 sciepub.com
sciepub.com
 Quick Submission
Quick Submission

Incidence of Antenatal Malaria Parasitaemia and the Effect on the Haemoglobin Profile of Pregnant Women in Enugu East Local Government Area, Enugu, Nigeria
Jenavine O. Mbah1, O. O. Njoku1, Agwu U. Nnachi2, , Ijem A. Nnachi1, Amaechi J. Nwinyimagu3
, Ijem A. Nnachi1, Amaechi J. Nwinyimagu3
1Department of Biological Sciences, Faculty of Science, Ebonyi State University, Abakaliki, Nigeria
2Department of Immunology, Faculty of Medicine, Nnamdi Azikiwe University, Nnewi Campus, Nigeria
3Department of Forestry, Ministry of Agriculture and Natural Resources, Ebonyi State, Abakaliki, Nigeria
Abstract
Maternal morbidity and mortality has been associated with anaemia in pregnancy and is the cause of low birth weight in infants and other complications. The contribution of malaria infection to maternal anaemia in pregnancy has been well-documented in most other countries. This study, therefore, investigated the incidence of antenatal malaria parasitaemia and haemoglobin profile of pregnant women in Enugu East Local Government Area, Enugu, Nigeria. Seven hundred (700) capillary blood samples were collected from women that were made up of 210 primiparae, 390 multiparae and 100 non-pregnant (that served as the control group), and tested for presence of malaria parasites and haemoglobin profile using microscopy and a portable β-haemoglobin photometer (HamoCue, Hemo Cue AB, Angelholm, Sweden) respectively. The result showed that majority of the malaria positive participants were anaemic with haemoglobin (HB) below 11g/dl. There were more positive cases among primigravidae (first pregnancy) and there were also downward gradation in the intensity of malaria from primiparae to control group. Prevalence of malaria parasitaemia was found to be 55.56% at Annunciation hospital and 60.06% at Park lane hospital which was higher than prevalence of 22.00% and 16.00%% among non pregnant women used as control. The results showed a significant difference (P<0.05) between the primigravidae, and multigravidae (more pregnancies). Women between the age ranges of 18 – 28 were most infected. The findings of this study have proven that primiparae have high susceptibility to malaria in endemic regions. Also, anaemia was associated with malaria in pregnancy. There is need to intensify effort in malaria prevention on pregnant women. Educational campaign is recommended at all levels to improve the awareness of malaria and preventive measures. Attack on malaria by provision of access to effective treatment and reduction of access with the vector is as well recommended.
Keywords: intensity, pregnancy, primigravidae, multigravidae, parasitaemia, malaria, anaemia
Copyright © 2015 Science and Education Publishing. All Rights Reserved.Cite this article:
- Jenavine O. Mbah, O. O. Njoku, Agwu U. Nnachi, Ijem A. Nnachi, Amaechi J. Nwinyimagu. Incidence of Antenatal Malaria Parasitaemia and the Effect on the Haemoglobin Profile of Pregnant Women in Enugu East Local Government Area, Enugu, Nigeria. American Journal of Epidemiology and Infectious Disease. Vol. 3, No. 5, 2015, pp 88-94. http://pubs.sciepub.com/ajeid/3/5/1
- Mbah, Jenavine O., et al. "Incidence of Antenatal Malaria Parasitaemia and the Effect on the Haemoglobin Profile of Pregnant Women in Enugu East Local Government Area, Enugu, Nigeria." American Journal of Epidemiology and Infectious Disease 3.5 (2015): 88-94.
- Mbah, J. O. , Njoku, O. O. , Nnachi, A. U. , Nnachi, I. A. , & Nwinyimagu, A. J. (2015). Incidence of Antenatal Malaria Parasitaemia and the Effect on the Haemoglobin Profile of Pregnant Women in Enugu East Local Government Area, Enugu, Nigeria. American Journal of Epidemiology and Infectious Disease, 3(5), 88-94.
- Mbah, Jenavine O., O. O. Njoku, Agwu U. Nnachi, Ijem A. Nnachi, and Amaechi J. Nwinyimagu. "Incidence of Antenatal Malaria Parasitaemia and the Effect on the Haemoglobin Profile of Pregnant Women in Enugu East Local Government Area, Enugu, Nigeria." American Journal of Epidemiology and Infectious Disease 3, no. 5 (2015): 88-94.
| Import into BibTeX | Import into EndNote | Import into RefMan | Import into RefWorks |
At a glance: Figures
1. Introduction
Infectious diseases have been a consistent burden and continue to pose threat to human health, longevity as well as the global economy [1]. Malaria is a mosquito-borne infectious disease of humans and other animals caused by parasitic protozoans of the genus Plasmodium [2]. This plasmodial infectious disease transmitted through the bite of an infected female anopheles mosquito [3], is one of the most devastating infectious diseases (second only to tuberculosis) in the tropical and subtropical developing countries of the world with more than one million deaths annually [4]. Malaria debilitates and kills more people than any other single infectious disease [5]. It is considered a disease of poverty and duly recognized as a public health problem with overwhelming medical, social and economic implications [6]. Malaria accounts for 40% public health expenditure, 30% - 50% of in-patient admission and up to 60% out-patient visits in endemic regions of the world [4, 7]. In Nigeria, it has contributed to a huge economic loss of about 12 billion US dollars annually from medical cost, loss of man-hours, school absenteeism and other indirect costs [8].
Pregnant women, children, and immunocompromised individuals have the highest mobidity and mortality, and Africa bears the heaviest burden due to malaria [4]. Malaria infection during pregnancy is of significant public health concern, as it presents substantial risks for the pregnant woman, her unborn baby and the newborn child [9]. Pregnancy is a period of drastic physiological change which places extreme stress on various systems of the body. The severity of malaria in pregnancy is thought to be due to impaired immunity and the accompanying anaemia resulting from the depletion of erythrocytes due to plasmodial invasion. Malaria morbidity and mortality have been associated with anaemia in pregnancy and it is the cause of low birth weight in infants [10]. Approximately 51% of pregnant women are anaemic before delivery [11]. Anaemia in pregnancy has a multifactorial aetiology [12] and has been found to be associated with a higher risk of prolonged labour, abnormal delivery and low birth weight [13]. The World Health Organization identifies anaemia in pregnancy as a haemoglobin (Hb) reading of < 11.0 g/dl. However, an Hb reading of < 10.0 g/dl is the level widely utilized at health centres throughout Africa. Additionally, it is the point at which a patient is likely to become symptomatic and at which therapeutic intervention becomes critical [14].
Globally, 125 million women are at risk [15] and sub-Saharan Africa, where over 90% of the world’s malaria-related deaths occur, 25 million pregnant women are currently at risk for malaria, accounting for 10,000 maternal [16] and 200,000 neonatal deaths per year [17, 18]. In such regions of high transmission and endemicity, sub-clinical malarial infection is common [19]. Foetal complications result from high placental plasmodial burden (in high-transmission regions) and maternal anaemia manifesting as still birth, intrauterine growth restriction, low-birth-weight neonates and neonatal and newborn death [4, 20].
The complication of pregnant woman with malaria infection varies depending on the intensity of the transmission of malaria in a particular locality and according to individual’s level of natural immunity [9]. Malaria in endemic areas (such as Nigeria) is difficult to define due to asymptomatic infection even among pregnant women. In medical practice, the diagnosis of malaria based on fever and parasitaemia alone can be misleading resulting in gross over-diagnosis or under-diagnosis as well as inappropriate prescription and use of anti-malarials [21]. The accumulation/build up of plasmodial parasites in the placenta makes them unavailable in the peripheral blood; the patients will not demonstrate obvious symptoms and would therefore see no need for malarial diagnosis and treatment. The results of this condition are the above mentioned complications and maternal death even in the face of potent anti-malarials and preventive measures that could circumvent them. To provide more information/data on the current situation of the complication of malaria and anaemia, this study investigated the antenatal malaria parasitaemia and haemoglobin profile of pregnant women in Enugu East Local Government Area, Enugu, Nigeria.
2. Materials and Methods
2.1. Study AreaThis study was carried out at Enugu State University of Science and Technology Teaching Hospital (Park-Lane), Enugu and Annunciation Specialist Hospital, Emene, both located in Enugu State, south-eastern Nigeria. Enugu State is bordered by Imo state and Abia state to the south, Benue state to the northeast, Ebonyi state to the east, Anambra state to the west, and Kogi state to the northwest. The temperature in Enugu city is at the average, warmer to hot in its warmer month (up to 80 degrees Fahrenheit) and gets cooler to mild (up to 60 degrees Fahrenheit). February is the hottest month in Enugu. It has a mean temperature of about 87.16’F (30.64’C) while November is the lowest temperature in the city reaching up to 60.54’F (15.86’C). The rainfall is lowest at about 0.16 cubic centimeters (0.0098 cu in). It gets to normal around February. July has the highest rainfall at about 35.7 cubic centimetres (2.18 cu in).
2.2. Study PopulationThe population of study was drawn from primigravid and multigravid women, attending antenatal clinic at ESUT teaching hospital (Park-Lane) Enugu and Annunciation specialist hospital Emene, Enugu. Non pregnant women that served as the control group were also included. Seven hundred (700) women that were made up of 210 primiparae, 390 multiparae and 100 non-pregnant that served as the control group was enlisted after a non-coercive informed consent.
2.3. Ethical ConsiderationAll authors hereby declare that all experiments have been examined and approved by the Ethics and Research Committee of the Enugu State University of Science and Technology Teaching Hospital (Park-Lane) in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Also, written informed consent was obtained from the participants (or their relatives). Samples, data and other information obtained from the patients were handled with utmost confidentiality and used for the purpose of the study only.
2.4. Data CollectionStructured questionnaires were administered to participants and used to obtain information such as sex, age, residence, level of education, occupation, number of pregnancies, if the expectant mother ever had malaria, when and how often, if she ever had anaemia, when, the patient’s view on malaria anaemia on expectant women. Interviewer guided structured questionnaires prepared by the investigator and administered to pregnant women after obtaining informed consent. Researcher also reviewed the antenatal cards for those who attended Antenatal clinic to make sure the information given by the respondents was correct. Information in the card included: gestation age at first pregnancy, gestation age at first ANC visit, gravidity, etc.
2.5. Laboratory Protocols2.5.1. Sample Collection and Processing
A total of 700 blood samples were collected from the participants by finger-pricking according to Cheesbrough [22] and tested for the presence of malaria parasites and ascertained the haemoglobin profile of each participant.
2.5.2. Malaria Determination
Thick and thin smears were prepared for all samples and stained with Giemsa stain for 10 minutes, washed in tap water, dried and examined under oil immersion for malaria parasites using light microscopy at 100 x magnifications. In thick blood smear, if 100 oil-immersion microscopic fields revealed no parasites, it is considered negative. Parasite densities were expressed per micro litre of blood. For each positive thick smear, the level of parasite was estimated by counting asexual stages against 200 leucocytes. Based on the number of parasites counted per high power field of the microscope using the plus sign system, the intensity of infection was estimated. A second microscopist, who was unaware of the results of the earlier microscopist, checked the entire thick smears for quality assessment. Additionally a 10% randomly selected negative slides was reread
2.5.3. Anaemia Determination
At the time of interview using a portable β-haemoglobin photometer (HamoCue, Hemo Cue AB, Angelholm, Sweden), the haemoglobin profile of the pregnant woman was determined. The remaining venous blood after malaria determination was used to estimate the Haemoglobin profile of each subject and the results were matched against the respective malaria infection status. Anaemia was defined as Hb<11g/dl and severe anaemia was defined as <7g/dl [23].
2.5.4. Statistical Analysis
Statistical Package for Social Sciences (SPSS) version 17.0 was used for data analysis
3. Results
Contribution of Socio-Demographic Characteristics and Stage of Pregnancy
The results showed that first trimester recorded the highest percentage of infection. Out of the 208 pregnant women at their first trimester, 107 (51.44%) tested positive of malaria while 101 (48.56%) tested negative of malaria. Second trimester has the next high percentage. Out of the 199 pregnant women at their second trimester, 90 (45.23%) are positive of malaria, while 109 (54.77%) were negative of malaria. The least infected were those at their third trimester and control group that recorded 39.90% infection for third trimester and 19.00% for control group (Table 1).
With respect to education, 9(1.29%) are illiterates, 22(3.14%) has basic education, 492(70.29%) has secondary education while 177(25.29%) has secondary education. From the result, It showed that illiterate mothers has the highest percentage of malaria infection with 55.56% positive and 44.44% negative, followed by mothers with basic education with 40.91% positive and 59.09% negative , secondary school certificate mothers has 43.29% positive and 56.71% negative. The least infected mothers are the tertiary education certificate mother that has 37.29% positive and 62.71% negative (Table 2).
Table 3 shows the employment status of the participants. With respect to occupation, 51(7.29%) were salaried women, 302(43.14%) were self employed women, while 347(49.57%) were unemployed. It showed that salaried women have the highest percentage of infection. Out of the 51 salaried women, 28(54.90%) tested positive for malaria while 23 (45.10%) tested negative, followed by unemployed mothers with 43.23% positive and 56.77% negative. The least infected is the self employed mother with 38.08% positive and 61.92% negative.
Intensity of Malaria in Pregnancy
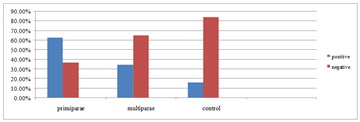
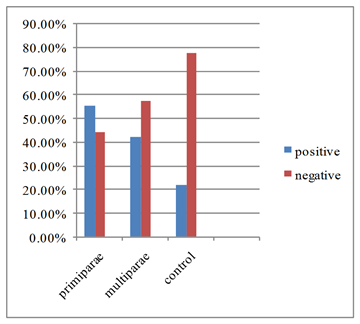
The results also showed that out of 376 women sampled, primiparae recorded 70 (63.06%) high positivity for malaria and 41 (36.94%) negative, followed by multiparae with 75 (34.88%) positive and 140 (65.12%) negative. The least infected was the control group with 8 (16.00%) positive and 42 (84.00%) negative (Figure 1). Study on the malaria parasitaemia by parity group at Annunciation hospital Enugu showed that out of 324 women sampled, primiparea recorded 55 (55.56%) high positivity for malaria and 44(44.44%) negative, followed by multiparae with 74(42.29%) positive and 101 (57.71%) negative. The least infected is the control group with 11(22.00%) positive and 39(78.00%) negative (Figure 2).
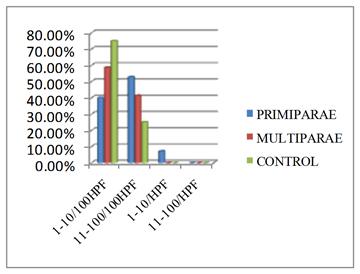
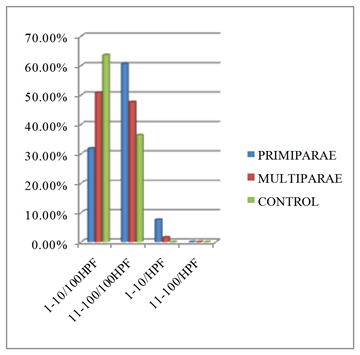
Figure 3 shows the intensity of malaria infection by parity group at Park-lane hospital Enugu. Intensity was highest among the primiparae with 52.86%, followed by multiparae with 41.33%. The least in intensity is the control group with 25.00%. There is a gradation of intensity from primiparae to control group. Figure 4 also shows the intensity of malaria infection by parity group at Annunciation hospital Emene Enugu. Intensity was highest among the primiparae with 60.61%, followed by multiparae with 47.62%. The least in intensity is the control group with 36.36%.

















 Download as
Download as
 Download as
Download as
 Download as
Download as
 Download as
Download as
Malaria and Haemoglobin Level in Pregnant Women
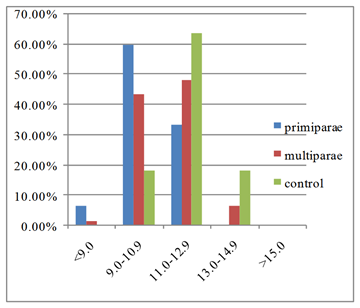
Figure 5 compares between haemoglobin profile of malaria positive primiparae, multiparae, and control women at annunciation hospital Emene Enugu. It showed that hemoglobin level of the infected women is dependent on malaria infection status and also the parity of pregnancy. More than half of malaria positive primiparae women have haemoglobin levels below the World Health Organisation (WHO) benchmark for pregnant women (11g/dl). Positive primiparae women recorded highest percentage of haemoglobin below normal, according to WHO standard. At <9.0, primaparae recorded 6.67%, at 9.0-10.9, it recorded 60.00%, making a total of 66.67%. At <9.0, multiparae records 1.61% and 43.55% at 9.0-10.9. Control group has the least percentage of below normal haemoglobin with 0% at <9.0 and 18.18% at 9.0-10.9.
 Download as
Download as
 Download as
Download as
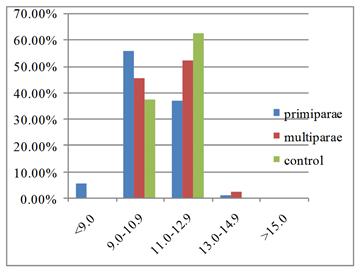
Figure 6 compares between haemoglobin profile of positive primiparae, multiparae, and control women at Park-Lane hospital Emene Enugu. Positive primiparae women recorded highest percentage of haemoglobin below normal, according to WHO standard. At <9.0, primaparae recorded 5.71%, at 9.0-10.9, it recorded 55.71%, making a total of 61.42%. At <9.0, multiparae records 0.0% and 45.33% at 9.0-10.9. Control group has the least percentage of below normal haemoglobin with 0% at <9.0 and 37.50% at 9.0-10.9.
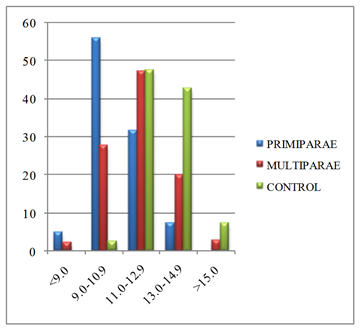
Figure 7 shows the comparison between haemoglobin profile of negative primiparae, multiparae, and control women at Park-Lane hospital Enugu. Even among the malaria negative women, primiparae women records high percentage of haemoglobin below normal, according to WHO standard. At <9.0, primaparae recorded 4.88%, at 9.0-10.9, it recorded 56.10%, At<9.0, multiparae records 2.14% and 27.86% at 9.0-10.9. Control group has the least percentage of below normal haemoglobin with 0% at <9.0 and 2.38% at 9.0-10.9.
 Download as
Download as
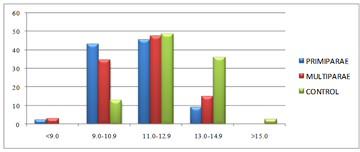
Figure 8 also shows the comparison between haemoglobin profile of negative primiparae, multiparae, and control women at Annunciation hospital Emene Enugu. Still among the malaria negative women, primiparae women records high percentage of haemoglobin below normal, according to WHO standard. At <9.0, primaparae recorded 2.27%, at 9.0-10.9, it recorded 43.18%, At<9.0, multiparae records 2.97% and 34.65% at 9.0-10.9. Control group has the least percentage of below normal haemoglobin with 0% at <9.0 and 12.82% at 9.0-10.9.
 Download as
Download as
4. Discussion
Maternal morbidity and mortality has been associated with anaemia in pregnancy and is the cause of low birth-weight infants [10]. Malaria infection during pregnancy can have adverse effect on both the foetus and the mother, to include foetal loss, maternal anaemia, premature delivery, delivery of low birth weight infants, intrauterine growth retardation and delivery of low birth weight infants [20]. The findings in this research have proven that primiparae have high susceptibility of malaria in endemic regions. This was found true, as prevalence of malaria parasitaemia was found to be 55.56% at Annunciation hospital and 60.06% at Park lane hospital which was higher than prevalence of 22.00% and 16.00%% among non pregnant women used as control. This prevalence is similar to 72% found by Adefioye et al. [24] in a study among pregnant women in Osogbo. It is also worth mentioning that Nwagha et al. [25] found a comparable prevalence of 60%. However, Amadi et al. [26].In a research on association of malaria and anaemia infection, anaemia prevalence was found to be 82%. In studies conducted by Brabin [27], it was found out that infection is more on the primigravidae than on the multigravidae. Prevalence was highest among the primigravidae and malaria positivity decreases as parity increased.
The recovery at latter pregnancy shows that the woman’s immune system are adjusting or have taken action against malaria infection, regaining immunity to anaemia and malaria, though there is no good evidence on whether natural immune depression is a serious illness in pregnancy, with placenta boost parasite increase but determines clinical result. There is significantly higher free and total serum cortisol consecration in pregnant women with malaria in Tanzania than controls without malaria whether it is multiparouse or nulliparouse. High plasma corticosteroid levels may have an immunosuppressive effect on cell mediated immune responses. It is clear evidence that cell-mediated immune responses to malaria antigens are more markedly suppressed in first than in subsequent pregnancies. McGregor [28] identified that as inhibition of type 1 cytokine responses (interferon, interleukins 2 and 12 and TNF) are factors responsible for susceptibility of primigravidae to malaria. Immunity has been altered at pregnancy hence, 70%-80% pregnant women at malaria endemic areas are susceptible to anaemia. Idowu et al. [29] observed higher prevalence of anaemia in pregnanacy (76.5%) in Abeokuta because women attending traditional birth home (TBH) were recruited into his study. Most of the women were taking herbal remedies made from roots, tree, and leaves of plants. To prevent anaemia, the supplements from iron are a necessary tool especially during increased physiological burden of pregnancy McGregor [28]. Same was lacking in among that visit traditional birth homes (TBH), this might be the cause higher prevalence recorded in that study.
The highest number of positive result was recorded with pregnant women that are at the age bracket of 15 to 35 years, while pregnant women at the age group of 36 to 45 years have the lowest result. This report supports Lander et al. [30] who said that prevalence is high at lower age and low as the women advance in age due to immunity acquired. As stated by other studies, the cause of anaemia has many factors with risk factors including hook worm infestation, lack of iron intake and malaria parasitaemia [31, 32] .
Though none of the contributing factors as stated by other studies [31, 32] was solely responsible for the observed anaemia in the respondents in the present study, malaria parasitaemia, as earlier mentioned have the ability to cause anaemia, the malaria parasite have the ability to cause haemolytic anaemia due to the destruction of the red blood cells by haemolysis. Although majority of the respondents knew that malaria was caused by mosquitoes, most of them used no preventive method against malaria infection hence a high incidence of parasitaemia.
There is need to intensify effort in malaria prevention on pregnant women. Educational campaign is recommended at all levels to improve the awareness of malaria and preventive measures. Attack on malaria by provision of access to effective treatment and reduction of access with the vector is hereby recommended. Use of insecticide treated net and monitoring will surely reduce the burden of parasitaemia. There should also be affordable and availability of these measures in recourse constrained settings. Other researches should be carried out to obtain effective planning and implementation of control programmes.
References
| [1] | Modebe AA, Nnachi AA, Ukaegbu AA, Tata N, Agha MV, Udu-Ibiam OE, Nnachi IA. Dual Infections of Enteric Salmonella species with Schistosoma mansoni among patients from two hospitals in Jos, Nigeria. Journal of Applied and Environmental Microbiology. 2014; 2(4): 198-202. | ||
 In article In article | |||
| [2] | Ukaegbu CO, Nnachi AU, Mawak JD, Igwe CC. Incidence Of Concurrent Malaria And Typhoid Fever Infections In Febrile Patients In Jos, Plateau State Nigeria. International Journal of Scientific and Technology Research. 2014; 3(4): 157-161. | ||
| In article | |||
| [3] | Monif GRG, Baker DA. Infectious Diseases in Obstetrics and Gynecology, 5th Edition. New York: Parthenon, 2004. 736 pp. | ||
| In article | |||
| [4] | Schantz-Dunn J, Nour NM. Malaria and Pregnancy: A Global Health Perspective. Review in Obstetrics Gynecology. 2009; 2(3): 186-192. | ||
| In article | PubMed | ||
| [5] | Sherman IW. A brief history of malaria and discovery of the parasite lifecycle. In malaria parasite biology, pathogenesis and protection. ASM press, Washington DC; 1998. | ||
| In article | |||
| [6] | Isah AY, Amanabo MA, Ekele BA. Prevalence of malaria parasitaemia amongst asymptomatic pregnant women attending a Nigerian hospital. 2011; 10(2): 171-174. | ||
| In article | |||
| [7] | Oshikoya KA. Antimalarial prescriptions for children presenting with uncomplicated malaria to a Teaching Hospital in Nigeria after the change of national guidelines for malaria treatment. World Journal of Medical Sciences. 2007; 2(1): 49-53. | ||
| In article | |||
| [8] | National Malaria Control Programme [NMCP] /Roll Back Malaria [RBM]. NMCP/RBM Business Plan (2009-2010), Nigeria; 2009. | ||
| In article | |||
| [9] | World Health Organization. Malaria in pregnant women. World Health Organization, Geneva. 2013. Available at: http://www.who.int/malaria/areas/high_risk_groups/pregnancy/en/. | ||
| In article | |||
| [10] | Achidi EA, Kuoh AJ, Achimbom BM, Motaze SC. Malaria infection in pregnancy and its effects on hemoglobin levels in women from a malaria endemic area of Fako Division, South West Province Cameroon. J Obstet Gynaecol Vol. 2005; 25:235-240. | ||
| In article | View Article PubMed | ||
| [11] | Bergmann R, Gravens-Muller L, Hertwig K, Hinkel J, Andres B, Bergmann K. Iron deficiency is prevalent in a sample of pregnant women at delivery in Germany. Eur J Obstet Gynecol Reprod Biol. 2002; 102(2):155-160. | ||
| In article | View Article | ||
| [12] | Thomson J. Anaemia in pregnant women in eastern caprivi,Namibia. S. Africa Med J. 1997; 87(11); 1544-1547. | ||
| In article | PubMed | ||
| [13] | Malhotra M, Sharma J, Batra S, Sharma S, Murthy N, Arora R. Maternal and perinatal outcome in varying grades of anaemia. Int J Gynaecol Obstet. 2002; 79(2):93-100. | ||
| In article | View Article | ||
| [14] | World Health Organisation. A Strategic Framework for Malaria Prevention and Control During: Pregnancy in the African Region, Brazzaville: WHO Regional Office for Africa; 2004. Available at: http://www.who.int/malaria/publications/atoz/afr_mal_04_01/en/index.html. | ||
| In article | |||
| [15] | Conroy AL, McDonald CR, Kain KC. Malaria in pregnancy: diagnosing infection and identifying fetal risk. Expert Rev Anti Infection Therapy. 2012; 10(11):1331-42. | ||
| In article | View Article PubMed | ||
| [16] | World Health Organization Web site, authors. Global Malaria Programme: pregnant women and infants. 2009. http://apps.who.int/malaria/pregnantwomenandinfants.html. | ||
| In article | |||
| [17] | Ismail MR, Ordi J, Menendez C, Ventura PJ, Aponte JJ, Kahigwa E, Hirt R, Cardesa A, Alonso PL. Placental pathology in malaria: a histological, immunohistochemical, and quantitative study. Hum Pathol. 2000;31:85-93. | ||
| In article | View Article | ||
| [18] | Matangila JR, Lufuluabo J, Ibalanky AL, da Luz RAI, Lutumba P, Van Geertruyden J-P. Asymptomatic Plasmodium falciparum infection is associated with anaemia in pregnancy and can be more cost-effectively detected by rapid diagnostic test than by microscopy in Kinshasa, Democratic Republic of the Congo. Malar J. 2014; 13: 132. | ||
| In article | View Article PubMed | ||
| [19] | Takem EN, D'Alessandro U. Malaria in pregnancy. Mediterr J Hematol Infect Dis. 2013;5(1):e2013010. | ||
| In article | View Article PubMed | ||
| [20] | Brabin BJ. An analysis of malaria in pregnancy in Africa. Bulletin of the World Health Organization. 1983; 61: 1005-1016. | ||
| In article | PubMed | ||
| [21] | Dicko A, Mantel C, Kouriba B, Sagara I, Thera MA, Doumbia S et al. Season, fever prevalence and pyrogenic threshold for malaria disease definition in an endemic area of Mali. Tropical Medicine and International Health, 2005; 10(6): 550-556. | ||
| In article | View Article PubMed | ||
| [22] | Cheesbrough M. District Laboratory Practice in Tropical Countries. Part 1. Second edition. Cambridge University Press, New York, USA; 2006. | ||
| In article | View Article PubMed | ||
| [23] | World Health Organisation. Prevention and Management of Severe Anaemia in Pregnancy:Report of a Technical Working Group. Geneva, Switzerland: WHO/FNE/MSM/93.5; 1993. | ||
| In article | |||
| [24] | Adefionye OA, Adeyeba O, Hassan WO, Oyeniran OA. Prevalence of malaria parasite infection among pregnant women in Osogbo, southwest Nigeria. International Journal of Natural and Applied Science. 2007; 2(2): 61-64, 3. | ||
| In article | |||
| [25] | Nwagha UI, Ugwu VO, Nwagha TU, Anyaehie USB. Asymptomatic Plasmodium parasitaemia in pregnant Nigerian women: almost a decade after Roll Back Malaria. Trans. Roy. Soc. Trop. Med. Hyg. 2009; 103:16-20. | ||
| In article | View Article PubMed | ||
| [26] | Amadi AN, Onwere S, Kamanu CI, Njoku OO, Aluka C. Study on the association between maternal malaria infection and anaemia. J Med Invest Pract (JOMIP). 2000; 1:23-25. | ||
| In article | |||
| [27] | Brabin BJ. The risks and severity of malaria in pregnant women. In: Applied field in malaria reports, no.1.Geneva, Switzerland World Health Organization (TDR/FIELDMAL/1); 1991. | ||
| In article | PubMed | ||
| [28] | McGregor IA. Thoughts on malaria in pregnancy Parasitologia. 1987; 29:153-163. | ||
| In article | |||
| [29] | Idowu OA, Mafiana CF, Dapo S. Anaemia in pregnancy: a survey of pregnant women in Abeokuta, Nigeria. Afr Health Sci Dec. 2005; 5(4):295-299. | ||
| In article | PubMed | ||
| [30] | Lander J, Leroy V, Simonon A, Karita E, Bogaerats J, Clercq AD, Van de Perre P, Dabis F. HIV infection, malaria and pregnancy: a prospective cohort study in Kigali, Rwanda. American Journal of tropical Medicine and Hygiene. 2002; 56-60. | ||
| In article | |||
| [31] | Aikawa M. Human Cerebral Malaria. Am J Trop Med Hyg. 1988; 39:341-352. | ||
| In article | |||
| [32] | Brooker S, Clark S, Snow RW, Bundy DAP. Malaria in African School Children-option for control. Transactions of Royal Society of Tropical Medicine and Hygiene. 2008; 102:304-305. | ||
| In article | View Article PubMed | ||
 CiteULike
CiteULike Delicious
Delicious



){kind=link}
{kind=link}
){kind=link}
{kind=link}
){kind=link}
{kind=link}
){kind=link}
{kind=link}
){kind=link}
{kind=link}
){kind=link}
{kind=link}
){kind=link}
{kind=link}
){kind=link}
{kind=link}