Background: Due to concerns about uncontrolled hemorrhage and peripartum hysterectomy, routine myomectomy at the time of caesarean section has historically been denounced. That is still a hotly contested subject everywhere. Nonetheless, numerous case reports of caesarean myomectomy have recently been published, proving their safety and the absence of any serious sequelae. Case presentation: A 34 years old gravid 3 para2 with one previous caesarean section (CS) presented with a complains of passage of liquor per vaginum for10 hours which was yellow in color and odorless accompanied by mild abdominal cramp. Gestational age calculated from early ultrasound was 40weeks. She hads regular antenatal care (ANC) follow up and pregnancy was planned, wanted, and supported. The most recent ultrasonography (USG) result indicated a single viable intrauterine pregnancy and an intramural fibroid measuring 8.6 by 6.1 cm in the lower uterine segment's left anterolateral wall. Due of the fibroid's protrusion into the incision line and fear off wound dehiscence and delay in uterine wound healing post-surgery, the decision of myomectomy was taken. In order to prevent post-partum hemorrhage, proflacis oxytocin infusion treatment were given. Conclusions: If conducted safely, it can avert the additional morbidity of a future operation, justifying the procedure's cost-effectiveness.
Leiomyomas are the most prevalent benign reproductive tract tumors in women of childbearing age. It's difficult to say how often they are throughout pregnancy. However, the literature indicates an incidence of 2-4%. 1. Uterine fibromyomas affect a large number of women accounting for significant morbidity and health care costs during reproductive age. 2, 3 The incidence is increasing as a result of delayed childbearing and a substantial increase in the number of cesarean sections in recent years. In pregnant women with increased maternal age there is high incidence of Myoma, Hence the possibility to encounter pregnant patients with myomas and the need to treat the associated complications is also rising 4, 5
Uterine fibroids tend to occur less frequently before puberty, more regularly during the reproductive years, and shrink in size after menopause in a woman's life cycle. 6 Uterine fibroids are classified into major three types according to their position, intramural, submucous and subserous and their positions play a role in the present symptoms. 7 The vast majority of individuals are asymptomatic or have minimal symptoms and require just conservative treatment. Menorrhagia, pelvic pain with or without dysmenorrhea or pressure symptoms, infertility, and recurrent pregnancy loss are the common symptoms and complications that women with fibroids may experience. 7
Management of myoma during caesarean section remains controversial issue despite progress in medical and non-surgical myoma treatment 8. Myomectomy is the most common operation performed during cesarean section and accounts for 0.89% of all cesarean sections. 9
Due to increased vascularity of the gravid uterus, which leads to significant hemorrhage, needless obstetric hysterectomy, and increased perioperative morbidity and mortality, myomectomy during cesarean section is typically avoided. However, with advances in anesthesia, adequate blood product availability, selective devascularization techniques, and a multidisciplinary approach in modern obstetrics, obstetricians are increasingly choosing to perform myomectomy during cesarean section, saving the patient from future morbidity due to multiple surgeries, anesthetic complications, and out-of-pocket expenditure. 10. Myomectomy during cesarean section was not found in obstetrics literature until recently and it was widely suggested to postpone the myomectomy and perform it later before the next pregnancy. 11 The most common reason for postponing myomectomy has been prevention of unwanted hysterectomy due to uncontrolled hemorrhage that adds to post-operative morbidity and increased hospital stay. 11, 12 It’s easy to remove pedunculated myomas and hemostasis can be achieved without much difficulty. A patient who undergoes myomectomy during cesarean section will not require a second operation. In addition, cesarean myomectomy also promotes puerperal involution and significantly reduces fibroid related complications that can develop later in life such as menorrhagia, anemia due to heavy bleeding and pain. 13
We provide a case of a successful myomectomy performed during an emergency cesarean delivery with no sequelae. We intend to deviate from the customary practice of avoiding myomectomy at the time of cesarean section and consider it after thorough case selection.
34 years old gravid 3 para2 with one previous caesarean section (CS) presented with a complains of passage of liquor per vaginum for10 hours which was yellow in color and odorless accompanied by mild abdominal cramp. Gestational age calculated from early ultrasound was 40weeks. She hads regular antenatal care (ANC) follow up and pregnancy was planned, wanted, and supported.
On arrival, her heart rate was 102 beats per minute, blood pressure was 110/70 mmHg, and slight pallor was observed. Abdominal examination indicated a term size uterus with longitudinal lying. Positive scar soreness was observed along with light uterine contractions. Fetal heart rate was 142 beats per minute during auscultation. A 2 cm dilated cervix that was 20–30% effaced and showing part at three stations with intact membranes was seen during a vaginal examination.
A single live intrauterine pregnancy was seen in her most recent ultrasound (USG) scan, along with an intramural fibroid measuring 8.6 by 6.1 cm in the uterus Left anterolateral wall of the lower uterine segment. Her preoperative hemoglobin level was 12.1gm/dl, hematocrit was 39.2%, and she had a negative blood group B.
The patient and her family members were informed about the risk of severe bleeding, the necessity for blood transfusion, and the peripartum hysterectomy before adequate blood products were arranged and informed written and inforemed consent was taken from them.
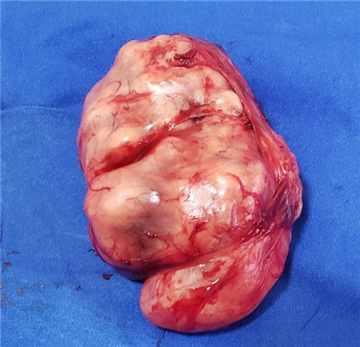
The abdomen was opened vertically in the infra-umbilical region to provide for adequate access during surgery. A single, large fibroid occupied the majority of the lower uterine segment's intramural space. The previous scar was still there, but it had thinned as a result of the fibroid's stretching effects. At one minute after a lower segment transverse incision was made below the inferior edge of the fibroid, a female newborn weighing 2.54 kg was delivered with an APGAR score of 9. Then after mayomectomy was done safly .The decision to perform a myomectomy was made due to the fibroid's protrusion into the incision line and the risk of wound dehecense and delayed uterine wound healing following surgery (Figure 1). In order to prevent post partum hemmorage, proflaxis oxytocin infusion treatment was given.post operatively the patiant was cofrtable, stable vital sign, no significant vaginal bleeding, and abdomen soft move with respiration.post oprative and post transfution (2unit Packed RBC) hematocrit was 33.6%, and hemogloblin 11.2gm/dl. Next day she start feeding and toleratethen discharged after 5 days with out any complication. On follow up vist the she has no any compliant and Other detacted complication.


Pregnancy with fibroid is a high-risk situation. Although the majority of such cases are asymptomatic or have mild symptoms, 10–40% of cases can present with antenatal complications in the form of pregnancy loss, degenerative changes, malpresentation, abruption placenta, preterm labor, dysfunctional labor or uterine inertia, and increased chances of operative delivery, thus increasing maternal and fetal morbidity and mortality 14. Treatment is usually conservative during the antenatal period in the form of bed rest, adequate hydration, and analgesics. Rarely is a myomectomy necessary when the patient has severe abdominal pain brought on by a twisted pedunculated sub-serosal fibroid, red degeneration that is resistant to conservative treatment, or a significantly massive myoma. 15. In a recent study, a successful myomectomy was performed during the first trimester at 11 weeks for a large myoma of 14 cm that was a cause of severe discomfort to the patient 16. The patient continued with pregnancy to term and delivered a healthy baby. Another case of successful myomectomy performed in the second trimester for a large subserous fibroid, weighing 3900 g and causing severe pressure symptoms and subacute intestinal obstruction, is described. The pregnancy continued uneventfully until term. 17. Myomectomy during cesarean section is still a topic of debate in the modern era. Except for pedunculated sub-serosal fibroids, it was regarded a dreadful surgery until the previous decade. Many studies, however, have determined that the operation is not risky and does not result in complications when performed by a qualified obstetrician. 18. Kwawukume performed cesarean myomectomies on 12 patients and reported that enucleation was much easier in pregnancy due to increased softness of the tissue 19. A retrospective case–control study, comparing 40 women with fibroids who underwent cesarean myomectomy with 80 women with fibroids forming the control group who underwent cesarean section alone, reported no significant difference in the incidence of hemorrhage between the two groups (12.5% and 11.3%, respectively) 20. Similar findings were reported in another study, with no significant differences in hemoglobin levels, incidence of blood transfusions, or postoperative pyrexia. However, not all myomas need to be removed, but only those causing difficulty in delivery of the fetus or wound closure and sub-serosal fibroids. In our case, myomectomy was inevitable as the myoma was in the incision line, making wound closure impossible. Every possible effort should be made to reduce the blood loss. Bilateral ligation of uterine arteries immediately after delivery of the fetus significantly reduces both intraoperative and postoperative blood loss and risk of peripartum hysterectomy 21. It also reduces the recurrence of myomas and minimizes the need for future surgery, with no apparent effect on fertility 22. This was a key step in our case which prevented the dreaded complications.
The procedure's cost-effectiveness is justified if it is performed safely because it can prevent the additional morbidity of a subsequent operation. One cannot, however, undervalue the value of a skilled obstetrician, a facility with enough staff and blood supplies, and cautious case selection.
Consent: The customers' written informed consent was obtained, including permission to publish this information and the usage of photos.
We would like to extend our sincere gratitude to all the people and organizations who have helped make this study paper available; they are deserving of our greatest appreciation. First off, I want to express my gratitude to Dr. Mebrahtu Gember, a senior obstetrician and gynecologist who performed the cesarean myomectomy and provided us with a sound assignment guideline over multiple meetings.
| [1] | Ardovino M, Ardovino I, Castaldi MA, Monteverde A, Colacurci N, Cobellis L. Laparoscopic myomectomy of a subserous pedunculated fibroid at 14 weeks of pregnancy: a case report. J Med Case Rep. 2011; 5:2–6. | ||
| In article | View Article PubMed | ||
| [2] | Sparic R, Mirkovic L, Malvasi A, Tinelli A. Epidemiology of uterine myomas: A review. Int J Fertil Steril.2016;9:424-35. | ||
| In article | |||
| [3] | Cardozo ER, Clark AD, Banks NK, Henne MB, Stegmann BJ, Segars JH. Theestimated annual cost of uterine leiomyomata in the United States. Am J Obstet Gynecol.2012; 206:211. e1-211 | ||
| In article | View Article PubMed | ||
| [4] | Coronado GD, Marshall LM, Schwartz SM. Complications in pregnancy, labor, and delivery with uterine leiomyomas: a population-based study.Obstet Gynecol.2000;95:764-9. | ||
| In article | View Article PubMed | ||
| [5] | Neiger R, Sonek JD, Croom CS. Pregnancy related changes in the size of uterine leiomyomas.J Reprod Med.2006;51:671-4. | ||
| In article | |||
| [6] | Cruz MSDDL, Buchanan EM: Uterine fibroids: diagnosis and treatment. Am Fam Physician. 2017, 95:100-7. | ||
| In article | |||
| [7] | McWilliams MM, Chennathukuzhi VM: Recent advances in uterine fibroid etiology. Semin Reprod Med. 2017, 35:181-9. 10.1055/s-0037-1599090. | ||
| In article | View Article PubMed | ||
| [8] | Sparic R, Nejkovic L, Mutavdzic D, Malvasi A, Tinelli A. Conservative surgical treatment of fibroids. Acta Chir Iugosl.2014;61:11-66. | ||
| In article | View Article | ||
| [9] | Baloniak B, Jasinskil O, Prews K. Slomko Z. Morphologic pattern of uterine myomas enucleated at cesarean section. Clinical Pol. 2002;73(4):255. | ||
| In article | |||
| [10] | Kathpalia SK, Arora D, Vasudeva S, Singh S. Myomectomy at cesarean section: a safe option. Med J Armed Forces India. 2016;72: S161–S163. | ||
| In article | View Article PubMed | ||
| [11] | Kwawkume EY. Myomectomy during cesarean section. IntJGynObs. 2003;76:183-4. | ||
| In article | View Article PubMed | ||
| [12] | Cohellis L, Florio P, Stradella L, Lulia EP. Electro-cautery of myomas during cesarean section, two cases reports. EuJ Obs Gyn Rep Biol. 2002. | ||
| In article | View Article PubMed | ||
| [13] | Kwawukume EY. Caesarean myomectomy.Afr J Reprod Health.2002;6:38-43. | ||
| In article | View Article PubMed | ||
| [14] | Obstet Gynecol Clin North Am 2006 Mar;33(1): 153-69. | ||
| In article | |||
| [15] | Ardovino M, Ardovino I, Castaldi MA, Monteverde A, Colacurci N, Cobellis L. Laparoscopic myomectomy of a subserous pedunculated fbroid at 14 weeks of pregnancy: a case report. J Med Case Rep. 2011; 5:2–6. | ||
| In article | View Article PubMed | ||
| [16] | Leach K, Khatain L, Tocce K. First trimester myomectomy as an alternative to termination of pregnancy in a woman with a symptomatic uterine leiomyoma: a case report. J Med Case Rep. 2011; 5:2–5. | ||
| In article | View Article PubMed | ||
| [17] | Bhatla N, Dash BB, Kriplani A, Agarwal N. Myomectomy during pregnancy: a feasible option. J Obstet Gynaecol Res. 2009;35(1):173–175. | ||
| In article | View Article PubMed | ||
| [18] | Guler AE, Guler ZÇD, Kinci MF, Mungan MT. Myomectomy during cesarean section: why do we abstain from? J Obstet Gynecol India. 2020. | ||
| In article | View Article PubMed | ||
| [19] | Kwawukume E. Myomectomy during cesarean section. Int J Gynecol Obstet. 2002;76(2):183–4. | ||
| In article | View Article PubMed | ||
| [20] | Kaymak O, Ustunyurt E, Okyay RE, Kalyoncu S, Mollamahmutoglu L. Myomectomy during cesarean section. Int J Gynecol Obstet. 2005;89(2):90–3. | ||
| In article | View Article PubMed | ||
| [21] | Lopes T, Spirtos N, Naik R. Monaghan J. Uterine fibroids. In: Bonney’s Gynaecological Surgery. 11th ed. Chichester: Blackwell; 2010. | ||
| In article | View Article | ||
| [22] | Liu WM, Wang PH, Tang WL, Te WI, Tzeng CR. Uterine artery ligation for treatment of pregnant women with uterine leiomyomas who are undergoing cesarean section. Fertil Steril. 2006;86(2):423–8. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2023 Bethel Tesfaye Bizuneh, Tewodros Kassahun Tarekegn, Hayat Yassin Nuri, Evelyn Cantillo Aguila, Efrata Sentayehu Teshome, Adey Gizachew Alemayehu, Tereza Mulatu Tafesse, Rediet Habtu Lebelo, Solomon Endale Dagnachew, Erdachew Gallo Beyene, Rediet Abebe Mekonnen, Michael Million Minase, Helen Assefa Berhe, Edlawit Mebrahtu Jember, Elul Simeneh Abiy, Sebelwongel Esubalew Bitew and Bisrat Nigussie Alemayehu
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Ardovino M, Ardovino I, Castaldi MA, Monteverde A, Colacurci N, Cobellis L. Laparoscopic myomectomy of a subserous pedunculated fibroid at 14 weeks of pregnancy: a case report. J Med Case Rep. 2011; 5:2–6. | ||
| In article | View Article PubMed | ||
| [2] | Sparic R, Mirkovic L, Malvasi A, Tinelli A. Epidemiology of uterine myomas: A review. Int J Fertil Steril.2016;9:424-35. | ||
| In article | |||
| [3] | Cardozo ER, Clark AD, Banks NK, Henne MB, Stegmann BJ, Segars JH. Theestimated annual cost of uterine leiomyomata in the United States. Am J Obstet Gynecol.2012; 206:211. e1-211 | ||
| In article | View Article PubMed | ||
| [4] | Coronado GD, Marshall LM, Schwartz SM. Complications in pregnancy, labor, and delivery with uterine leiomyomas: a population-based study.Obstet Gynecol.2000;95:764-9. | ||
| In article | View Article PubMed | ||
| [5] | Neiger R, Sonek JD, Croom CS. Pregnancy related changes in the size of uterine leiomyomas.J Reprod Med.2006;51:671-4. | ||
| In article | |||
| [6] | Cruz MSDDL, Buchanan EM: Uterine fibroids: diagnosis and treatment. Am Fam Physician. 2017, 95:100-7. | ||
| In article | |||
| [7] | McWilliams MM, Chennathukuzhi VM: Recent advances in uterine fibroid etiology. Semin Reprod Med. 2017, 35:181-9. 10.1055/s-0037-1599090. | ||
| In article | View Article PubMed | ||
| [8] | Sparic R, Nejkovic L, Mutavdzic D, Malvasi A, Tinelli A. Conservative surgical treatment of fibroids. Acta Chir Iugosl.2014;61:11-66. | ||
| In article | View Article | ||
| [9] | Baloniak B, Jasinskil O, Prews K. Slomko Z. Morphologic pattern of uterine myomas enucleated at cesarean section. Clinical Pol. 2002;73(4):255. | ||
| In article | |||
| [10] | Kathpalia SK, Arora D, Vasudeva S, Singh S. Myomectomy at cesarean section: a safe option. Med J Armed Forces India. 2016;72: S161–S163. | ||
| In article | View Article PubMed | ||
| [11] | Kwawkume EY. Myomectomy during cesarean section. IntJGynObs. 2003;76:183-4. | ||
| In article | View Article PubMed | ||
| [12] | Cohellis L, Florio P, Stradella L, Lulia EP. Electro-cautery of myomas during cesarean section, two cases reports. EuJ Obs Gyn Rep Biol. 2002. | ||
| In article | View Article PubMed | ||
| [13] | Kwawukume EY. Caesarean myomectomy.Afr J Reprod Health.2002;6:38-43. | ||
| In article | View Article PubMed | ||
| [14] | Obstet Gynecol Clin North Am 2006 Mar;33(1): 153-69. | ||
| In article | |||
| [15] | Ardovino M, Ardovino I, Castaldi MA, Monteverde A, Colacurci N, Cobellis L. Laparoscopic myomectomy of a subserous pedunculated fbroid at 14 weeks of pregnancy: a case report. J Med Case Rep. 2011; 5:2–6. | ||
| In article | View Article PubMed | ||
| [16] | Leach K, Khatain L, Tocce K. First trimester myomectomy as an alternative to termination of pregnancy in a woman with a symptomatic uterine leiomyoma: a case report. J Med Case Rep. 2011; 5:2–5. | ||
| In article | View Article PubMed | ||
| [17] | Bhatla N, Dash BB, Kriplani A, Agarwal N. Myomectomy during pregnancy: a feasible option. J Obstet Gynaecol Res. 2009;35(1):173–175. | ||
| In article | View Article PubMed | ||
| [18] | Guler AE, Guler ZÇD, Kinci MF, Mungan MT. Myomectomy during cesarean section: why do we abstain from? J Obstet Gynecol India. 2020. | ||
| In article | View Article PubMed | ||
| [19] | Kwawukume E. Myomectomy during cesarean section. Int J Gynecol Obstet. 2002;76(2):183–4. | ||
| In article | View Article PubMed | ||
| [20] | Kaymak O, Ustunyurt E, Okyay RE, Kalyoncu S, Mollamahmutoglu L. Myomectomy during cesarean section. Int J Gynecol Obstet. 2005;89(2):90–3. | ||
| In article | View Article PubMed | ||
| [21] | Lopes T, Spirtos N, Naik R. Monaghan J. Uterine fibroids. In: Bonney’s Gynaecological Surgery. 11th ed. Chichester: Blackwell; 2010. | ||
| In article | View Article | ||
| [22] | Liu WM, Wang PH, Tang WL, Te WI, Tzeng CR. Uterine artery ligation for treatment of pregnant women with uterine leiomyomas who are undergoing cesarean section. Fertil Steril. 2006;86(2):423–8. | ||
| In article | View Article PubMed | ||



{kind=link}
{kind=link}
{kind=link}