Costal chondrosarcoma is characterized by a high locoregional invasion potential. Because more chondrosarcomas are resistant to chemotherapy and radiation therapy, the main treatment is based on surgery. Radiologic evaluation of patients and confirmatory biopsy of tissue plays a great role in determining localization, spread, invasion, and treatment options. Chondrosarcomas which arise from the axial skeleton have a poor prognosis. Costal chondrosarcomas in pediatric patients are not well discussed in the literature and due to its proximity of organs in the thoracic cavity, carries great risk for complications. Clinical presentation can be unpredictable. Low cost, accessibility, quick examination time makes X-rays a preferable inspection tool to detect the disease, but the important thing here is to examine each chest radiograph precisely, otherwise, the result may be misleading. Costal Chondrosarcoma in an 8-month-old female is a rare case and is covered in this case report.
An 8-month-old female was admitted to the clinic with a complaint of cough. The patient was examined by a pediatrician, and a slight weakening of the respiratory tract in the right lung was revealed on auscultation. No significant change in laboratory indicators was observed.
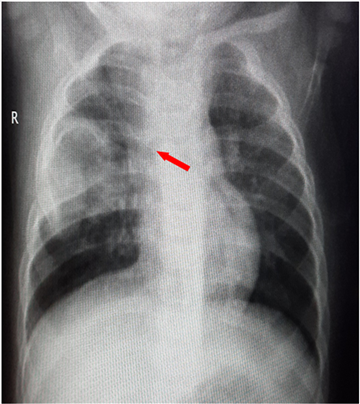
The patient was first examined by frontal-posterior-anterior and lateral chest radiography, then the examination was performed in an oblique lie.
Examination revealed no parenchymal changes in the lungs and no cardio-mediastinal pathology. Examination of the chest wall revealed a pathological shadow of a heterogeneous structure and inaccurate contours in the projection on the right upper and lateral hemithorax and posterior mediastinum, and deformity of the adjacent ribs was also noted. This process is assumed to be of nerve or bone origin.
The patient underwent a thoracic CT examination to clarify the diagnostic process. Examination revealed the expansile formation of 45x36x38 mm extension, with indistinct contours, in which the calcified components are visible. It caused an increase in the posterior part of the IV rib. After the contrast enhancement, the lesion was minimally contrasted. CT scan result was evaluated as Ewing sarcoma or right IV rib chondrosarcoma and the patient was referred to an oncologist (Figure 1 and Figure 2).

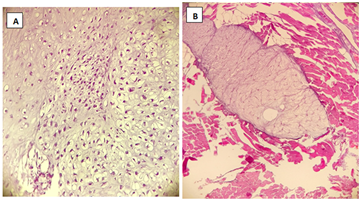
The right IV rib was resected with a derivative and pathos cytomorphological examination was performed. The bulge in the encapsulated smooth and rough structure of 4.3x3.3x3 cm was observed on the bone in the operating material corresponding to the 11.5 cm long rib fragment, Figure 3 (A, B). Pathos cytomorphological opinion: Chondrosarcoma (ICD-O:9220/3), Grade 2. Surgical margins were evaluated as tumor-negative.
After the operation, the patient was regularly monitored by the oncologist every 3 months. Appropriate clinical and laboratory evaluations were performed and no recurrent or metastatic changes were detected within 1 year.
Malignant primary bone tumors of the thoracic wall are rare. They account for 4.5 to 8% of all bone tumors. Most often, they are located in the ribs and are predominantly chondrosarcoma (CS), which alone accounts for 40% of all malignant rib tumors 1. Its diagnosis is suspected to be based on imaging studies, with a definitive diagnosis based on histology. CS is a malignant tumor with cartilaginous differentiation, with no bone or osteoid production, but it can contain foci of tumor-induced or endochondral ossification. It is characterized by a high potential for locoregional invasion and recurrence after treatment 1.
Grade 1 involvement includes especially flat bones, for example, axial skeleton, pelvis, scapula, and skull base. Due to the absence of mitosis, cellularity is moderate and no metastases are observed. Grade 1 chondrosarcomas 10-year survival rate variables between 83 to 95 percentage, in grade 2 chondrosarcoma more cellularity and mitosis can be observed. Although grade 1 has a more abundant cartilage matrix, in grade 2 less chondroid matrix observes and despite grade 1 having less potential for metastasis, in grade 2 this risk increases up to intermediate level (10-15 percentage) and 10 years survival decreases from 64 to 86 percentage 2, 3, 4.
Studies show that the clinical and biological character of a tumor depends on its location and grading 5. In grade 3 tumors are also characterized with high metastatic potential (nearly 32 to 70 percentage), abundant cellularity and easy observable mitosis, spindle cells, and worse prognosis with 10 years survival rate of 29 to 55 percentage 2, 3.
It is important to emphasize that chondrosarcomas with axial skeleton location have a poor outcome and need more aggressive management 6, 8.
Even though etiology is not well known for primary chondrosarcoma, studies show that some similarities among chondrocyte growth and differentiation in the growth plate in both malignant and nonmalignant tumors, cartilage tumors always constitute in the bones which arise from enchondral ossification 9.
In spite of the fact that osteochondroma and enchondroma are being benign cartilage tumors, they can play a role in secondary chondrosarcoma formation and can be counted as precursor lesions. Osteochondroma called osteocartilaginous exostosis is bony projections that arise from bone surfaces and as a continuation of bone which it arises from, it contains bone marrow. The inherited form of osteochondromas is called hereditary multiple exostoses and these patients have two or more osteochondromas in an axial and appendicular skeleton which becomes a serious condition, especially they are prone to fracture, pain, swelling in the affected area.
Studies show that there is a 5% risk of malignancy transformation with solitary or multiple osteochondromas 10, 11, 12, 13, 14.
According to some studies, the average time for malignancy transformation from initially diagnosed osteochondroma to chondrosarcoma was 9,8 years 15.
Any changes compared to the previous size, any new symptom associated with osteochondroma require further evaluation to exclude malignant transformation, especially in the pelvis, hips, and shoulder girdle, as they are more prone to malignant transformation 16, 17.
Another precursor of chondrosarcoma is enchondroma (also benign cartilage tumor but arise from the medulla of bones), which can manifest as Ollier disease (enchondromatosis- multiple enchondromas) and Maffucci syndrome (enchondromatosis along with soft tissue hemangiomas), which rather than carrying risk for malignant transformation also leads to bone deformities, limb - length changes. Having multiple enchondromas carries more risk (50%) rather than solitary lesion (1%) 15, 18, 19, 20, 21, 22, 23.
Despite usual chondrosarcomas being asymptomatic, initial complaints may be due to pain and local swelling. As in our patient came from cough symptoms is assumed due to pleural irritation and swelling due to the wide mass effect of the tumor. Studies show that 3 to 17 percent of patients had pathological fractures due to chondrosarcoma 24.
Due to its proximity to internal organs in the thoracic cavity, costal chondrosarcomas carry a great risk for injury. Depending on localization they carry a high risk for fracture and corresponding traumatic pneumothorax, pericardial injury, mass effect lead to compressive atelectasis.
Because of poor response to chemotherapy and radiotherapy, surgical management gives the only reliable cure for the management of chondrosarcomas.
Some studies demonstrate that extensive intralesional curettage and following local chemical therapies gives benefit for long-term surveillance 25, 26, 27, 28, 29, 30.
The success rate of surgical management highly depends on the grade, location, and tumor extent. For determining management approach radiology plays a great role in detecting some of the features of tumors mentioned above. Plain radiography due to its low cost, easy access, and quick examination time carries a great benefit for the initial evaluation of patients. In our case also considering patients’ age we conducted chest X-rays. Initial assumption can be made by X-ray due to location and radiographic appearance lesion gives to physician information about chondrosarcomas 31. X-ray, MRI and CT give additional advantageous information about tumor spread, invasion, extend, and size. For detection of matrix mineralization as well as for tumors localized in anatomically difficult areas CT is preferred. Chondrosarcomas show themselves as low attenuation on CT. In determining soft tissue and bone involvement MRI is preferred and tumors can be seen on T2-weighted images as high signal intensity.
MRI also helps to determine cartilaginous cap assessment, the limit of which is 2sm 32. Thick cap and ambiguous calcification and size more than 2sm suggest secondary chondrosarcomas. Periosteal reaction is not commonly seen but the cortex is often thick. Scant of mineralization of soft tissue mass suggest high-grade tumor, especially dedifferentiated types.
Despite the fact that Positron emission scanning with fluorodeoxyglucose plays an important role in determining most tumors and has high sensitivity, it plays a less significant role in the evaluation of chondrosarcomas. Although grade 2 and grade 3 have higher Standardized uptake values due to high glucose metabolism, PET inadequately differentiates benign cartilage tumors from malignant forms 33. It gives uncertain benefits for metastasis and relapses. For confirmatory diagnosis, biopsy plays an important role. But percutaneous small tissue sample biopsy lacks diagnostic, does not reflect the true characteristics of the lesion and is not recommended. Biopsy should be taken with the surgeon via a wide section and if malignancy is seen in the biopsy it must be determined due to definitive surgery and tissue for sampling needed to be taken from the most aggressively described area according to radiography 34.
Radiology here plays an important role, especially for guiding surgeons and determining the borders of tumors for wide local tissue resection, otherwise, the result may be misleading because of missing the needed tissues, especially in areas of low-grade chondrosarcomas seen.
Regarding metastasis, for chondrosarcoma, the lungs are more involved organs and followed by the liver. For grade 1 tumors due to the low potential of metastasis, lung scans are not necessary. Having the high metastatic potential to lungs especially in grade 2 and grade 3 tumors of chondrosarcoma, CT plays a superior role in compared to PET scans (due to inadequacy for determining metastases) examinations. Despite the fact that a Pet scan can give us information about the site of metastatic disease, but detecting especially small metastasis in the lung is inferior to a CT scan 33.
A reasonable differential includes enchondroma, giant cell tumor, and a bone cyst. Chondrosarcomas account for 27% of all primary malignant bone tumors, second only to osteosarcoma in adults 35. Those that occur as de novo are called primary. Those that arise from previously benign cartilaginous lesions (i.e. - enchondroma or the benign cartilage cap of an osteochondroma) are secondary. Concerning their osseous location, chondrosarcoma may be further designated as conventional/central (arising in the medullary cavity), peripheral, or juxtacortical (periosteal). Finally, histological classifications of primary chondrosarcoma include intramedullary, clear cell, juxtacortical, myxoid, mesenchymal, extraskeletal, and dedifferentiated 35.
The grading of chondrosarcoma is based on cellularity, nuclear size, degree of nuclear staining (hyperchromasia), and presence of mitotic figures 36. A diagnosis of a Grade 2 (as in our patient) or a Grade 3 chondrosarcoma can usually be based on cytological or histological features only. Differentiating an enchondroma from a well-differentiated/Grade 1 chondrosarcoma can be difficult. The criteria for diagnosis of chondrosarcoma in small bones include cortical or soft tissue destruction or the presence of mitotic figures.
Radiographically chondrosarcomas present as an expansile, mixed sclerotic, and centrally lucent lesion, with a narrow zone of transition, and possible thin sclerotic margin. The sclerotic portion represents the chondroid matrix mineralization 35. Flocculent calcifications described as “arcs-and-rings” are the defining radiographic feature of a chondroid lesion helping to differentiate them from tumors with an “amorphous and cloudlike” osseous matrix. The “arcs-and-rings” represent endochondral ossification at the edge of the cartilage lobules 35.
Most CT features of chondrosarcoma are a more sensitive extension of the radiographic findings. CT accurately defines the intraosseous portion of the tumor, better detects subtle tumor matrix and adequately delineates soft tissue extension 35. On CT, the non-mineralized portion of the tumor is hypodense to muscle because of the abundant water content of hyaline cartilage. The mineralized portion shows the characteristic chondroid “rings and arcs” appearance (70%) 35.
Clinical behavior, anatomical location, and radiologic findings must be taken into consideration in conjunction with the histological criteria to differentiate an enchondroma from low-grade chondrosarcoma. The presence of focal pain is often used to crudely distinguish chondrosarcoma, but it may be difficult to localize pain in the pediatric population. In a study based on initial clinical and imaging information that didn't directly involve any pathologists or radiologists and was restricted to orthopedic oncologists for diagnosis and grading of cartilaginous neoplasms, inter and intra-observer agreements were only fair to good 37. As cartilaginous tumors can be quite challenging to diagnose, these lesions should be discussed in a multidisciplinary meeting that includes a radiologist and a pathologist specializing in bone tumors.
1. Rib tumors are rare entities in the pediatric population. However, a significant number of rib lesions are malignant. Therefore, proper diagnosis and expeditious treatment are critical. The case presented one of the rarest cases of osteosarcoma of the rib in a child.
2. In the early stages of the disease, a weak noticeable symptom was recorded as a cough. That is why, chest bone structures should be carefully examined along with lungs in thoracic radiology, especially in the first phase of Chest X-ray (Chest Radiography) examination in children.
3. Early diagnosis and adequate treatment (surgical intervention) save the patient from metastatic and relapses.
4. The main point here is early diagnosis and treatment. Costal chondrosarcomas in pediatric patients are not well discussed in the literature and due to its proximity of organs in the thoracic cavity, carries great risk for complications.
CS-Chondrosarcoma
MRI- Magnetic resonance tomography
CT- computed tomography
AP-anterior-posterior
R- right
The authors declare no conflict of interest.
| [1] | D. Bacha, A. Ayadi-Kaddour, S. Fenniche, A. Marghli, T. Kilani, F. El Mezni, Costal chondrosarcoma. Report of five cases, Orthopaedics & Traumatology: Surgery & Research, Volume 95, Issue 2,2009,Pages 164-169. | ||
| In article | View Article PubMed | ||
| [2] | Angelini A, Guerra G, Mavrogenis AF, et al. Clinical outcome of central conventional chondrosarcoma. J Surg Oncol 2012; 106: 929. | ||
| In article | View Article PubMed | ||
| [3] | Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer 1977; 40: 818. | ||
| In article | View Article | ||
| [4] | BjÃrnsson J, McLeod RA, Unni KK, et al. Primary chondrosarcoma of long bones and limb girdles. Cancer 1998; 83: 2105. | ||
| In article | View Article | ||
| [5] | Soft tissue and bone tumors. In WHO Classification of Tumours, 5th ed, WHO Classification of Tumours Editorial Board (Ed), IARC Press, 2020. | ||
| In article | |||
| [6] | Bindiganavile S, Han I, Yun JY, Kim HS. Long-term Outcome of Chondrosarcoma: A Single Institutional Experience. Cancer Res Treat 2015; 47:897. | ||
| In article | View Article PubMed | ||
| [7] | Fromm J, Klein A, Baur-Melnyk A, et al. Survival and prognostic factors in conventional central chondrosarcoma. BMC Cancer 2018; 18: 849. | ||
| In article | View Article PubMed | ||
| [8] | van Praag Veroniek VM, Rueten-Budde AJ, Ho V, et al. Incidence, outcomes and prognostic factors during 25 years of treatment of chondrosarcomas. Surg Oncol 2018; 27: 402. | ||
| In article | View Article PubMed | ||
| [9] | Bovée JV, Hogendoorn PC, Wunder JS, Alman BA. Cartilage tumors and bone development: molecular pathology and possible therapeutic targets. Nat Rev Cancer 2010; 10: 481. | ||
| In article | View Article PubMed | ||
| [10] | Bovée JV. Multiple osteochondromas. Orphanet J Rare Dis 2008; 3: 3. | ||
| In article | View Article PubMed | ||
| [11] | Schmale GA, Conrad EU 3rd, Raskind WH. The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994; 76: 986. | ||
| In article | View Article PubMed | ||
| [12] | Wicklund CL, Pauli RM, Johnston D, Hecht JT. Natural history study of hereditary multiple exostoses. Am J Med Genet 1995; 55: 43. | ||
| In article | View Article PubMed | ||
| [13] | Peterson HA. Multiple hereditary osteochondromata. Clin Orthop Relat Res 1989; 222. | ||
| In article | View Article | ||
| [14] | Pedrini E, Jennes I, Tremosini M, et al. Genotype-phenotype correlation study in 529 patients with multiple hereditary exostoses: identification of “protective” and “risk” factors. J Bone Joint Surg Am 2011; 93: 2294. | ||
| In article | View Article PubMed | ||
| [15] | Altay M, Bayrakci K, Yildiz Y, et al. Secondary chondrosarcoma in cartilage bone tumors: report of 32 patients. J Orthop Sci 2007; 12:415. | ||
| In article | View Article PubMed | ||
| [16] | Ahmed AR, Tan TS, Unni KK, et al. Secondary chondrosarcoma in osteochondroma: report of 107 patients. Clin Orthop Relat Res 2003; 193. | ||
| In article | View Article PubMed | ||
| [17] | Pierz KA, Womer RB, Dormans JP. Pediatric bone tumors: osteosarcoma Ewing’s sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001; 21: 412. | ||
| In article | View Article PubMed | ||
| [18] | Silver C, Jüppner H. Ollier disease. Orphanet J Rare Dis 2006; 1: 37. | ||
| In article | View Article PubMed | ||
| [19] | Liu J, Hudkins PG, Swee RG, Unni KK. Bone sarcomas are associated with Ollier's disease. Cancer 1987; 59:1376. | ||
| In article | View Article | ||
| [20] | Schwartz HS, Zimmerman NB, Simon MA, et al. The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987; 69:269. | ||
| In article | View Article PubMed | ||
| [21] | Albregts AE, Rapini RP. Malignancy in Maffucci's syndrome. Dermatol Clin 1995; 13:73. | ||
| In article | View Article | ||
| [22] | Verdegaal SH, Bovée JV, Pansuriya TC, et al. Incidence, predictive factors, and prognosis of chondrosarcoma in patients with Ollier disease and Maffucci syndrome: an international multicenter study of 161 patients. Oncologist 2011; 16: 1771. | ||
| In article | View Article PubMed | ||
| [23] | Pannier S, Legeai-Mallet L. Hereditary multiple exostoses and enchondromatosis. Best Pract Res Clin Rheumatol 2008; 22: 45. | ||
| In article | View Article PubMed | ||
| [24] | Murphey MD, Walker EA, Wilson AJ, et al. From the archives of the AFIP: imaging of primary chondrosarcoma: radiologic-pathologic correlation. Radiographics 2003; 23: 1245. | ||
| In article | View Article PubMed | ||
| [25] | Leerapun T, Hugate RR, Inwards CY, et al. Surgical management of conventional grade 1 chondrosarcoma of long bones. Clin Orthop Relat Res 2007; 463: 166. | ||
| In article | View Article PubMed | ||
| [26] | van der Geest IC, de Valk MH, de Rooy JW, et al. Oncological and functional results of cryosurgical therapy of enchondromas and chondrosarcomas grade 1. J Surg Oncol 2008; 98: 421. | ||
| In article | View Article PubMed | ||
| [27] | Donati D, Colangeli S, Colangeli M, et al. Surgical treatment of grade I central chondrosarcoma. Clin Orthop Relat Res 2010; 468: 581. | ||
| In article | View Article PubMed | ||
| [28] | Bauer HC, Brosjà O, Kreicbergs A, Lindholm J. Low risk of recurrence of enchondroma and low-grade chondrosarcoma in extremities. 80 patients followed for 2-25 years. Acta Orthop Scand 1995; 66: 283. | ||
| In article | View Article PubMed | ||
| [29] | Aarons C, Potter BK, Adams SC, et al. Extended intralesional treatment versus resection of low-grade chondrosarcomas. Clin Orthop Relat Res 2009; 467: 2105. | ||
| In article | View Article PubMed | ||
| [30] | Streitb ürger A, Ahrens H, Balke M, et al. Grade I chondrosarcoma of bone: the Münster experience. J Cancer Res Clin Oncol 2009; 135:543. | ||
| In article | View Article PubMed | ||
| [31] | Soft tissue and bone tumors. In WHO Classification of Tumours, 5th ed, WHO Classification of Tumours Editorial Board (Ed), IARC Press, 2020. | ||
| In article | |||
| [32] | Bernard SA, Murphey MD, Flemming DJ, Kransdorf MJ. Improved differentiation of benign osteochondromas from secondary chondrosarcomas with standardized measurement of cartilage cap at CT and MR imaging. Radiology 2010; 255: 857. | ||
| In article | View Article PubMed | ||
| [33] | Lee FY, Yu J, Chang SS, et al. Diagnostic value and limitations of fluorine-18 fluorodeoxyglucose positron emission tomography for cartilaginous tumors of bone. J Bone Joint Surg Am 2004; 86-A: 2677. | ||
| In article | View Article PubMed | ||
| [34] | Kerr DA, Lopez HU, Deshpande V, et al. Molecular distinction of chondrosarcoma from chondroblastic osteosarcoma through IDH1/2 mutations. Am J Surg Pathol 2013; 37: 787. | ||
| In article | View Article PubMed | ||
| [35] | Mosier SM, Patel T, Strenge K, Mosier AD. Chondrosarcoma in childhood: the radiologic and clinical conundrum. J Radiol Case Rep. 2012; 6(12): 32-42. | ||
| In article | View Article PubMed | ||
| [36] | Puri A. Chondrosarcomas in children and adolescents. EFORT Open Rev. 2020; 5(2): 90-95. Published 2020 Feb 26. | ||
| In article | View Article PubMed | ||
| [37] | Zamora T, Urrutia J, Schweitzer D, Amenabar PP, Botello E. Do Orthopaedic Oncologists Agree on the Diagnosis and Treatment of Cartilage Tumors of the Appendicular Skeleton? Clin Orthop Relat Res. 2017 Sep; 475(9): 2176-2186. | ||
| In article | View Article PubMed | ||
Published with license by Science and Education Publishing, Copyright © 2022 Malakhat Jahangir Sultanova and Mehriban Musa Sariyeva
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | D. Bacha, A. Ayadi-Kaddour, S. Fenniche, A. Marghli, T. Kilani, F. El Mezni, Costal chondrosarcoma. Report of five cases, Orthopaedics & Traumatology: Surgery & Research, Volume 95, Issue 2,2009,Pages 164-169. | ||
| In article | View Article PubMed | ||
| [2] | Angelini A, Guerra G, Mavrogenis AF, et al. Clinical outcome of central conventional chondrosarcoma. J Surg Oncol 2012; 106: 929. | ||
| In article | View Article PubMed | ||
| [3] | Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer 1977; 40: 818. | ||
| In article | View Article | ||
| [4] | BjÃrnsson J, McLeod RA, Unni KK, et al. Primary chondrosarcoma of long bones and limb girdles. Cancer 1998; 83: 2105. | ||
| In article | View Article | ||
| [5] | Soft tissue and bone tumors. In WHO Classification of Tumours, 5th ed, WHO Classification of Tumours Editorial Board (Ed), IARC Press, 2020. | ||
| In article | |||
| [6] | Bindiganavile S, Han I, Yun JY, Kim HS. Long-term Outcome of Chondrosarcoma: A Single Institutional Experience. Cancer Res Treat 2015; 47:897. | ||
| In article | View Article PubMed | ||
| [7] | Fromm J, Klein A, Baur-Melnyk A, et al. Survival and prognostic factors in conventional central chondrosarcoma. BMC Cancer 2018; 18: 849. | ||
| In article | View Article PubMed | ||
| [8] | van Praag Veroniek VM, Rueten-Budde AJ, Ho V, et al. Incidence, outcomes and prognostic factors during 25 years of treatment of chondrosarcomas. Surg Oncol 2018; 27: 402. | ||
| In article | View Article PubMed | ||
| [9] | Bovée JV, Hogendoorn PC, Wunder JS, Alman BA. Cartilage tumors and bone development: molecular pathology and possible therapeutic targets. Nat Rev Cancer 2010; 10: 481. | ||
| In article | View Article PubMed | ||
| [10] | Bovée JV. Multiple osteochondromas. Orphanet J Rare Dis 2008; 3: 3. | ||
| In article | View Article PubMed | ||
| [11] | Schmale GA, Conrad EU 3rd, Raskind WH. The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994; 76: 986. | ||
| In article | View Article PubMed | ||
| [12] | Wicklund CL, Pauli RM, Johnston D, Hecht JT. Natural history study of hereditary multiple exostoses. Am J Med Genet 1995; 55: 43. | ||
| In article | View Article PubMed | ||
| [13] | Peterson HA. Multiple hereditary osteochondromata. Clin Orthop Relat Res 1989; 222. | ||
| In article | View Article | ||
| [14] | Pedrini E, Jennes I, Tremosini M, et al. Genotype-phenotype correlation study in 529 patients with multiple hereditary exostoses: identification of “protective” and “risk” factors. J Bone Joint Surg Am 2011; 93: 2294. | ||
| In article | View Article PubMed | ||
| [15] | Altay M, Bayrakci K, Yildiz Y, et al. Secondary chondrosarcoma in cartilage bone tumors: report of 32 patients. J Orthop Sci 2007; 12:415. | ||
| In article | View Article PubMed | ||
| [16] | Ahmed AR, Tan TS, Unni KK, et al. Secondary chondrosarcoma in osteochondroma: report of 107 patients. Clin Orthop Relat Res 2003; 193. | ||
| In article | View Article PubMed | ||
| [17] | Pierz KA, Womer RB, Dormans JP. Pediatric bone tumors: osteosarcoma Ewing’s sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001; 21: 412. | ||
| In article | View Article PubMed | ||
| [18] | Silver C, Jüppner H. Ollier disease. Orphanet J Rare Dis 2006; 1: 37. | ||
| In article | View Article PubMed | ||
| [19] | Liu J, Hudkins PG, Swee RG, Unni KK. Bone sarcomas are associated with Ollier's disease. Cancer 1987; 59:1376. | ||
| In article | View Article | ||
| [20] | Schwartz HS, Zimmerman NB, Simon MA, et al. The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987; 69:269. | ||
| In article | View Article PubMed | ||
| [21] | Albregts AE, Rapini RP. Malignancy in Maffucci's syndrome. Dermatol Clin 1995; 13:73. | ||
| In article | View Article | ||
| [22] | Verdegaal SH, Bovée JV, Pansuriya TC, et al. Incidence, predictive factors, and prognosis of chondrosarcoma in patients with Ollier disease and Maffucci syndrome: an international multicenter study of 161 patients. Oncologist 2011; 16: 1771. | ||
| In article | View Article PubMed | ||
| [23] | Pannier S, Legeai-Mallet L. Hereditary multiple exostoses and enchondromatosis. Best Pract Res Clin Rheumatol 2008; 22: 45. | ||
| In article | View Article PubMed | ||
| [24] | Murphey MD, Walker EA, Wilson AJ, et al. From the archives of the AFIP: imaging of primary chondrosarcoma: radiologic-pathologic correlation. Radiographics 2003; 23: 1245. | ||
| In article | View Article PubMed | ||
| [25] | Leerapun T, Hugate RR, Inwards CY, et al. Surgical management of conventional grade 1 chondrosarcoma of long bones. Clin Orthop Relat Res 2007; 463: 166. | ||
| In article | View Article PubMed | ||
| [26] | van der Geest IC, de Valk MH, de Rooy JW, et al. Oncological and functional results of cryosurgical therapy of enchondromas and chondrosarcomas grade 1. J Surg Oncol 2008; 98: 421. | ||
| In article | View Article PubMed | ||
| [27] | Donati D, Colangeli S, Colangeli M, et al. Surgical treatment of grade I central chondrosarcoma. Clin Orthop Relat Res 2010; 468: 581. | ||
| In article | View Article PubMed | ||
| [28] | Bauer HC, Brosjà O, Kreicbergs A, Lindholm J. Low risk of recurrence of enchondroma and low-grade chondrosarcoma in extremities. 80 patients followed for 2-25 years. Acta Orthop Scand 1995; 66: 283. | ||
| In article | View Article PubMed | ||
| [29] | Aarons C, Potter BK, Adams SC, et al. Extended intralesional treatment versus resection of low-grade chondrosarcomas. Clin Orthop Relat Res 2009; 467: 2105. | ||
| In article | View Article PubMed | ||
| [30] | Streitb ürger A, Ahrens H, Balke M, et al. Grade I chondrosarcoma of bone: the Münster experience. J Cancer Res Clin Oncol 2009; 135:543. | ||
| In article | View Article PubMed | ||
| [31] | Soft tissue and bone tumors. In WHO Classification of Tumours, 5th ed, WHO Classification of Tumours Editorial Board (Ed), IARC Press, 2020. | ||
| In article | |||
| [32] | Bernard SA, Murphey MD, Flemming DJ, Kransdorf MJ. Improved differentiation of benign osteochondromas from secondary chondrosarcomas with standardized measurement of cartilage cap at CT and MR imaging. Radiology 2010; 255: 857. | ||
| In article | View Article PubMed | ||
| [33] | Lee FY, Yu J, Chang SS, et al. Diagnostic value and limitations of fluorine-18 fluorodeoxyglucose positron emission tomography for cartilaginous tumors of bone. J Bone Joint Surg Am 2004; 86-A: 2677. | ||
| In article | View Article PubMed | ||
| [34] | Kerr DA, Lopez HU, Deshpande V, et al. Molecular distinction of chondrosarcoma from chondroblastic osteosarcoma through IDH1/2 mutations. Am J Surg Pathol 2013; 37: 787. | ||
| In article | View Article PubMed | ||
| [35] | Mosier SM, Patel T, Strenge K, Mosier AD. Chondrosarcoma in childhood: the radiologic and clinical conundrum. J Radiol Case Rep. 2012; 6(12): 32-42. | ||
| In article | View Article PubMed | ||
| [36] | Puri A. Chondrosarcomas in children and adolescents. EFORT Open Rev. 2020; 5(2): 90-95. Published 2020 Feb 26. | ||
| In article | View Article PubMed | ||
| [37] | Zamora T, Urrutia J, Schweitzer D, Amenabar PP, Botello E. Do Orthopaedic Oncologists Agree on the Diagnosis and Treatment of Cartilage Tumors of the Appendicular Skeleton? Clin Orthop Relat Res. 2017 Sep; 475(9): 2176-2186. | ||
| In article | View Article PubMed | ||



{kind=link}
{kind=link}
{kind=link}