Diagnosing a rare disease is challenging but unravelling the rare findings of a common disease is motivating! One such common disease dealt in the case report below is Amoebiasis. Amoebiasis is a major public health problem worldwide. Mortality due to amebiasis is mostly by extra intestinal infections, amebic liver abscess being the most common one. Overall, 10% of the world’s population is infected with Entamoeba histolytica (E. histolytica) but out of this only 1% becomes symptomatic. Nearly 20% of the Indian population show manifestations of the disease. With this background epidemiological prevalence, we present an unusual case of a 30year old male with a ruptured amoebic liver abscess into the pericardium.
The most common presentation of Amoebiasis is Amoebic Dysentery. Due to the tissue invasiveness of the causative organism, it is also known to cause extraintestinal manifestations like amoebic liver abscess. The incidence of amoebic liver abscess formation is (3-9)% of all cases of amoebiasis 3. Amoebic liver abscess may rupture into pleura, lungs, pericardium, peritoneum or brain. The incidence of hepato-pericardial fistula leading to pyopericardium is extremely rare. Only 27 such cases have been reported worldwide till date. We report a case of young male presenting with ruptured amoebic liver abscess into the pericardium.
A 30-year-old male, chronic alcoholic, without any particular pathological antecedents, presented to the casualty with a history of retrosternal, dull aching chest pain for 3 days which was gradually progressive thus, incapacitating him to walk or sit comfortably. The history mimicked an acute coronary event, as the pain was also associated with dyspnea and palpitation. On general examination, his Heart rate was 130 beats/min and respiratory rate was 30/min with a low volume pulse and blood pressure of 90/60 mmHg. His Jugular Venous Pressure (JVP) was high and Kussmaul’s sign was positive. Cardiovascular examination showed muffled heart sounds on auscultation. On Abdominal examination, he had severe right hypochondriac tenderness and a palpable Liver (Liver span - 17cm).
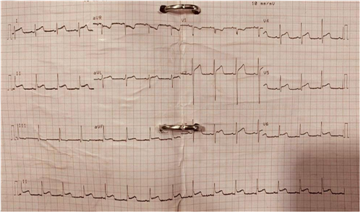
His ECG showed diffuse ST segment elevation in all the limb leads and chest leads, not pertaining to any single coronary arterial territory involvement, as shown in the figure below (Figure 1).
The qualitative troponin I test was negative. Emergency Bedside echocardiography showed early signs Cardiac Tamponade with preserved left ventricular systolic function and no regional wall motion abnormality.
The patient was immediately taken up for pericardiocentesis under fluoroscopic guidance and 700 ml of thick dark chocolate brown fluid was aspirated, as shown in the figure below (Figure 2). The aspirate was sent for microbiological analysis. The laboratory values are as shown below (Table 1).

On the second day since admission (post procedure), he complained of severe breathlessness. The repeat echocardiography revealed recurrence of tamponade. A pigtail drain was placed in situ which drained atleast 600 -700 ml aspirate per day.
Based on the cues from above findings, hunt for the primary source of abscess began. Contrast Enhanced Computed Tomography (CECT) Chest, Abdomen & Pelvis revealed a subdiaphragmatic collection (151 mL) indenting the left lobe of liver inferiorly and superiorly communicating the pericardial space. Other findings were mild ascites, mild hepatomegaly, moderate bilateral pleural effusion, mediastinal and abdominal adenopathy and gross pericardial effusion.
All the test results raised the suspicion of an amoebic liver abscess rupture into the pericardium via a hepato-pericardial fistula as the closest diagnosis. It was confirmed by positive Amoebic serology.
Eventually, the patient was started on Intravenous Metronidazole at a dose of 2 g/day in divided doses for next 14 days. He was also started on enzymatic preparations of trypsin, chymotrypsin and Serratiopeptidase to subside the associated inflammation. On the seventh day since admission, he started showing signs of recovery. His vital parameters normalized, and the drain collection gradually decreased to nil amount by the tenth say since admission. The drain was removed on the twelfth day and he was discharged from the hospital with complete recovery. He regularly follows up in the Medicine Outpatient Department (OPD) every 15 days.
Over the past years, it has been observed that Amoebiasis is a relatively benign condition with no symptoms unless intestinal involvement turns predominant. The strain virulence, environment, host’s genetic susceptibility, immune status, age, and gender determine the prognosis of the illness 4.
A case of Ruptured Amoebic Liver Abscess presenting as Cardiac Tamponade was reported recently that presented with deranged Liver function and gradually progressed to bilateral empyema. Eventually, bilateral pigtail drains were inserted through the chest wall and Cultures demonstrated superadded Acinetobacter baumanii infection. The medical management revolved around Metronidazole covered by restricted Antibiotics like Colistin 5.
Two large case series of hepatic amebic abscesses have been published. One spanning over 18 years by Carlos et al. examined 501 cases of amebic liver abscess. There were 326 cases of rupture through the diaphragm with 5 cases (0.01%) rupturing into the pericardium and 1 case rupturing into both pleural and pericardial cavities. The second such study from China by Meng et al. reported 503 cases of amebic liver abscess over 21 years 6.
Treatment of amebic liver abscess depends on the severity at presentation and on the associated complications. Most early, small, and uncomplicated abscesses can be treated by medical therapy alone. Drainage when required has been done in different ways according to the presentation of the patient 7, 8. Cases of pericardial rupture of an amebic liver abscess developing cardiac tamponade similar to this case and relieved by pericardiotomy have been reported 8. On the other hand, intra-pericardial ruptures have been managed only by percutaneous drainage when emergency intervention is not necessitated by development of cardiac tamponade 9.
Therapeutic aspiration by imaging-guided percutaneous interventions (needle aspirations, pigtail catheters) of liver abscess should be contemplated in a patient with a high risk of rupture that includes large abscess (cavity diameter > 5 cm), left lobe abscess due to risk of rupture into the pericardial sac, and liver abscess resistant to 5-7 days of medical management 10.
Amoebic Liver abscess has been shown to develop into unexpected complications which may require aggressive management. Rapid diagnosis of the disease is not just sufficient. Early treatment and regular follow up can help predict these complications at an earlier stage thus warranting the desired mode of management and saving lives of many! Despite the disease being a relatively benign condition, late diagnosis may create heavy casualties which may be life threatening. This case highlights one such catastrophic complication of untreated hepatic amebiasis presenting with cardiac tamponade.
It gives us immense pleasure to present our acknowledgement, a token of appreciation to all the persons involved directly and indirectly with the preparation of our case report. We are extremely grateful to our beloved teacher and guide, Dr. S H Talib, Prof Emeritus & Chief Advisor, Department of Medicine, M.G.M. Medical College and Hospital, Aurangabad and Dr. Prashant Udgire, Professor, Department of Cardiology, M.G.M Medical College and Hospital, Aurangabad for their able guidance, supervision, invaluable suggestions and kind help rendered throughout the preparation of this case report.
| [1] | Haque R, Huston CD, Hughes M, Erik H, Petri WA Jr. Amebiaisis. N Engl J Med. 2003; 348: 1565-73. | ||
| In article | View Article PubMed | ||
| [2] | Rani R, Murthy RS, Bhattacharya S, Ahuja V, Rizvi MA, Paul J. Changes in bacterial profile during amebiasis: demonstration of anaerobic bacteria in ALA pus samples. Am J Trop Med Hyg. 2006; 75(5): 880-5. | ||
| In article | View Article PubMed | ||
| [3] | Jackson-Akers JY, Prakash V, Oliver TI. Amebic Liver Abscess. [Updated 2020 Apr 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430832/. | ||
| In article | |||
| [4] | Bernin H, Marggraff C, Jacobs T, Brattig N, An LV, Blessmann J et al. Immune markers characteristic for asymptomatically infected and diseased Entamoeba histolytica individuals and their relation to sex. BMC Infect Dis 2014; 14: 621. | ||
| In article | View Article PubMed | ||
| [5] | Cliojis Francis, Swati Soni, Anunay Gupta, Sourabh Agstam, A case report of ruptured amoebic liver abscess causing cardiac tamponade and requiring pericardial window, European Heart Journal - Case Reports, ytaa 182. | ||
| In article | |||
| [6] | Ibarra-Perez C. Thoracic complications of amebic abscess of the liver: Report of 501 cases. Chest 1981; 79: 672-7. | ||
| In article | View Article PubMed | ||
| [7] | Chandran SR, Balakrishnan RK, Chinnaswamy B, Srinivasan GK. Ameobic hepatopericardial fistula causing cardiac tamponade. Ann Trop Med Public Health 2012 ; 5:387-9. | ||
| In article | View Article | ||
| [8] | Miyauchi T, Takiya H, Sawamura T, Murakami E. Cardiac tamponade due to intrapericardial rupture of an amebic liver abscess. Jpn J Thorac Cardiovasc Surg 2005; 53: 206-9. | ||
| In article | View Article PubMed | ||
| [9] | Takhtani D, Kalagara S, Trehan MS, Chawla Y, Suri S. Intrapericardial rupture of amebic liver abscess managed with percutaneous drainage of liver abscess alone. Am J Gastroenterol 1996; 91: 1460-2. | ||
| In article | |||
| [10] | Shamsuzzaman SM, Hashiguchi Y. Thoracic amebiasis. Clin Chest Med 2002; 23: 479-492. | ||
| In article | View Article | ||
Published with license by Science and Education Publishing, Copyright © 2020 Richa Rajput, Abhinav Chhabra and Rohit Jacob
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Haque R, Huston CD, Hughes M, Erik H, Petri WA Jr. Amebiaisis. N Engl J Med. 2003; 348: 1565-73. | ||
| In article | View Article PubMed | ||
| [2] | Rani R, Murthy RS, Bhattacharya S, Ahuja V, Rizvi MA, Paul J. Changes in bacterial profile during amebiasis: demonstration of anaerobic bacteria in ALA pus samples. Am J Trop Med Hyg. 2006; 75(5): 880-5. | ||
| In article | View Article PubMed | ||
| [3] | Jackson-Akers JY, Prakash V, Oliver TI. Amebic Liver Abscess. [Updated 2020 Apr 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430832/. | ||
| In article | |||
| [4] | Bernin H, Marggraff C, Jacobs T, Brattig N, An LV, Blessmann J et al. Immune markers characteristic for asymptomatically infected and diseased Entamoeba histolytica individuals and their relation to sex. BMC Infect Dis 2014; 14: 621. | ||
| In article | View Article PubMed | ||
| [5] | Cliojis Francis, Swati Soni, Anunay Gupta, Sourabh Agstam, A case report of ruptured amoebic liver abscess causing cardiac tamponade and requiring pericardial window, European Heart Journal - Case Reports, ytaa 182. | ||
| In article | |||
| [6] | Ibarra-Perez C. Thoracic complications of amebic abscess of the liver: Report of 501 cases. Chest 1981; 79: 672-7. | ||
| In article | View Article PubMed | ||
| [7] | Chandran SR, Balakrishnan RK, Chinnaswamy B, Srinivasan GK. Ameobic hepatopericardial fistula causing cardiac tamponade. Ann Trop Med Public Health 2012 ; 5:387-9. | ||
| In article | View Article | ||
| [8] | Miyauchi T, Takiya H, Sawamura T, Murakami E. Cardiac tamponade due to intrapericardial rupture of an amebic liver abscess. Jpn J Thorac Cardiovasc Surg 2005; 53: 206-9. | ||
| In article | View Article PubMed | ||
| [9] | Takhtani D, Kalagara S, Trehan MS, Chawla Y, Suri S. Intrapericardial rupture of amebic liver abscess managed with percutaneous drainage of liver abscess alone. Am J Gastroenterol 1996; 91: 1460-2. | ||
| In article | |||
| [10] | Shamsuzzaman SM, Hashiguchi Y. Thoracic amebiasis. Clin Chest Med 2002; 23: 479-492. | ||
| In article | View Article | ||




{kind=link}
{kind=link}