25(12):816-8.2009. | ||
| In article | |||
| [10] | Ali K, Sammy I, Nunes P. Is the APLS formula used to calculate weight-for-age applicable to a Trinidadian population? BMC Emergency Medicine, 12:9.2012. http//www.biomedcentral/1471-227X/12/9. | ||
| In article | |||
| [11] | Parka J, Kwakb YH, Kimb DK, Jungb JY, Leec JH, Jangd HY et al. A new age-based formula for estimating weight of Korean children. Resuscitation, 83(9): 1129-1134. 2012. | ||
| In article | View Article PubMed | ||
| [12] | House DR, Ngetich E , Vreeman RC, Rusyniak DE. Estimating the Weight of Children in Kenya: Do the Broselow Tape and Age-Based Formulas Measure Up? Ann Emerg Med., 61:1-8. 2013. | ||
| In article | View Article PubMed | ||
| [13] | Senbanjo IO, Adeodu OO, Adejuyigbe EA Influence of socio-economic factors on nutritional status of children in a rural community of Osun State, Nigeria available at www.uib.es/congres/ecopub/ecineq/papers/235senbanjo. | ||
| In article | |||
| [14] | Nguyen K, Krieser D, Kerr D, Jolly D, Clooney M, Kelly A. Failed Validation of the Argall Weight Formula for Estimating Children’s Weight in an Australian Emergency Department. Academic Emergency Medicine. 14(5): 486-488, 2008. | ||
| In article | |||
| [15] | Geduld H, Hodkinson, PW, Wallis, LA “Validation of weight estimation by age and length based methods in the Western Cape, South Africa population,” Emergency Medicine Journal, 28: 856–860. 2010. | ||
| In article | View Article PubMed | ||
| [16] | Loo,PY, Chong SL, Lek, N Bautista D., Ng KC. Evaluation of three paediatric weght estimation methods in Singapore. Journal of Paediatric Child Health, 49(4)E 311-316. 2013. | ||
| In article | |||
| [17] | Seddon C, Lockitt L,Eisenhut M. Validation of Advanced Paediatric Life Support formulas for weight calculation in a multiethinic population. International Scholarly Research Network(ISRN) paediatrics. | ||
| In article | |||
| [18] | Anderson, M. Under-estimation potentially better than overestimation. Arch.Dis. Childhood, 92: 937-939.2007. | ||
| In article | |||
 CiteULike
CiteULike Delicious
Delicious



{kind=link}
{kind=link}
{kind=link}
{kind=link}