Background: Pancreatic ascites is a rare entity resulting from pancreatic duct leakage into peritoneum. The most common etiology is chronic pancreatitis or abdominal trauma. Case Presentation: A 23-year-old female with history of chronic pancreatitis secondary to alcohol abuse presented with acute on chronic epigastric pain with unintentional weight loss. Physical exam revealed epigastric and right upper quadrant tenderness without rebound or guarding. Labs were significant for low serum albumin and elevated lipase level. CT of abdomen without contrast demonstrated large volume ascites with normal looking pancreas. MRI of abdomen with intravenous contrast revealed two dilated tubules within the pancreatic neck communicating with the pancreatic duct, representing pancreatic fluid leakage into the peritoneal cavity. Paracentesis was performed yielding large volume of ascitic fluid with high amylase level, characteristic of pancreatic ascites. Patient was managed conservatively with bowel rest and octreotide. Conclusion: Pancreatic ascites is uncommon among the differential diagnosis of ascites. Diagnosis is suspected in a patient with chronic alcoholism or pancreatitis presenting with high amylase exudative ascites and/or pleural effusion. Though limited evidence, interventional therapy especially endoscopic procedure is recommended as initial treatment.
Ascites is the anomalous accumulation of fluid within the peritoneal cavity. In the United States, the most common etiology of ascites is cirrhosis followed by malignancy and heart failure 1. Pancreatic ascites only accounts for approximately 1% of all cases of ascites 1.
A 23-year-old woman presented to the hospital for 2-month history of nausea, vomiting and severe acute on chronic epigastric pain radiating to the back associated with 40-pound unintentional weight loss over 1-2 months, and abdominal distension. She reported no fever, chills, night sweats, diarrhea, steatorrhea, discoloration to the skin or changes in urine or stool color. Her past medical history was significant for previous admissions for acute pancreatitis on chronic pancreatitis secondary to chronic alcohol consumption with previous therapeutic paracentesis for recurrent ascites. Previous ascitic fluid was negative for cytology, had SAAG of 0.5, lipase and amylase levels were not available, and fluid lacked evidence of spontaneous bacterial peritonitis (SBP). Patient used to drink three to four beers per day before she quit one month prior to presentation. She took no medications and her family history was unremarkable.
On examination, the patient was not in acute distress, but appeared ill. Her vital signs were stable, with temperature at 97.8F, heart rate 92 bpm, blood pressure 108/67 mmHg, respiratory rate 18 breaths per minutes, and O2 saturation at 99% on room air.
There were no abnormalities on head, neck, and cardiopulmonary examination. The abdomen was soft, distended, with normoactive bowel sounds throughout, with evident epigastric and right upper quadrant tenderness to touch, without rebound or guarding. Notably, positive shifting dullness and prominent fluid wave were present. Complete blood counts and basic metabolic panels were unremarkable. Liver function tests were significant for low albumin 2.2 g/dL (normal range: 3.5-5.7 g/dL) in the setting of normal total protein level and mildly elevated aspartate aminotransferase 44 U/L (normal range: 13-39 U/L) with normal alanine transaminase, total bilirubin and alkaline phosphate level. Lipase was elevated to 251 U/L (normal range: 11-82 U/L). Coagulation test including prothrombin, activated partial thromboplastin and international normalized ratio were normal.
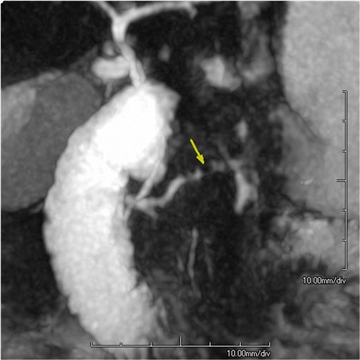
Computerized tomography (CT) of abdomen and pelvis without intravenous (IV) contrast showed large volume abdominal pelvic ascites and hepatic steatosis, however, the pancreas appeared within normal limits. Interventional radiology (IR) guided abdominal paracentesis was performed with 5-liter bloody ascitic fluid being removed. Serum ascites albumin gradient (SAAG) was 0.7 g/dL. Total protein, amylase, and lipase were 3.4 g/L, 3466 U/L, and >6000 U/L, respectively, suggestive of pancreatic ascites. Peritoneal fluid also showed no malignant cells, lacked evidence of SBP, and Adenosine deaminase (ADA) levels, although elevated at 22.7 U/L, were not significant enough to indicate peritoneal tuberculosis, which is usually 36 U/L. Cytopathology result was negative for malignant cell. Magnetic resonance imaging (MRI) of the abdomen and magnetic resonance cholangiopancreatography (MRCP) with IV contrast revealed dilated tubular structures within the pancreatic neck, possibly communicating with the non-dilated main pancreatic duct, representing an area of pancreatic necrosis or pseudocyst formation bisecting the pancreas without evidence of pancreatic mass (Figure 1).
Meanwhile, patient was managed conservatively with octreotide and bowel rest. She declined total parenteral nutrition. Endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy and stent placement was offered to patient for pancreatic duct leak, however the patient refused intervention. A second IR guided therapeutic paracentesis was performed during the hospital stay for symptomatic relief with 4.8 liters of ascitic fluid removal. Peritoneal fluid results were consistent with previous diagnosis of pancreatic ascites. Follow-up MRI abdomen with IV contrast revealed persistent pancreatic duct leak at the neck of the pancreas with two dilated tubular structures measuring 1cm x 8mm, and 8mm x 2 cm, with possible communication to the pancreatic duct.
Extensive discussions about the risk and benefits of different management modalities including total parenteral nutrition, enteral tube feeding, surgical or endoscopic intervention were carried out with the patient, however she declined interventions. Patient was discharged with appointment with GI clinic and abdominal scan follow-up within 6 months.
Pancreatic ascites was first reported in 1953 by Dr. Earl Belle Smith, who reported two cases of ascites associated with chronic pancreatitis 2. Pancreatic ascites is a rare entity defined as accumulation of pancreatic fluid in the peritoneal cavity and secondary to leakage of pancreatic secretions due to pancreatic duct injury 3. It is characterized as exudative ascites with SAAG less than 1.1, very high amylase (usually above 1000 IU/L) and protein (over 3 g/dL) level in ascitic fluid 4.
Minor pancreatic duct injuries result in peripancreatic fluid collection, which leads to formation of a pseudocyst. Major pancreatic duct injury, when complicated by pancreatic necrosis, could delay the resorption of walled-off necrosis due to leakage of pancreatic fluid into necrosis. The presence of local complications of pancreatitis, like pseudocyst or walled-off necrosis, increases the risk of pancreatic ascites. Another local aberration that can cause pancreatic ascites is persistent fistula into the peritoneum. Pancreatic fistulas could result from blunt abdominal trauma, ductal lithiasis, ampullary stenosis or iatrogenic causes, like ERCP or pancreatic biopsy 5, 6, 7, 8. In a case series with 185 pancreatic ascites patients, the most common etiology was chronic pancreatitis, followed by pancreatic trauma 9.
Although the exact prevalence is unknown given its low incidence, pancreatic ascites was reported to be present in 4% of chronic pancreatitis cases and 6-14% of pseudocyst cases 10. The majority of the cases are seen among men (male: female ratio of 2:1) into their second to fifth decades of life 9. Clinically, pancreatic ascites can present with increased abdominal girth, weight loss, early satiety and shortness of breath due to concomitant high amylase pleural effusion resulting from pancreatic-pleural fistulas 11. Severe abdominal pain or peritoneal symptoms were typically absent, particularly in alcoholics 4, 12.
Given the digestive function of pancreatic enzymes, pancreatic ascites could cause potentially debilitating or fatal digestion of tissues within the peritoneal cavity. Historically, minimizing pancreatic secretion through total parenteral nutrition, avoiding enteral feeding and somatostatin analog such as octreotide, administration of diuretics, and evacuation of effusions and ascites through thoracentesis and paracentesis were the mainstem conservative treatment 13. Patients who do not respond to conservative treatment within 6 weeks would proceed to surgery, including resecting the leaking part of the pancreas, cyst-gastrostomy, or Roux-en-Y cyst-jejunostomy if a pseudocyst was present. However, this approach had led to 10-15% overall mortality rate, 15-25% recurrent rate and 56% failure rate 12, 13. The risk factors for failure of conservative therapy include severity of pancreatic duct disease seen on ERCP, including the presence of more than one site of contrast extravasation, and degree of biochemical abnormalities on admission labs, including hyponatremia, low serum albumin level and a higher ratio of ascitic fluid protein to total serum protein levels 14.
Given high failure rate of conservative treatment, interventional therapy, including surgery or endoscopy, were strongly recommended as the initial treatment option lately 15. In a recent case series including 139 pancreatic ascites patients, interventional therapy has shown beneficial effects in clinical outcomes compared to conservative therapy 4. Endoscopic trans-papillary stenting or sphincterotomy through ERCP to relieve intraductal pressure is an increasingly well-described treatment approach with high success rate (85.7%) and low mortality (0%) than surgery (87.2% success rate and 7.7% mortality rate) or conservative therapy 4. Until now, no randomized controlled trials have been performed to validate the optimal treatment strategy for pancreatic ascites given its rarity.
In a nutshell, pancreatic ascites is an uncommon cause of ascites and should be considered among the possible diagnosis in patients with chronic alcoholism, pancreatitis, or abdominal trauma history. Pancreatic ascites could constitute a therapeutic challenge given limited reported evidence, however, interventional strategy including endoscopic trans-papillary stenting or sphincterotomy, should be strongly considered as the initial treatment with higher successful rate and low mortality rate.
This work is supported in part by Dr. Moro O. Salifu’s efforts through NIH Grant # S21MD012474.
| [1] | Runyon BA, Montano AA, Akriviadis EA, Antillon MR, Irving MA, McHutchison JG, “The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites,” Ann Intern Med, 117(3): 215-220, 1992. | ||
| In article | View Article PubMed | ||
| [2] | Smith EB, “Hemorrhagic Ascites and Hemothorax Associated with Benign Pancreatic Disease,” AMA Archives of Surgery, 67(1): 52-56, 1953. | ||
| In article | View Article PubMed | ||
| [3] | Lipsett PA, Cameron JL, “Internal pancreatic fistula,” Am J Surg, 163(2): 216-220, 1992. | ||
| In article | View Article | ||
| [4] | Gómez-Cerezo J, Barbado Cano A, Suárez I, Soto A, Ríos JJ, Vázquez JJ, “Pancreatic ascites: study of therapeutic options by analysis of case reports and case series between the years 1975 and 2000,” Am J Gastroenterol, 98(3):568-577, 2003. | ||
| In article | View Article PubMed | ||
| [5] | Williet N, Kassir R, Cuilleron M, Dumas O, Rinaldi L, Augeul-Meunier K, Cottier M, Roblin X, Phelip JM, “Difficult endoscopic diagnosis of a pancreatic plasmacytoma: Case report and review of literature,” World J Clin Oncol, 8(1):91-95, 2017. | ||
| In article | View Article PubMed | ||
| [6] | Kapoor VK, “Complications of pancreato-duodenectomy,” Rozhl Chir, 95(2): 53-59, 2016. | ||
| In article | |||
| [7] | Larsen M, Kozarek R, “Management of pancreatic ductal leaks and fistulae,” J Gastroenterol Hepatol, 29(7): 1360-1370, 2014. | ||
| In article | View Article PubMed | ||
| [8] | Saâda E, Follana P, Peyrade F, Mari V, François E, “Pathogenesis and management of refractory malignant ascites,” Bull Cancer, 98(6): 679-687, 2011. | ||
| In article | View Article PubMed | ||
| [9] | Broe PJ CJ, “Pancreatic ascites and pancreatic pleural effusions,” in Complications of pancratitis Medical and surgical management. edn. Edited by Bradley EL e. Philadelphia WB Saunders 1982: 245-264. | ||
| In article | |||
| [10] | Brooks JR, “Pancreatic ascites” in Surgery of the Pancreas edn. Edited by Brooks JR. Phiadelphia: WB Saunders; 1983: 230-232. | ||
| In article | |||
| [11] | Sankaran S, Walt AJ, “Pancreatic Ascites: Recognition and Management,” Archives of Surgery, 111(4):430-434, 1976. | ||
| In article | View Article PubMed | ||
| [12] | Lipsett PA, Cameron JL, “Internal pancreatic fistula,” The American Journal of Surgery, 163(2):216-220, 1992. | ||
| In article | View Article | ||
| [13] | Kozarek RA, “Management of pancreatic ascites,” Gastroenterol Hepatol (NY), 3(5):362-364, 2007. | ||
| In article | |||
| [14] | Schneider Bordat L, El Amrani M, Truant S, Branche J, Zerbib P, “Management of pancreatic ascites complicating alcoholic chronic pancreatitis,” J Visc Surg, 2021. | ||
| In article | View Article PubMed | ||
| [15] | Karlapudi S, Hinohara T, Clements J, Bakis G, “Therapeutic challenges of pancreatic ascites and the role of endoscopic pancreatic stenting,” BMJ Case Rep, 2014. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2021 Tian Li, Clara E. Wilson, Harry Zinn, Moro O. Salifu and Isabel M. McFarlane
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Runyon BA, Montano AA, Akriviadis EA, Antillon MR, Irving MA, McHutchison JG, “The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites,” Ann Intern Med, 117(3): 215-220, 1992. | ||
| In article | View Article PubMed | ||
| [2] | Smith EB, “Hemorrhagic Ascites and Hemothorax Associated with Benign Pancreatic Disease,” AMA Archives of Surgery, 67(1): 52-56, 1953. | ||
| In article | View Article PubMed | ||
| [3] | Lipsett PA, Cameron JL, “Internal pancreatic fistula,” Am J Surg, 163(2): 216-220, 1992. | ||
| In article | View Article | ||
| [4] | Gómez-Cerezo J, Barbado Cano A, Suárez I, Soto A, Ríos JJ, Vázquez JJ, “Pancreatic ascites: study of therapeutic options by analysis of case reports and case series between the years 1975 and 2000,” Am J Gastroenterol, 98(3):568-577, 2003. | ||
| In article | View Article PubMed | ||
| [5] | Williet N, Kassir R, Cuilleron M, Dumas O, Rinaldi L, Augeul-Meunier K, Cottier M, Roblin X, Phelip JM, “Difficult endoscopic diagnosis of a pancreatic plasmacytoma: Case report and review of literature,” World J Clin Oncol, 8(1):91-95, 2017. | ||
| In article | View Article PubMed | ||
| [6] | Kapoor VK, “Complications of pancreato-duodenectomy,” Rozhl Chir, 95(2): 53-59, 2016. | ||
| In article | |||
| [7] | Larsen M, Kozarek R, “Management of pancreatic ductal leaks and fistulae,” J Gastroenterol Hepatol, 29(7): 1360-1370, 2014. | ||
| In article | View Article PubMed | ||
| [8] | Saâda E, Follana P, Peyrade F, Mari V, François E, “Pathogenesis and management of refractory malignant ascites,” Bull Cancer, 98(6): 679-687, 2011. | ||
| In article | View Article PubMed | ||
| [9] | Broe PJ CJ, “Pancreatic ascites and pancreatic pleural effusions,” in Complications of pancratitis Medical and surgical management. edn. Edited by Bradley EL e. Philadelphia WB Saunders 1982: 245-264. | ||
| In article | |||
| [10] | Brooks JR, “Pancreatic ascites” in Surgery of the Pancreas edn. Edited by Brooks JR. Phiadelphia: WB Saunders; 1983: 230-232. | ||
| In article | |||
| [11] | Sankaran S, Walt AJ, “Pancreatic Ascites: Recognition and Management,” Archives of Surgery, 111(4):430-434, 1976. | ||
| In article | View Article PubMed | ||
| [12] | Lipsett PA, Cameron JL, “Internal pancreatic fistula,” The American Journal of Surgery, 163(2):216-220, 1992. | ||
| In article | View Article | ||
| [13] | Kozarek RA, “Management of pancreatic ascites,” Gastroenterol Hepatol (NY), 3(5):362-364, 2007. | ||
| In article | |||
| [14] | Schneider Bordat L, El Amrani M, Truant S, Branche J, Zerbib P, “Management of pancreatic ascites complicating alcoholic chronic pancreatitis,” J Visc Surg, 2021. | ||
| In article | View Article PubMed | ||
| [15] | Karlapudi S, Hinohara T, Clements J, Bakis G, “Therapeutic challenges of pancreatic ascites and the role of endoscopic pancreatic stenting,” BMJ Case Rep, 2014. | ||
| In article | View Article PubMed | ||



{kind=link}