 sciepub.com
sciepub.com
 Quick Submission
Quick Submission

Assessing the Link between Colonoscopy Preparation Quality and Diabetes Mellitus
Deepthi C. Lankalapalli1, , Martin Kim1, Pranay Srivastava1, Stanley Abraham2, Miral Subhani1, Lu Fan1, Prakash Viswanathan1, Kaleem Rizvon1, Paul Mustacchia1
, Martin Kim1, Pranay Srivastava1, Stanley Abraham2, Miral Subhani1, Lu Fan1, Prakash Viswanathan1, Kaleem Rizvon1, Paul Mustacchia1
1Department of Internal Medicine, Nassau University Medical Center, East Meadow, USA
2New York Institute of Technology College of Osteopathic Medicine, Glen Head, USA
Abstract
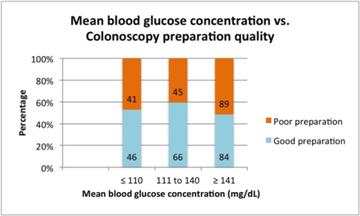
Diabetes mellitus, advanced age and male gender are known risk factors for poor bowel preparation for colonoscopy. There is limited literature about the relationship between levels of glycemic control and bowel preparation quality. We studied the association of diabetes-related and demographic variables with quality of bowel preparation for colonoscopy. Retrospective data was obtained for 380 consecutive patients who had HbA1c measured and had colonoscopies within 3 months of this measurement. The outcome variable was colonoscopy preparation quality (good versus poor). Predictors included HbA1c, mean blood glucose concentration, age, sex, and body mass index. The data obtained was further analyzed statistically. The sample was approximately equally distributed between those with good (53.4%) and poor (46.6%) quality colonoscopy preparation. When analyzed based on HbA1c, poor preparations were seen in 46% of the patients with HbA1c ≤ 6.9%, 43% of those with HbA1c between 7% and 9%, and 51% of the patients with HbA1c ≥ 9.1%. Poor preparations were also seen in 47% of the patients with mean blood glucose concentration ≤ 110mg/dL, 40% of those with mean blood glucose concentration between 111mg/dL and140mg/dL, and 51% of the patients with mean blood glucose concentration ≥ 141mg/dL. Gender was the only variable that statistically significantly differed between the groups where males had a greater percentage of poor quality colonoscopy preparation than females (61.6% vs. 38.4%). Patients who had colonoscopies as outpatients were more likely to have poor preparations than those who were inpatients at the time (55% vs. 40%). Ultimately, there was no association between levels of glycemic control, characterized by HbA1c and mean blood glucose concentration, and colonoscopy preparation quality.
Keywords: bowel preparation, colonoscopy, HbA1c, mean blood glucose concentrations, diabetes mellitus
Copyright © 2017 Science and Education Publishing. All Rights Reserved.Cite this article:
- Deepthi C. Lankalapalli, Martin Kim, Pranay Srivastava, Stanley Abraham, Miral Subhani, Lu Fan, Prakash Viswanathan, Kaleem Rizvon, Paul Mustacchia. Assessing the Link between Colonoscopy Preparation Quality and Diabetes Mellitus. American Journal of Clinical Medicine Research. Vol. 5, No. 2, 2017, pp 22-25. http://pubs.sciepub.com/ajcmr/5/2/3
- Lankalapalli, Deepthi C., et al. "Assessing the Link between Colonoscopy Preparation Quality and Diabetes Mellitus." American Journal of Clinical Medicine Research 5.2 (2017): 22-25.
- Lankalapalli, D. C. , Kim, M. , Srivastava, P. , Abraham, S. , Subhani, M. , Fan, L. , Viswanathan, P. , Rizvon, K. , & Mustacchia, P. (2017). Assessing the Link between Colonoscopy Preparation Quality and Diabetes Mellitus. American Journal of Clinical Medicine Research, 5(2), 22-25.
- Lankalapalli, Deepthi C., Martin Kim, Pranay Srivastava, Stanley Abraham, Miral Subhani, Lu Fan, Prakash Viswanathan, Kaleem Rizvon, and Paul Mustacchia. "Assessing the Link between Colonoscopy Preparation Quality and Diabetes Mellitus." American Journal of Clinical Medicine Research 5, no. 2 (2017): 22-25.
| Import into BibTeX | Import into EndNote | Import into RefMan | Import into RefWorks |
At a glance: Figures
1. Introduction
Colonoscopy remains to be the most frequently used screening tool till today and an increasing number of patients are going through screening than ever before. [1] However, inadequate bowel preparation is seen in 1 out of 5 colonoscopies. [2] Poor preparations warranting for repeat procedures remain to be a burden on patients and doctors due to increased costs and time spent to decrease the rate of missed lesions. [2, 3] Various studies have shown an association between advanced age, male gender, obesity, and the presence of comorbidities such as diabetes mellitus. It is likely that gastroparesis, diabetic colonic motor dysfunction, or diabetic autonomic neuropathy in general may be leading to an increased incidence of poor preparations in the diabetic population. Though studies have shown that diabetic patients have a significantly poorer response to a 6-L Golytely preparation than do non-diabetic patients, [4] an association between different levels of glycemic control with a much larger sample size has not been studied well.
In this retrospective study, we aim to find an association between increasing HbA1c and mean blood glucose concentration (MBGC) levels along with variables such as age, gender, body mass index (BMI) and poor bowel preparation quality. The goal of this study is to possibly improve bowel preparations by tailoring regimens that are more effective for diabetics if there is an association between glycemic control and poor preparations.
2. Materials and Methods
Retrospective data was obtained from 2011 to 2015 for 380 patients from the Electronic Medical Records (EMR) at Nassau University Medical Center in Long Island, New York for consecutive patients who had HbA1c measured and had colonoscopies within 3 months of this measurement. The Institutional Review Board approved the study.
The primary outcome variables in the study were colonoscopy preparation quality, HbA1c levels and mean blood glucose concentration levels. Colonoscopy preparation quality (good versus poor) was graded according to the Aronchick bowel preparation scale. Bowel preparation was done with ingestion of 1 gallon of NuLytely bowel preparation polyethylene glycol solution along with Dulcolax the day prior to the procedure. Bowel preparations were considered good if they received a score of 1 or 2 and poor if they received a score of 3,4 or 5 based on the Aronchick scale. HbA1c levels and MBGC levels were obtained from the EMR as well.
The results were then further stratified and adjusted by age, gender, and body mass index for each patient that were also obtained from the EMR. HbA1c, MBGC, age, and BMI were analyzed with the Pearson chi square test to calculate the categorical variables and logistic regression analysis was used to calculate odds ratio. These variables were analyzed with values categorized as: HbA1c levels ≤ 6.9%, between 7% and 9%, or ≥ 9.1%, MBGC levels ≤ 110mg/dL, between 111mg/dL and140mg/dL, or ≥ 141mg/dL, above or below the age of 60 years, and BMI above or below 25 kg/m2. Data was also stratified based on the patient being an inpatient or outpatient at the time of the procedure. Analysis of variance (ANOVA) or the Mann Whitney test was used for skewed data to analyze the continuous variables. P value ≤ 0.05 was considered significant. Statistical Package for the Social Sciences and Python software were used to analyze the data.
3. Results
The overall sample was approximately equally distributed between those with good (53.4%, n=203) and poor (46.6%, n=177) quality colonoscopy preparation. There were almost equal number of subjects who had good and poor preparations in those with HbA1c ≤ 6.9% and HbA1c ≥ 9.1%. Poor preparations were found in 42.8% of patients with HbA1c between 7% and 9% (Figure 1). In addition, the number of good and poor preparations were almost equally split in those with MBGC ≤ 110mg/dL and ≥ 141mg/dL. Poor preparations were seen in 40.5% of subjects with MBGC between 111mg/dL and140mg/dL (Figure 2). Overall, HbA1c and mean blood glucose concentration did not statistically differ between the colonoscopy preparation groups as shown in Figure 1 and Figure 2.

 Download as
Download as

 Download as
Download as
Only gender statistically significantly differed (p=0.02) between the groups with males having a greater percentage of poor quality colonoscopy preparations than females (61.6% vs. 38.4%) (Table 1). Age and BMI did not statistically differ between the colonoscopy preparation groups (Table 1). Although not statistically significant, patients who had colonoscopies as out-patients were more likely to have poor preparations than those who were in-patient at the time (55% vs. 44%) of the procedure (Table 2). Similar results were seen in the diabetic population as well, in which out-patients once again had poorer preparations than in-patients (55% vs. 40%) (Table 3).
Table 1. Colonoscopy preparation quality stratified based on age, gender, body mass index (BMI), and hemoglobin (Hb)


, and hemoglobin (Hb))





)




)


4. Discussion
Colorectal cancer (CRC) is a common and highly diagnosable cancer. 134,490 new cases were estimated in 2016 and CRC is responsible for 8.3% of all deaths related to cancer. Colonoscopy has been the main screening tool known to help in decreasing high mortality associated with colorectal cancer. [1] A rate as high as 15-25% has been reported for sub-adequate colonoscopy preparations that lead to repeat colonoscopies. [5]
Many factors have been associated with inadequate bowel preparations. Several studies have shown that advanced age [6], male sex [7, 8], and comorbidities such as diabetes mellitus [9, 10], are independent risk factors for poor bowel preparation. Poor preparations warranting repeat procedures remain to be a burden on the healthcare system due to increased costs and time spent to decrease the rate of missed lesions. [11], [12] In addition, colonoscopies have been warranted more often in diabetics due to their gastrointestinal manifestations along with a higher incidence of CRC among them. [11], [12]
Diabetes mellitus (DM) has been well known to impair the gastrointestinal system. The negative influence that DM has on colonic motility because of autonomic neuropathy leading to impaired postprandial gastro colic response has been one of the widely seen underlying etiologies for poor preparation. [13] Delay of stool transit due to diabetic autonomic neuropathy along with an increased incidence of CRC by 1.16-1.30 in diabetics compared to non-diabetics urges for an improvement in colonoscopy preparations. [13] This study evaluated the possibility of inadequate glycemic control (characterized by HbA1c and MBGC) having an impact on poor bowel preparations.
A prior study conducted by Ozturk et al in Turkey showed that there was a statistically significant correlation between poor bowel cleansing quality and HbA1c levels along with the presence of late diabetic complications. [14] However, the Oztur et al. study only included 50 diabetic patients. In contrast, this study did not show an association between preparation quality and HbA1c levels and MBGC. One of the strengths of this study is there is a better representation of the general population as it included a diverse population with a sample of 380 consecutive diabetic patients.
Another study by Manhal Izzy et al also showed that the bowel preparation quality is not associated with the degree of glycemic control in DM, however, the study only relied on HbA1c as a measurement of glycemic control. [15] Instead, this study also explored for an association between MBGC at the time of the colonoscopy preparation. Although a higher MBGC has been previously shown to slower gastric emptying, this study further revealed that glycemic control most likely does not have an impact on colonoscopy preparation quality.
Although not significant, there was a trend of higher rate of good preparation overall for inpatient than outpatient groups. This may be the result of more frequent instruction for preparation by multiple disciplines (gastroenterology team, medical team, nursing staff) and closer observation by these disciplines to ensure compliance. In addition, inpatients tend to have tighter glucose monitoring in comparison to outpatients around the time of their colonoscopies, including right before the bowel preparation. Therefore, global outpatient education from endocrinology, gastroenterology, and primary care teams regarding finger stick monitoring, medication compliance and dietary restrictions may decrease the incidence of poor preps in outpatients.
Another strength of this study is that it is one of the first to look for possible variables within diabetics associated with an increase in poor bowel cleansing in a diverse patient population. This study also considered an association of obesity with poor preparations as metabolic syndrome has also been seen to be an independent risk factor for inadequate bowel cleansing.
Limitations to this study include a small proportion of the sample population having extremely high HbA1c, unknown status of patient medication use at the time of colonoscopy, and unknown past medical history, which may have affected gastric motility. Also, given the nature of the study being retrospective, limited data was available in terms of each subjects’ duration of the diabetes and their complications.
5. Conclusion
In conclusion, HbA1c levels and mean blood glucose concentration are not associated with colonoscopy bowel preparation quality. The underlying etiology for an increased likelihood of diabetics having poor preparations is still unknown. In addition, as inpatients tend to have stricter glycemic control on days prior to the procedure, an association between blood glucose levels days before procedure and preparation quality may be beneficial to explore.
Acknowledgements
None
Competing Interests
The authors have no competing interests.
Abbreviations
• EMR – electronic medical records
• MBGC - mean blood glucose concentration
• BMI – body mass index
• ANOVA – analysis of variance
• CRC – colorectal carcinoma
• DM – diabetes mellitus
References
| [1] | “SEER Stat Fact Sheets: Colon and Rectum Cancer.” October 2016. National Cancer Institute-Surveillance, Epidemiology, and End Results Program. <https://seer.cancer.gov/statfacts/html/colorect.html>. | ||
 In article In article | |||
| [2] | Lee, T.J., Nair, S., Beintaris, I. and Rutter, M.D, “Recent advances in colonoscopy,” F1000Research, 5. 2016. | ||
| In article | View Article | ||
| [3] | Bucci, C., Rotondano, G., Hassan, C., et al, “Optimal bowel cleansing for colonoscopy: split the dose! A series of meta-analyses of controlled studies,” Gastrointestinal endoscopy, 80 (4). 566-76. 2014. | ||
| In article | View Article PubMed | ||
| [4] | Taylor, C. and Schubert, M.L, “Decreased efficacy of polyethylene glycol lavage solution (golytely) in the preparation of diabetic patients for outpatient colonoscopy: a prospective and blinded study,” The American journal of gastroenterology, 96 (3). 710-4. 2001. | ||
| In article | View Article PubMed | ||
| [5] | Pyenson, B., Scammell, C. and Broulette, J, “Costs and repeat rates associated with colonoscopy observed in medical claims for commercial and Medicare populations,” BMC health services research, 14 (1). 92. 2014. | ||
| In article | View Article PubMed | ||
| [6] | Nguyen, D.L. and Wieland, M, “Risk factors predictive of poor quality preparation during average risk colonoscopy screening: the importance of health literacy,” J Gastrointestin Liver Dis, 19 (4). 369-72. 2010. | ||
| In article | PubMed | ||
| [7] | Ness, R.M., Manam, R., Hoen, H. and Chalasani, N, “Predictors of inadequate bowel preparation for colonoscopy,” The American journal of gastroenterology, 96 (6). 1797-802. 2001. | ||
| In article | View Article PubMed | ||
| [8] | Chan, W.K., Saravanan, A., Manikam, J., Goh, K.L. and Mahadeva, S, “Appointment waiting times and education level influence the quality of bowel preparation in adult patients undergoing colonoscopy,” BMC gastroenterology, 11 (1). 86. 2011. | ||
| In article | View Article PubMed | ||
| [9] | Chung, Y.W., Han, D.S., Park, K.H., et al, “Patient factors predictive of inadequate bowel preparation using polyethylene glycol: a prospective study in Korea,” Journal of clinical gastroenterology, 43 (5). 448-52. 2009. | ||
| In article | View Article PubMed | ||
| [10] | Alavi, A., Cohen, S. and Braunstein, S, “Colonic dysfunction in diabetes mellitus,” Gastroenterology, 79 (8). 1217-21. 1980. | ||
| In article | PubMed | ||
| [11] | Enck, P., Rathmann, W., Spiekermann, M., et al, “Prevalence of gastrointestinal symptoms in diabetic patients and non-diabetic subjects,” Zeitschrift fur Gastroenterologie, 32 (11). 637-41. 1994. | ||
| In article | PubMed | ||
| [12] | La Vecchia, C., Negri, E., Decarli, A. and Franceschi, S, “Diabetes mellitus and colorectal cancer risk,” Cancer Epidemiology and Prevention Biomarkers, 6 (12). 1007-10. 1997. | ||
| In article | |||
| [13] | Vinik, A.I., Maser, R.E., Mitchell, B.D. and Freeman, R, “Diabetic autonomic neuropathy,” Diabetes care, 26 (5). 1553-79. 2003. | ||
| In article | View Article PubMed | ||
| [14] | Ozturk, N.A., Gokturk, H.S., Demir, M., Unler, G.K., Gur, G. and Yilmaz, U, “Efficacy and safety of sodium phosphate for colon cleansing in type 2 diabetes mellitus,” Southern medical journal, 103 (11). 1097-102. 2010. | ||
| In article | View Article PubMed | ||
| [15] | Izzy, M., Changela, K., Alhankawi, D., Haeri, N.S., Shah, S., Jibara, G., Anand, S., et al, “Impact of glycemic control on colonoscopy outcomes: bowel preparation and polyp detection,” Annals of Gastroenterology: Quarterly Publication of the Hellenic Society of Gastroenterology, 29 (3). 332. 2016. | ||
| In article | PubMed PubMed | ||
 CiteULike
CiteULike Delicious
Delicious



 versus Colonoscopy preparation quality (good vs. poor) (p=0.23)){kind=link}
{kind=link}
 versus Colonoscopy preparation quality (good vs. poor) (p=0.18)){kind=link}
{kind=link}