 sciepub.com
sciepub.com
 Quick Submission
Quick Submission

Budesonide in Severe Alcoholic Hepatitis: Results of the Original Research
Komkova I.I.1, Tkachenko P.E.1, , Maevskaya M.V.1, Ivashkin V.T.1
, Maevskaya M.V.1, Ivashkin V.T.1
1Hepatology department, I.M.Sechenov First State Medical University, Moscow, Russia
Abstract
Background and aim: Severe alcoholic hepatitis (AH) is a life-threatening alcoholic liver disease with a potential of 30-40% mortality at 1 month. While steroids remain to be a first line therapy, there is a need in alternative treatment. The aim of the study is to compare efficacy and safety of budesonide and prednisolone in treatment of severe AH and to determine predictors of none-response, predictors of short-term mortality. Methods: 37 patients with severe AH were randomized in 2 groups and enrolled in the prospective trial. Group 1 (n=17) patients received budesonide 9 mg/daily per os, group 2 (n=20) patients were managed with prednisolone 40 mg/daily per os. Treatment duration was 28 days. Response criteria – Lille model. Results: There were no significant differences in short-term survival (р = 0,857). In group 2 adverse events were statistically more frequently than in group 1 (70% vs. 26,7%, р = 0,011). Hepatorenal syndrome occurred more frequently in group 2 (р = 0,033). Predictors of non-response were MELD score (р = 0,009), ABIC score (р = 0,011), hepatic encephalopathy (p=0,035), total bilirubin (p=0,016). Predictors of mortality were Lille score (p=0,018), serum glucose (p=0,017), total bilirubin level at the 7th day of the therapy (p=0,030). Conclusions: Budesonide therapy for patients with severe alcoholic hepatitis showed same efficacy as prednisolone treatment with significantly less adverse events. Budesonide appears to be effective in prevention of hepatorenal syndrome.
Keywords: severe alcoholic hepatitis, prednisolone, budesonide, hepatorenal syndrome
Copyright © 2016 Science and Education Publishing. All Rights Reserved.Cite this article:
- Komkova I.I., Tkachenko P.E., Maevskaya M.V., Ivashkin V.T.. Budesonide in Severe Alcoholic Hepatitis: Results of the Original Research. American Journal of Clinical Medicine Research. Vol. 4, No. 1, 2016, pp 7-10. http://pubs.sciepub.com/ajcmr/4/1/2
- I.I., Komkova, et al. "Budesonide in Severe Alcoholic Hepatitis: Results of the Original Research." American Journal of Clinical Medicine Research 4.1 (2016): 7-10.
- I.I., K. , P.E., T. , M.V., M. , & V.T., I. (2016). Budesonide in Severe Alcoholic Hepatitis: Results of the Original Research. American Journal of Clinical Medicine Research, 4(1), 7-10.
- I.I., Komkova, Tkachenko P.E., Maevskaya M.V., and Ivashkin V.T.. "Budesonide in Severe Alcoholic Hepatitis: Results of the Original Research." American Journal of Clinical Medicine Research 4, no. 1 (2016): 7-10.
| Import into BibTeX | Import into EndNote | Import into RefMan | Import into RefWorks |
At a glance: Figures
1. Introduction
The use of alcoholic beverages has been an integral part of many cultures. However, heavy drinking can cause both somatic and psychiatric disorders. The association between alcohol consumption and internal injury is well established [1, 2]. Alcohol has a great impact on the liver and can lead to the development of alcoholic liver disease (ALD). Chronic consumption of alcohol can cause a spectrum of liver abnormalities, ranging from simple steatosis (fatty liver) to steatohepatitis, cirrhosis and hepatocellular carcinoma [1]. However, only 10-35% of consistent, heavy drinkers will develop alcoholic hepatitis (AH) and only 8-20% will progress to liver cirrhosis, which suggests that other host or environmental factors are important in the evolution of alcohol-related liver disease [4, 5, 6, 7].
AH is a distinct manifestation of alcoholic liver disease characterized by jaundice and liver failure, with up to 30%–40% mortality at 1 month after diagnosis for those with severe disease [8, 9]. Various scores have been developed to identify patients with severe AH including the Model for End-Stage Liver Disease (MELD); Maddrey (mDF); GASH; and Age, serum Bilirubin, INR, and serum Creatinine (ABIC) [10]. Corticosteroids like prednisolone remain a mainstay of treatment for severe AH, though they are not effective in all patients. In addition, side effects of prednisolone are common and sometimes severe enough to require drug discontinuation [9, 11, 12]. Steroids equivalent to prednisolone in efficacy but with better side effect profiles are needed.
Budesonide is a second-generation glucocorticosteroid with an affinity for glucocorticoid receptors in the liver 15 times greater than that of prednisone [21]. Its higher affinity and lower side-effect profile make it an alternative therapeutic option. It has been successfully applied in autoimmune hepatitis and inflammatory bowel disease in place of prednisolone [13-18][13]. In this study, we aimed to evaluate the efficacy and tolerability of budesonide as an alternative first line treatment option for severe AH.
2. Methods
We performed a multicenter randomized controlled trial. Patients hospitalized between 2011 and 2013 for severe alcoholic hepatitis at 3 Russian hospitals were considered for eligibility. Patents met study eligibility criteria if they had average alcohol consumption of greater than 50 g per day in the 3 months before enrollment, screened positive for excessive drinking with an AUDIT score ≥ 8 points and CAGE questionnare score ≥ 3 points, were 18 years of age or older, and had a Maddrey’s discriminant function of 32 or more.
Key exclusion criteria were hepatocellular carcinoma; SAMe; UDCA or pentoxifillin administration prior to hospitalization; uncontrolled bacterial infection or gastrointestinal hemorrhage in the previous 4 days; infection with hepatitis C virus (HCV), hepatitis B virus (HBV), or human immunodeficiency virus (HIV); autoimmune hepatitis; hemochromatosis; Wilson’s disease; alpha1-antitrypsin deficiency; acetaminophen-induced hepatitis; cancer; psychiatric disease; drug abuse; or serious cardiac, respiratory, or neurologic disease.
2.1. Study DesignPatients who met the eligibility criteria were enrolled and randomly assigned to receive either prednisolone or budesonide. Investigators and patients were not blinded to treatment assignments. The experimental protocol was approved by the medical ethics committee of our hospital, and all patients or their medical proxy signed an informed consent form.
All study participants underwent an initial clinical examination that recorded vital signs (heart rate, blood pressure, temperature) and assessed for hepatic encephalopathy, ascites, gastrointestinal hemorrhage, and jaundice. Alcohol consumption was evaluated using the AUDIT and the CAGE questionnaires [19].
Patients were monitored with serial physical examinations and laboratory tests until the end of the study. At baseline, day 7, and day 28, clinical variables and laboratory values were used to calculate Child-Turcotte-Pugh (CTP), mDF, MELD, and ABIC scores as indicators of liver failure and prognosis. Patients were screened for bacterial infections through serial checks of urine, ascites, blood, and chest radiography. The Lille model was used to assess therapy response on day 7 of therapy [20].
2.2. Study TreatmentsPatients randomized to the treatment arm received 9 mg oral budesonide per day for 28 days. Patients in the control group received 40 mg oral prednisolone per day for 28 days. Prednisolone regimen was chosen according to EASL guidelines for severe alcoholic hepatitis. Budesonide 9 mg per day is currently used for autoimmune liver diseases and inflammatory bowel diseases as an alternative option to prednisolone. We considered this regimen to be appropriate for AH. By the time of the study we had no evidence of using budesonide in AH. Throughout the study, diuretics, albumin, fresh frozen plasma, and antibiotics were administered if medically indicated. The use of acetaminophen, pentoxifylline, or anti–TNF-α treatments was prohibited. All patients received standardized hospital nutrition consisting of 1800 to 2000 kcal per day, with sodium restriction initiated as medically indicated.
2.3. Study OutcomesThe primary study outcome was survival at 40 days. Secondary outcomes included changes in ALT, AST, γGT and bilirubin; rate of hepatitis complications; and adverse events.
2.4. Statistical AnalysisDescriptive statistics were used to summarize the data. Quantitative variables, expressed as means ±SD, were compared using the Wilcoxon test, Mann-Whitney U-test, or Student’s t-test as appropriate. Qualitative variables, expressed as percentages, were compared using the chi-square test or Fisher’s exact test. Kaplan–Meier survival curves were plotted for up to 40 days and compared using a log-rank test. Factors predictive of mortality in univariate analysis (p<0.05) were included in multivariate Cox logistic regression. Statistical analyses were performed by SPSS (Statistical Package for the Social Sciences) 17.0 with p-values <0.05 considered significant. All reported p-values are two-sided.
3. Results
A total of 179 patients with ALD were evaluated for eligibility. 37 patients met the inclusion criteria and were enrolled in the study. Of these, 17 patients received budesonide (experimental group) and 20 received prednisolone (control group). Two patients from the budesonide group failed to maintain abstinence from alcohol in first 3 days and were therefore excluded.
The two groups were similar in major characteristics with the exception of gender. Females were predominant in the budesonide group, while the prednisolone group had significantly more males. Although females tend to develop severe ALD at lower doses of alcohol [5], there is no evidence showing that corticosteroid therapy is more efficacious in females than in males. Previous studies showed that gender and age did not influence the pharmacokinetics of both budesonide and prednisolone [15].







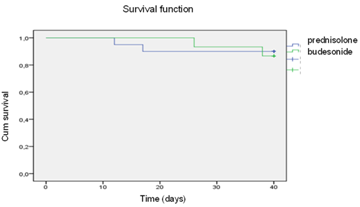
Two patients from the budesonide group (11.8%) and two patients from the prednisolone group (10%) died. Kaplan-Meier analysis showed no significant differences between the two groups (p = 0.810, Log-Rank; p = 0.857, Breslow).
 Download as
Download as

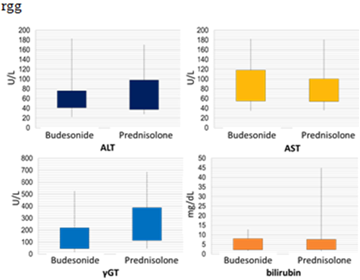
At day 28 there were no significant differences in key laboratory tests evaluated: ALT (p = 0.492), AST (p = 0.551), γGT (p = 0.12), and bilirubin (p = 0.899).
 Download as
Download as
 Download as
Download as
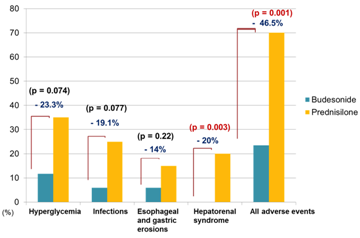
The rate of hepatorenal syndrome was 20% in the prednisolone group (4 of 20 patients) and 0% in the budesonide group (p = 0.003). The overall rate of infection was 25% (5 of 20 patients) in the prednisolone group and 6.7% (1 of 17 patients) in the budesonide group (p = 0.077). Hyperglycemia occurred in 35% (7 of 20 patients) in the prednisolone group and was seen in 13.3% (2 of 17 patients) in the budesonide group (p = 0.073). The two groups did not differ significantly with respect to other complications. Overall, 70% of patients (14 of 20) in the prednisolone group had at least one adverse event versus 23.5% of patients (4 of 17) in the budesonide group (p = 0.011).
3.4. Predictive Factors for DeathWe used a Cox regression model to reveal factors independently associated with increased mortality. Elevated baseline glucose level (p = 0.017), higher Lille score at 40 days (p = 0.018) and higher bilirubin level on day 7 (p = 0.03) were significantly associated with mortality. We then used Kaplan–Meier survival curves to analyze the impact of complications from corticosteroid therapy on survival. Hyperglycemia (p = 0.006) and new infection (p = 0.002) during hospitalization were significantly associated with decreased survival.
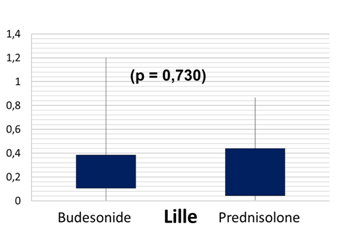
3.5. Response to Treatment as Measured by the Lille ModelResponders and nonresponders were compared to determine factors independently associated with response to corticosteroid therapy using Cox regression models. Higher grade encephalopathy (p = 0.035); higher ABIC (p = 0.011) and MELD score (p = 0.023); and higher baseline bilirubin level (p = 0.016) were significantly associated with response to corticosteroid therapy (Lille model <0.45).
 Download as
Download as
4. Discussion
In patients with severe AH, budesonide was not superior to prednisolone in terms of response to treatment and 40-day survival. The metabolism of budesonide is severely affected in patients with advanced liver disease and extensive fibrosis, which can decrease the drug’s beneficial effects on liver function [21]. A recent study examining efficacy and tolerability of budesonide in autoimmune hepatitis (AIH) showed that treatment failure was more commonly observed in patients with liver fibrosis than in patients without fibrosis (60% vs. 12.5%, p = 0.066). In that study, treatment failure was observed in a total of 7 patients, 6 of whom had varying degrees of fibrosis on liver biopsy. Three of the 7 patients had AIH/PBC overlap, making it hard to determine negative effects of cholestasis on treatment response in these patients [22]. In the present study, all patients in the budesonide group had liver cirrhosis. Treatment response was achieved in 80% of patients, a rate similar to that seen in the prednisolone group.
The main features of budesonide that make it an attractive treatment option are its safety profile and the lower incidence of associated side effects. In our study, the rate of all adverse events was significantly lower in the budesonide group (p = 0.011). HRS occurred in 4 of the 20 patients in the prednisolone group, while no cases of HRS were registered in budesonide group. Creatinine level had risen in the prednisolone group at 7 days (p = 0.004). Differences in creatinine level between the two groups at 28 days were also significant (p = 0.003). The glomerular filtration rate (GFR), as measured by the Cockcroft-Gault formula, tended to increase in the budesonide group while decreasing in prednisolone group, though the difference was not significant at 7 or 28 days (p = 0.094 and 0.061, respectively). The exact mechanism of budesonide’s apparent nephroprotective effect is not clear, and further research in this area is needed.
In previous studies [23] budesonide has been reported to increase the risk of thrombotic complications in patient with liver cirrhosis. Cirrhotic patient with autoimmune hepatitis have developed Budd-Chiari syndrome after switching to budesonide therapy, requiring budesonide to be discontinued and treatment with prednisolone resumed. Two months later, hepatocellular carcinoma was diagnosed. Neoplasia tends to increase the risk of hypercoagulation, even though in that study HCC did not reveal signs of vascular invasion on post-OLT histology. Nevertheless, the association between budesonide and Budd-Chiari syndrome is unclear [23].
In another study, budesonide had marked differences in pharmacokinetics and tolerability in patients with early-stage PBC versus those with late-stage PBC. Two patients with stage IV PBC developed PVT shortly after administration of budesonide.
At the same time, patients with cholestatic liver diseases such as PBC and primary sclerosing cholangitis are known to be more prone to hypercoagulation. It remains unclear whether cirrhotic patients are at higher risk for budesonide-associated thrombosis than cirrhotic patients with other forms of liver disease [22]. Among 15 patients receiving 9 mg of prednisolone per day for 28 days in our trial, CTP class C cirrhosis was diagnosed in 14 cases but no thrombotic complications were observed.
We conclude that budesonide therapy for patients with severe alcoholic hepatitis was effective and resulted in significantly less adverse events, particularly hepatorenal syndrome, when compared to prednisolone. We believe that further trials of budesonide as an alternative therapeutic option for patients with severe alcoholic hepatitis are needed.
References
| [1] | Mayevskaya M.V., Morozova M.A., Ivashkin V.T. Algorithm of management of patient with alcohol-induced liver disease. Russian journal of gastroenterology, hepatology and coloproctology. 2011. Vol. 17 (6), p. 4-10. | ||
 In article In article | |||
| [2] | Bueverov A.O., Mayevskaya, M.V., Ivashkin V.T. Differentiated management of alcoholic liver disease.– Russian journal of gastroenterology, hepatology and coloproctology. 2005. Vol. 15 (5), p. 4-10. | ||
| In article | |||
| [3] | Ivashkin V.T. Gastroenterology: textbook – “Geotar-Media”, 2015. | ||
| In article | |||
| [4] | Mayevskaya M.V. Alcohol, alcoholism and related consequences. Russian journal of gastroenterology, hepatology and coloproctology. 2013. Vol. 23 (6), p. 43-48. | ||
| In article | |||
| [5] | Fernández-Checa JC. Alcohol-induced liver disease: when fat and oxidative stress meet. Ann Hepatol. 2003 Apr-Jun; 2 (2): 69-75. | ||
| In article | PubMed | ||
| [6] | Limuro Y., Frankenberg M., Arteel G. et al. Female rats exhibit greater susceptibility to early alcohol-induced liver injury than males. Am. J. Physiol. 1997; 272: 1186-1194. | ||
| In article | |||
| [7] | Naveau S., Cassard-Doulcier A., Njiké-Nakseu M., Bouchet-Delbos L., Barri-Ova N., Boujedidi H., Dauvois B. et. al. Harmful effect of adipose tissue on liver lesions in patients with alcoholic liver disease. J Hepatol. 2010 Jun; 52 (6): 895-902. Epub 2010 Mar 24. | ||
| In article | View Article PubMed | ||
| [8] | Mathurin P. Therapeutic management of alcoholic hepatitis. Clinical Research in Hepatology and Gastroenterology. 2015 Jul; 39: 41-45. | ||
| In article | View Article PubMed | ||
| [9] | O’Shea R.S., Dasarathy S., McCullough A.J. et al. Alcoholic liver disease. AASLD practice guidelines. Hepatology. 2010; 51(1): 307-328. | ||
| In article | View Article PubMed | ||
| [10] | Sheth M, Riggs M, Patel T. Utility of the Mayo End-Stage Liver Disease (MELD) score in assessing prognosis of patients with alcoholic hepatitis. BMC Gastroenterol. 2002; 2: 2. | ||
| In article | View Article PubMed | ||
| [11] | Mayevskaya M.V., Morozova M.A., Ivashkin V.T. Management of patients with alcoholic liver disease. - Russian journal of gastroenterology, hepatology and coloproctology. 2007; 17(6): 1-10. | ||
| In article | |||
| [12] | P. Maturin, M.R. Lucey. Management of alcoholic hepatitis. Journal of Hepatology. 2012; 56, supplement 1: 39-45. | ||
| In article | View Article | ||
| [13] | Manns MP, Woynarowski M, Kreisel W, Lurie Y, Rust C, Zuckerman E, Bahr MJ et. al. European AIH-BUC-Study Group Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis. Gastroenterology. 2010 Oct; 139(4): 1198-206. Epub 2010 Jun 22. | ||
| In article | View Article PubMed | ||
| [14] | Zandieh I, Krygier D, Wong V, Howard J, Worobetz L, Minuk G, Witt-Sullivan H et. al. The use of budesonide in the treatment of autoimmune hepatitis in Canada. Can J Gastroenterol. 2008 Apr; 22(4): 388-92. | ||
| In article | PubMed | ||
| [15] | Czaja AJ. Autoimmune hepatitis: Focusing on treatments other than steroids. Can J Gastroenterol. 2012 Sep; 26(9): 615-20. | ||
| In article | View Article | ||
| [16] | D'Haens GR, Kovács A, Vergauwe P, Nagy F, Molnár T, Bouhnik Y, Weiss W et. al. Clinical trial: Preliminary efficacy and safety study of a new Budesonide-MMX® 9 mg extended-release tablets in patients with active left-sided ulcerative colitis. J Crohns Colitis. 2010 Jun; 4(2): 153-60. Epub 2009 Oct 24. | ||
| In article | View Article PubMed | ||
| [17] | Seow CH, Benchimol EI, Griffiths AM, Otley AR, Steinhart AH. Budesonide for induction of remission in Crohn's disease. Cochrane Database Syst Rev. 2008 Jul 16; (3). | ||
| In article | |||
| [18] | Wagner M, Lampinen M, Sangfelt P, Agnarsdottir M, Carlson M. Budesonide treatment of patients with collagenous colitis restores normal eosinophil and T-cell activity in the colon. Inflamm Bowel Dis. 2010 Jul; 16(7): 1118-26. | ||
| In article | View Article PubMed | ||
| [19] | Bush KR, Bradley KA, McDonell MB, Malone T, Fihn SD; Screening for problem drinking: Comparison of CAGE and AUDIT. Ambulatory Care Quality Improvement Project. J Gen Intern Med. 1998 Jun; 13 (6): 379-88. | ||
| In article | View Article PubMed | ||
| [20] | Louvet A, Naveau S, Abdelnour M, Ramond MJ, Diaz E, Fartoux L, Mathurin P. et. al. The Lille model: a new tool for therapeutic strategy in patients with severe alcoholic hepatitis treated with steroids. Hepatology. 2007 Jun; 45 (6): 1348-54. | ||
| In article | View Article PubMed | ||
| [21] | Hempfling W., Grunhage F., Dilger K., Reichel C, Beuers U., Sauerbruch T. Pharmacokinetics and Pharmacodynamic Action of Budesonide in Early- and Late-Stage Primary Biliary Cirrhosis. Hepatology. 2003 Jul; 38 (1): 196-202. | ||
| In article | View Article PubMed | ||
| [22] | Efe C., Ozaslan E., Kav T. Liver fibrosis may reduce the efficacy of budesonide in the treatment of autoimmune hepatitis and overlap syndrome. Autoimmunity Reviews 11 (2012): 330-33. | ||
| In article | View Article PubMed | ||
| [23] | Mederacke I., Helfritz F., Puls F. Budd-Chiary syndrome after treatment with budesonide in a cirrhotic patient with autoimmune hepatitis. Annals of Hepatology. 2012; 11(1), p 143-144. | ||
| In article | PubMed | ||
 CiteULike
CiteULike Delicious
Delicious



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}