Median Arcuate Ligament Syndrome (MALS) is due to compression of the celiac axis by a fibrous arc shaped band of tissue connecting the right and left diaphragmatic crus. It is characterized by postprandial abdominal pain, weight loss, and intermittent abdominal bruit. Due to lack of specificity in clinical presentation, MALS is typically a diagnosis of exclusion and is low on the differential diagnosis for chronic abdominal pain. Here, we present a case of MALS in a young female.
Median Arcuate Ligament Syndrome (MALS) is also known as Celiac Axis Syndrome, Harjola-Marable syndrome, or Dunbar syndrome. It is a rare disorder that is due to the compression of the celiac artery by the median arcuate ligament resulting in signs and symptoms of foregut ischemia 1. It affects approximately two per 100,000 patients 2. This condition is typically seen in women within the ages of 30 to 50 as well as patients with a slender body physique 3. There is an increasing prevalence of this disorder in the pediatric population with females being more affected than males, especially in pubertal and post pubertal adolescents 4. There are no classic physical exam findings associated with MALS, but an abdominal bruit can be seen in about 35% of symptomatic patients 5. Individuals affected with this condition tend to have the hook sign or J shape on imaging 6. The characteristic hook-like appearance in MALS is due to the narrowing of the proximal celiac axis and can help differentiate MALS from other etiologies of celiac artery stenosis. We present a female with Median Arcuate Ligament Syndrome (MALS). This article was previously presented as a meeting poster at the Ross University School of Medicine Research Day Symposium on January 28, 2022, and at the Student National Medical Association (SNMA) Annual Medical Educational Conference (AMEC) on April 15, 2022.
40-year-old Caucasian female with a history of hypothyroidism, pericarditis with pericardial effusion s/p healed pericardial window, and former alcohol use. She presented to the ER with complaints of nausea, vomiting, generalized weakness, and epigastric pain for one day. She admitted to having long term fatigue, abdominal discomfort, and 60 pounds unintentional weight loss in the last one year. She denied chest pain, dysuria, hematemesis, and melena. Physical exam was notable for bradycardia at 38 bpm and an unremarkable abdominal exam. EKG showed sinus bradycardia. Cardiac, liver, and pancreatic markers were unremarkable.
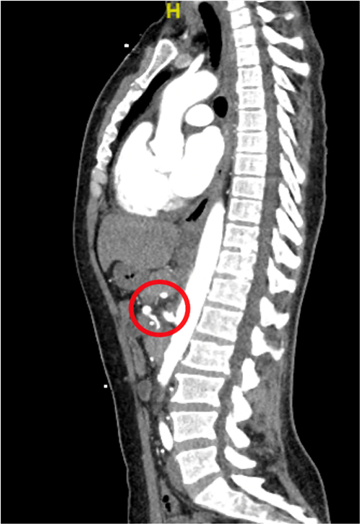
Patient’s CT Abdomen with contrast showed severe stenosis of the proximal celiac axis. Individuals with this condition have a characteristic hook-like appearance that is due to the narrowing of the proximal celiac axis and can help differentiate MALS from other etiologies of celiac artery stenosis. This can be seen in the patient's CT imaging in Figure 1 below.
Duplex ultrasound of mesenteric arteries revealed elevated peak systolic velocity of the celiac artery up to 386 cm/s and two times greater than the abdominal aorta peak systolic velocity, suggestive of median arcuate ligament compression syndrome. Patient’s bradycardia was attributed to increased vagal tone from nausea and vomiting which was controlled with Ondansetron as needed. Following improvement of symptoms, she was discharged, and followed up with a vascular surgeon for laparoscopic decompression of the celiac artery.
Based on the rarity of MALS, there is no current diagnostic protocol or treatment algorithm for this condition. Therapeutic interventions should be patient focused with consideration of the severity of clinical presentation. Symptom relief can be achieved with a variety of surgical interventions including median arcuate ligament release via open, laparoscopic, or robotic approach in addition to celiac ganglionectomy and or celiac artery reconstruction 7, 8.
A clinical study investigating postoperative symptomatic relief in MALS patients that underwent laparoscopic surgical intervention showed that 67% of the patient group had complete resolution of symptoms and 23% of the patient group had partial resolution of symptoms within 3 to 6 months post operative period 9.
A comparative study between the laparoscopic and robotic surgical intervention for MALS indicated that both interventions tend to have decreased postoperative complications with the laparoscopic approach having a shorter operative time. Within a mean follow up time of 22.2 months in the laparoscopic treatment patient group, 67% of this patient group had complete resolution of abdominal pain. Within a mean follow up time of 20 months in the robotic treatment patient group, 50% of this patient group had complete resolution of abdominal pain 10. Additionally, percutaneous transluminal angioplasty, primary reanastomosis, or celiac artery bypass grafting can be done in refractory cases of MALS. Immediate postoperative symptomatic relief is noted to be up to 85%. Prolonged symptomatic relief for years following surgery is about 53-80% with surgical decompression alone versus over 80% symptomatic relief with both decompression and vascular intervention 7. Future research work in this condition should be directed at the development of diagnostic guidelines to avoid delayed treatment as well as more evidence based therapeutic interventions.
MALS is a rare clinical condition that is usually seen in thin body habitus females within the ages of 30 to 50 years old. Our case represents an individual within the classically affected demographic presenting with constitutional and gastrointestinal symptoms. On imaging, our patient presents with the hook-like appearance that is indicative of this condition. Based on the rarity and nonspecific clinical presentation in this disorder, diagnostic and therapeutic algorithms are currently lacking. Future research work on this condition should be directed at the development of diagnostic guidelines and more evidence based therapeutic interventions.
| [1] | Goodall, R., Langridge, B., Onisa, S., Ellis, M., Lane, T., and Davies, A.H. “Median arcuate ligament syndrome,” Journal of vascular surgery, 71(6), 2170-2176. June 2020. | ||
| In article | View Article PubMed | ||
| [2] | Grotemeyer, D., Duran, M., and Iskandar, F. “Median arcuate ligament syndrome: vascular surgical therapy and follow-up of 18 patients,” Journal of Vascular Surgery, 51(4), 1063-1064. April 2010. | ||
| In article | View Article | ||
| [3] | Kim, E. N., Lamb, K., Relles, D., Moudgill, N., DiMuzio P.J., and Eisenberg J.A. “Median arcuate ligament syndrome—review of this rare disease,” JAMA Surgery, 151(5), 471-477. May 2016. | ||
| In article | View Article PubMed | ||
| [4] | Scholbach T. “Celiac artery compression syndrome in children, adolescents, and young adults: clinical and color duplex sonographic features in a series of 59 cases,” Journal of ultrasound in medicine: official journal of the American Institute of Ultrasound in Medicine, 25(3), 299-305. March 2006. | ||
| In article | View Article PubMed | ||
| [5] | Kuruvilla, A., Murtaza, G., Cheema, A., and Arshad, H. “Median Arcuate Ligament Syndrome: It Is Not Always Gastritis,” Journal of investigative medicine high impact case reports, 5(3), 1-3. September 2017. | ||
| In article | View Article PubMed | ||
| [6] | Cernigliaro, J., Chen F., and Bhatt, S. “The Hook sign of median arcuate ligament syndrome on ultrasound,” Abdominal Radiology, 46(5), 2251-2252. November 2020. | ||
| In article | View Article PubMed | ||
| [7] | Sapadin, A., and Misek, R. “Atypical presentation of median arcuate ligament syndrome in the emergency department,” Clinical Practice and Cases in Emergency Medicine, 3(4), 413-416. October 2019. | ||
| In article | View Article PubMed | ||
| [8] | Roddy, S.P. “Laparoscopic versus open celiac ganglionectomy in patients with median arcuate ligament syndrome,” Journal of vascular surgery, 52(5), 1419. November 2010. | ||
| In article | View Article | ||
| [9] | Kazmi, S., Safi, N., Berge S.T., Kamzi M., Sundhagen J.O., and Hisdal, J. “Laparoscopic Surgery for Median Arcuate Ligament Syndrome (MALS): A Prospective Cohort of 52 Patients,” Vascular health and risk management, 18(3), 139-151. March 2022. | ||
| In article | View Article PubMed | ||
| [10] | Do, M.V., Smith, T.A., Bazan, H.A., Sternbergh, W.C., Abbas, A.E., and Richardson, W.S. “Laparoscopic versus robot-assisted surgery for median arcuate ligament syndrome,” Surgical endoscopy, 27(11), 4060-4066. July 2013. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2022 Folake Ishola, Yaqub Nadeem Mohammed and Geetha Krishnamoorthy
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Goodall, R., Langridge, B., Onisa, S., Ellis, M., Lane, T., and Davies, A.H. “Median arcuate ligament syndrome,” Journal of vascular surgery, 71(6), 2170-2176. June 2020. | ||
| In article | View Article PubMed | ||
| [2] | Grotemeyer, D., Duran, M., and Iskandar, F. “Median arcuate ligament syndrome: vascular surgical therapy and follow-up of 18 patients,” Journal of Vascular Surgery, 51(4), 1063-1064. April 2010. | ||
| In article | View Article | ||
| [3] | Kim, E. N., Lamb, K., Relles, D., Moudgill, N., DiMuzio P.J., and Eisenberg J.A. “Median arcuate ligament syndrome—review of this rare disease,” JAMA Surgery, 151(5), 471-477. May 2016. | ||
| In article | View Article PubMed | ||
| [4] | Scholbach T. “Celiac artery compression syndrome in children, adolescents, and young adults: clinical and color duplex sonographic features in a series of 59 cases,” Journal of ultrasound in medicine: official journal of the American Institute of Ultrasound in Medicine, 25(3), 299-305. March 2006. | ||
| In article | View Article PubMed | ||
| [5] | Kuruvilla, A., Murtaza, G., Cheema, A., and Arshad, H. “Median Arcuate Ligament Syndrome: It Is Not Always Gastritis,” Journal of investigative medicine high impact case reports, 5(3), 1-3. September 2017. | ||
| In article | View Article PubMed | ||
| [6] | Cernigliaro, J., Chen F., and Bhatt, S. “The Hook sign of median arcuate ligament syndrome on ultrasound,” Abdominal Radiology, 46(5), 2251-2252. November 2020. | ||
| In article | View Article PubMed | ||
| [7] | Sapadin, A., and Misek, R. “Atypical presentation of median arcuate ligament syndrome in the emergency department,” Clinical Practice and Cases in Emergency Medicine, 3(4), 413-416. October 2019. | ||
| In article | View Article PubMed | ||
| [8] | Roddy, S.P. “Laparoscopic versus open celiac ganglionectomy in patients with median arcuate ligament syndrome,” Journal of vascular surgery, 52(5), 1419. November 2010. | ||
| In article | View Article | ||
| [9] | Kazmi, S., Safi, N., Berge S.T., Kamzi M., Sundhagen J.O., and Hisdal, J. “Laparoscopic Surgery for Median Arcuate Ligament Syndrome (MALS): A Prospective Cohort of 52 Patients,” Vascular health and risk management, 18(3), 139-151. March 2022. | ||
| In article | View Article PubMed | ||
| [10] | Do, M.V., Smith, T.A., Bazan, H.A., Sternbergh, W.C., Abbas, A.E., and Richardson, W.S. “Laparoscopic versus robot-assisted surgery for median arcuate ligament syndrome,” Surgical endoscopy, 27(11), 4060-4066. July 2013. | ||
| In article | View Article PubMed | ||



{kind=link}