The transition to total edentulism has always been a particularly brutal and traumatic experience for most patients. Nowadays, people who have had their teeth removed are reluctant to expose their disability. The problem becomes even more acute when the anterior region is involved. In such cases, the practitioner must know how to respect these fundamental functional and aesthetic criteria linked to his patient's rehabilitation. Immediate complete dentures are an unavoidable therapeutic solution to respect the aesthetic prejudice. The value of immediate dentures is well established. it has become an essential and unavoidable step to avoid or reduce the aesthetic, functional and psychological consequences of the loss of anterior teeth. The aim of this article is to propose a complete protocol for the realization of an immediate complete dentures, highlighting the key points, difficulties and errors that the practitioner may encounter, through a clinical case. The production of this prosthesis is one of the most difficult and least predictable.
Despite advances in prevention, the transition to total edentulism remains a hot topic. Today, mainly due to increasing life expectancy and an aging population, the number of edentulous people in the world is constantly on the rise. The World Health Organization (WHO) even predicts that 30% of the world's population will be edentulous by 2030. 1, 2
Tooth loss has a number of consequences for our patients. Firstly, there is a functional problem, with disturbances in chewing, eating, speaking, swallowing and salivating. Secondly, edentulism has aesthetic, anatomical and psychological repercussions. The abrupt transition from partial to total edentulism is logically dreaded by the patient. One of the practitioner's imperatives is to make the transition to total edentulism once the indication has been established. The placement of an immediate complete denture can represent a therapeutic solution.
An immediate complete denture is a prosthesis made in the presence of the patient's residual teeth and inserted on the day the teeth are avulsed. It offers numerous advantages, not only aesthetic and psychological, but also functional and biological.
Immediate complete denture can restore, and sometimes even improve, the patient's aesthetics, preventing the patient from becoming edentulous while a total prosthesis is being fitted. 3 Depending on the clinical situation, the presence of residual natural teeth can give an indication as to the choice and fitting of prosthetic teeth (color, size, shape). 4
The transition to total edentulism can be psychologically brutal and is dreaded by patients. Immediate total prosthesis avoids this situation by fitting the prosthesis immediately after the avulsion of the residual teeth. The patient is never exposed to his or her handicap, and can quickly resume a normal social life. 5
The elimination of inflammatory and infectious foci improves the patient's oral health. What's more, the prosthesis inserted immediately after extraction of the residual teeth acts as a dressing. The prosthesis ensures hemostasis and holds the blood clot in place, particularly during feeding, thus limiting post-operative oedema. Secondly, immediate insertion of the prosthesis will help to guide healing and preserve bone capital as much as possible. Bone resorption is limited thanks to a stable, balanced occlusion. 6, 7, 8
Immediate full prosthesis restores occlusal function, taking into account various factors (occlusal plane, vertical occlusal dimension, reference condylar position). Changes in maxillo-mandibular relations require a period of neuromuscular re-education.
However, even though immediate total dentures offer many advantages, there are a number of disadvantages, such as the absence of an esthetic fitting. In addition, there may be problems in fitting the prosthesis, due to a correction on the working cast (removal of teeth, provision for subtractive osteoplasty). Finally, the transition to total edentulism requires considerable psychological support to reduce the patient's apprehension, whether about total edentulism, the surgical procedure or his or her new appearance. 5
It is therefore of vital importance for the practitioner to know how to identify and master these difficulties, so as to be able to anticipate them. The purpose of this article is to provide the key stages and criteria for the realization of the immediate complete prosthesis and thus avoid a possible failure on the day of fitting.
A 54-year-old female patient with CL I of Kennedy partial edentulism in the maxilla and subtotal edentulism in the mandible.
Clinical and radiological examination revealed cervico-radicular caries on residual teeth, occlusal caries on 13-14 and chronic periodontitis with moderate to terminal lysis on all maxillary and mandibular teeth, mobilities and recessions, therefore all teeth are destined for extraction. (Figure 1)

Considering the patient's aesthetic requirements, the severity of the periodontal lesions and the resorption of the alveolar ridges, the prosthetic rehabilitation envisaged is an immediate full denture.
This prosthesis will preserve existing bone capital, guide healing and bone remodeling thanks to the use of a surgical guide and the establishment of a balanced occlusion, thus reducing resorption, create a real surgical dressing, maintain the patient's correct vertical occlusal dimension, and ensure a psychologically trauma-free transition to total edentulism.
The preparatory phase consists of avulsion of the posterior teeth. Obtaining a healed osteo-fibromucosal bearing surface is important to ensure stable support of the prosthesis and guide healing of the avulsion of the anterior block. 9 In addition, avulsion of the posterior teeth also avoids interference during registration of the inter-maxillary relationship, and provides better registration of the osteo-mucosal bearing zones. A healing delay may be necessary at the extraction sites to ensure pain-free healing of the mucosa.
In order to record the anatomy of the dentate and edentulous areas, and also to record the physiological mucosal reflection line, a primary impression was taken with alginate, and given the mobility of the anterior teeth, a retainer was required to prevent tooth avulsion during the impression process.
Casting the primary impression gives us a model on which an individual resin impression tray is built.
The limits of the individual impression tray in edentulous areas are similar to those of a complete denture: 1 to 1.5 mm below the vestibular fundus, at the level of the vestibular fundus in the para-tuberosity area, 2 mm behind the bending line of the soft tissue and 2 mm from the brakes and flanges.
Depending on the clinical situation, several types of individual impression tray can be produced: open-tooth trays for residual teeth and full-tooth trays.
After adaptation of individual impression trays, thermoplastic Kerr paste is applied to the edentulous areas to obtain the peripheral border tray modeling and posteriorly the velopalatal border tray, which is the junction between the hard palate (non-mobile during phonation) and the soft palate (mobile during phonation), also called the post-dam. In the toothed anterior region, a soft border tray modeling is created using Imprégum. (Figure 2) The Central impression is made with polyethers. (Figure 3) due to the fact that the erupted anterior-superior teeth interfered with the fox ruler, the occlusal plane was set in a lower parallel plane, approaching the free borders of the residual teeth without any contact whatsoever. (Figure 4)



Determining the position of the future inter-incisal point is a crucial step for the functional and aesthetic success of the future prosthesis. 10 The patient is affected by periodontal disease, with egression and vestibuloversion of the maxillary anterior block, resulting in an inter-incisal point that is lower and more anterior than the ideal inter-incisal point, they are also laterally displaced. It is raised by 3.5mm and shifted to the right by 1mm, in the sagittal plane the inter-incisal point is set back approximately 2mm. (Figure 5)

The Occlusal Plane is set lower on the occlusal rims than the ideal plane where the desired PI for the future prosthesis is located. D is the distance between these two planes (D= 3.5 mm). (Figure 6)

The maxillary model is placed in the articulator by increasing the vertical dimension at the incisal edge by the previously measured D value, increased by one third to compensate for the incisal edge's distance from the inter-incisal point and the articulator's axis of rotation. (Figure 6a) The maxillary model is then centered symmetrically with respect to the inter-incisal point of the teeth placed 2mm in front of the cross geometrically materializing the ideal positioning of the PI in the case of normocclusion. (Figure 6b)
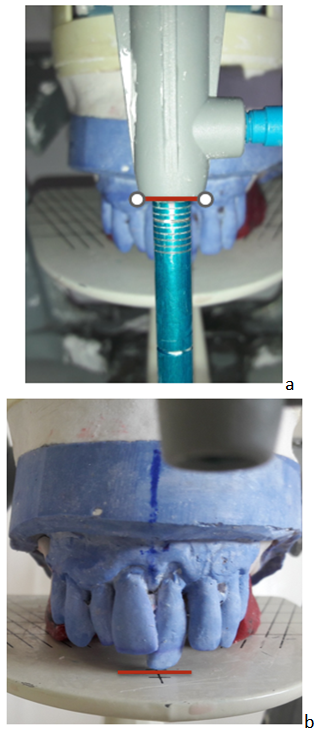
Figure 6 a b. Articulator mounting of the maxillary model
Once the maxillo-mandibular relationship has been recorded, the shape, size, color and material of the prosthetic teeth are determined.
Then, in order to visualize the amount of resection, a vestibular silicon key was made, and an anterior mordu key was used to transfer the inter-incisal point.
One of the keys to immediate total prosthetics is the anticipatory preparation of the working model. Only the practitioner has the clinical data to anticipate alveolar resorption and assess alveolysis of residual teeth (X-rays, periodontal probing, etc.). Correcting the model is a kind of surgical simulation.
The teeth are then fitted in accordance with aesthetic requirements and functional imperatives, particularly phonetic ones.
The immediate total removable prosthesis is then polymerized.
The surgical phase in total immediate prosthetics follows a very specific protocol, which consists firstly of avulsing the anterior teeth, and secondly of performing osteoplasty using the surgical guide. (Figure 7)

Once hemostasis has been achieved using the surgical guide, the prosthesis is inserted and the occlusion checked for simultaneous bilateral occlusal contact between the second premolars and first molars, and for the absence of anterior contact. (Figure 8)

Immediately after the operation, an ice pack is applied to the surgical area. Post-operative advice is given as follows.
Follow-up surgery is performed at 48h, the prosthesis is removed and cleaned. Healing is checked and the occlusion corrected if necessary. Bilateral contacts in the posterior sectors are sought in maximum intercuspidial occlusion.
Prostheses are checked cyclically until they are functionally and aesthetically integrated.
As the population ages and life expectancy increases, we are faced with a growing number of patients who are edentulous or candidates for total edentulism. This is an extreme mutilation of the oral cavity, affecting vital and psycho-affective functions such as chewing, swallowing, phonation, smiling and kissing, and thus impacting on patients' psycho-social well-being. Accompanying patients as they make the transition to full edentulism, and ensuring the success of their prosthetic treatment, are key factors in preventing or correcting any deterioration in their general state of health. Faced with this real public health problem, there is today a wide range of treatment solutions, including long transitional prostheses, supra-dental complete removable prostheses and immediate complete removable prostheses. Due to the tissue changes associated with bone and mucosa healing, there are two types of immediate prosthesis: the transitional immediate prosthesis and the customary immediate prosthesis. 11
The immediate prosthesis is designed and fabricated entirely before the last teeth are avulsed, and inserted on the day of avulsion. It is by no means a temporary prosthesis. 12
The immediate complete prosthesis meets all the criteria for a successful of a conventional prosthesis. Its aim is to maintain patient's maxillary anterior teeth during all phases of prosthetic of the prosthesis until the day it is fitted. 13
In addition to psychological and functional goals, the main objective of the of the immediate complete prosthesis is to preserve existing bone tissue by minimizing resorption 4
The immediate complete prosthesis is immediately the patient's prosthesis of choice.
The patient feels at the end of his or her treatment, thus encouraging good cooperation and easier adaptation to his or her new condition. and easier adaptation to their new condition 9
It preserves or improves aesthetics, sparing the patient the handicap of being totally edentulous while the prosthesis is being fitted.
The patient can then continue to speak, smile and interact with his or her social environment, and quality of life can be preserved. 3
In addition, immediate prosthetics ensure that orofacial functions are preserved, as they do not expose the patient to a phase of total edentulism without a prosthesis. In fact, it not only enables the patient to chew and swallow satisfactorily, but also ensures optimal phonation. 13, 14
On the other hand, immediate insertion of the prosthesis provides permanent support of the paraprosthetic organs, preserving their position and tone.
The prosthetic space is no longer in danger of being reduced by sagging cheeks and lips, and the prosthetic extrados simply take over from the dental units. The tongue is also held in place, preventing it from extending laterally over the ridges. 15, 16
The immediate complete prosthesis is, in fact, a definitive prosthesis that follows rigorous and perfectly defined technical steps. 17 This type of prosthesis has all the success factors of a definitive prosthesis, featuring, impression techniques adapted to clinical conditions; restoration of stable occlusal relationships in a bilaterally balanced pattern and anterior teeth set-up that takes into account the aesthetics of the remaining natural teeth. 18, 19
The advantages of this particular technique are numerous and justify its interest. 20
Immediate full dentures appear to be an effective solution for the transition to full edentulism. It offers the patient a simple aesthetic and functional rehabilitation, while saving time, comfort and money.
However, the success of this therapy is particularly dependent on the human qualities of the dentist, given the psychological difficulties inherent in edentulous patients, and the limitations of immediate full Thus, the patient's psychological preparation, the quality and precision of the pre-prosthetic steps, and regular monitoring are essential prerequisites for therapeutic success.
| [1] | Pouysségur V., Montal S., Dupuis V. Prothèse amovible complète immédiate : les dernières dents garder ou extraire. Edition Espace Id 2011. | ||
| In article | |||
| [2] | Douglass CW, Jiménez MC. Our Current Geriatric Population: Demographic and Oral Health Care Utilization. Dental Clinics of North America. 1 oct 2014; 58(4): 717-28. | ||
| In article | View Article PubMed | ||
| [3] | Demurashvili G, Davarpanah K, Boittin A, Postaire M, Raux D. Intérêt de la prothèse complète immédiate bi-maxillaire. Strat Prothétique. janv 2012; 12(1): 49-57. | ||
| In article | |||
| [4] | Berteretche MV, Pennequin G. Prothèse immédiate : esthétique et montage antérieur. Rev Odontostomatol (Paris) 1999;28:105-1. | ||
| In article | |||
| [5] | Rignon-Bret C. Prothèse totale immédiate. Cdp. 2020. (MÉMENTO). | ||
| In article | |||
| [6] | Tallgren A, Lang BR, Walker GF, Ash MM Jr. Roentgen cephalometric analysis of ridge resorption and changes in jaw and occlusal relationships in immediate complete denture wearers. J Oral Rehabil. 1980 Jan; 7(1): 77-94. | ||
| In article | View Article PubMed | ||
| [7] | Van Waas MA, Jonkman RE, Kalk W, Van ’t Hof MA, Plooij J, Van Os JH. Differences two years after tooth extraction in mandibular bone reduction in patients treated with immediate overdentures or with immediate complete dentures. J Dent Res. 1993 Jun; 72(6): 1001-4. | ||
| In article | View Article PubMed | ||
| [8] | Berteretche M-V, Hüe O. Prothèse complète immédiate : EMC 2008. | ||
| In article | |||
| [9] | Pompignoli M, Postaire M, Raux D. La prothèse complète immédiate. Paris: Quintessence; 2004. | ||
| In article | |||
| [10] | Janati G., Bellemkhannate S. Integration esthétique de la prothèse complete : Intérêt de la prothèse immédiate et des empreintes à visée esthétique. Le Courrier du dentiste 2012. | ||
| In article | |||
| [11] | Bissasu M. A simple procedure for minimizing adjustment of immediate complete denture: a clinical report. J Prosthet Dent. août 2004; 92(2): 125-7. | ||
| In article | View Article PubMed | ||
| [12] | Berteretche M, Hüe O. La prothèse complète immédiate : une entité, mais différentes approches. Cah Proth. 1998; (104): 89-101. | ||
| In article | |||
| [13] | Hüe O, Berteretche M. Prothèse complète: Réalité clinique, Solutions thérapeutiques. Paris: Quintessence; 2003. | ||
| In article | |||
| [14] | Hüe O, Braud A, Berteretche M. Prothèse complète immédiate : comment gérer l’esthétique? Strat Prothétique. avr 2007; 7(2): 111-20. | ||
| In article | |||
| [15] | Sadowsky S. Use of foil to block out extraction sites prior to relining immediate dentures. J Prosthet Dent. janv 2006; 95(1): 79. | ||
| In article | View Article PubMed | ||
| [16] | Sadowsky S, Gupta S, Gonzales E. A technique to correct incisal plane error in maxillary immediate denture therapy. J Prosthet Dent. août 2013; 110(2): 141-3. | ||
| In article | View Article PubMed | ||
| [17] | Postaire M, Demurashvili G, Vicaux F, Raux D. La prothèse complète immédiate mandibulaire, une solution simple... et efficace. Strat Prothétique. Mars 2010; 10(2): 139-46. | ||
| In article | |||
| [18] | Postaire M, Herbout B. Intérêt de la précision dans la détermination et dans l’enregistrement du rapport mandibulo-maxillaire chez l’édenté total. StratProthétique. juin 2016; 16(3): 197-202. | ||
| In article | |||
| [19] | Postaire M, Pompignoli M. Les dernières dents... Garder ou extraire : solutions cliniques. Paris: Espace ID; 2011. | ||
| In article | |||
| [20] | Viennot S, Moyencourt C, Millet C, Buch D. Réhabilitation esthétique et fonctionnelle par prothèse complète immédiate : étapes cliniques. juin 2004; (126): 9-18. | ||
| In article | |||
Published with license by Science and Education Publishing, Copyright © 2024 Fatima Zahra Ghazzar, Rabab Elabdouli and Samira Bellemkhannate
![]() This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
This work is licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/
| [1] | Pouysségur V., Montal S., Dupuis V. Prothèse amovible complète immédiate : les dernières dents garder ou extraire. Edition Espace Id 2011. | ||
| In article | |||
| [2] | Douglass CW, Jiménez MC. Our Current Geriatric Population: Demographic and Oral Health Care Utilization. Dental Clinics of North America. 1 oct 2014; 58(4): 717-28. | ||
| In article | View Article PubMed | ||
| [3] | Demurashvili G, Davarpanah K, Boittin A, Postaire M, Raux D. Intérêt de la prothèse complète immédiate bi-maxillaire. Strat Prothétique. janv 2012; 12(1): 49-57. | ||
| In article | |||
| [4] | Berteretche MV, Pennequin G. Prothèse immédiate : esthétique et montage antérieur. Rev Odontostomatol (Paris) 1999;28:105-1. | ||
| In article | |||
| [5] | Rignon-Bret C. Prothèse totale immédiate. Cdp. 2020. (MÉMENTO). | ||
| In article | |||
| [6] | Tallgren A, Lang BR, Walker GF, Ash MM Jr. Roentgen cephalometric analysis of ridge resorption and changes in jaw and occlusal relationships in immediate complete denture wearers. J Oral Rehabil. 1980 Jan; 7(1): 77-94. | ||
| In article | View Article PubMed | ||
| [7] | Van Waas MA, Jonkman RE, Kalk W, Van ’t Hof MA, Plooij J, Van Os JH. Differences two years after tooth extraction in mandibular bone reduction in patients treated with immediate overdentures or with immediate complete dentures. J Dent Res. 1993 Jun; 72(6): 1001-4. | ||
| In article | View Article PubMed | ||
| [8] | Berteretche M-V, Hüe O. Prothèse complète immédiate : EMC 2008. | ||
| In article | |||
| [9] | Pompignoli M, Postaire M, Raux D. La prothèse complète immédiate. Paris: Quintessence; 2004. | ||
| In article | |||
| [10] | Janati G., Bellemkhannate S. Integration esthétique de la prothèse complete : Intérêt de la prothèse immédiate et des empreintes à visée esthétique. Le Courrier du dentiste 2012. | ||
| In article | |||
| [11] | Bissasu M. A simple procedure for minimizing adjustment of immediate complete denture: a clinical report. J Prosthet Dent. août 2004; 92(2): 125-7. | ||
| In article | View Article PubMed | ||
| [12] | Berteretche M, Hüe O. La prothèse complète immédiate : une entité, mais différentes approches. Cah Proth. 1998; (104): 89-101. | ||
| In article | |||
| [13] | Hüe O, Berteretche M. Prothèse complète: Réalité clinique, Solutions thérapeutiques. Paris: Quintessence; 2003. | ||
| In article | |||
| [14] | Hüe O, Braud A, Berteretche M. Prothèse complète immédiate : comment gérer l’esthétique? Strat Prothétique. avr 2007; 7(2): 111-20. | ||
| In article | |||
| [15] | Sadowsky S. Use of foil to block out extraction sites prior to relining immediate dentures. J Prosthet Dent. janv 2006; 95(1): 79. | ||
| In article | View Article PubMed | ||
| [16] | Sadowsky S, Gupta S, Gonzales E. A technique to correct incisal plane error in maxillary immediate denture therapy. J Prosthet Dent. août 2013; 110(2): 141-3. | ||
| In article | View Article PubMed | ||
| [17] | Postaire M, Demurashvili G, Vicaux F, Raux D. La prothèse complète immédiate mandibulaire, une solution simple... et efficace. Strat Prothétique. Mars 2010; 10(2): 139-46. | ||
| In article | |||
| [18] | Postaire M, Herbout B. Intérêt de la précision dans la détermination et dans l’enregistrement du rapport mandibulo-maxillaire chez l’édenté total. StratProthétique. juin 2016; 16(3): 197-202. | ||
| In article | |||
| [19] | Postaire M, Pompignoli M. Les dernières dents... Garder ou extraire : solutions cliniques. Paris: Espace ID; 2011. | ||
| In article | |||
| [20] | Viennot S, Moyencourt C, Millet C, Buch D. Réhabilitation esthétique et fonctionnelle par prothèse complète immédiate : étapes cliniques. juin 2004; (126): 9-18. | ||
| In article | |||



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}