 sciepub.com
sciepub.com
 Quick Submission
Quick Submission

Preventing Repeat Abortions among Women in Kumasi, Ghana
Agyei Helena1, , Dr. Easmon Otupiri1, Dr. R. E. Larson-Reindorf1
, Dr. Easmon Otupiri1, Dr. R. E. Larson-Reindorf1
1Department of Community Health, SMS-KNUST, Kumasi, Ghana
Abstract
Induced Abortion which constitutes 10% of maternal mortality in Ghana presents a serious health problem particularly among women within 20-24 years presenting at Komfo Anokye Teaching Hospital (KATH), Kumasi. To accelerate progress towards achieving MDG 5 there must be substantial reduction in induced abortion alongside an increased contraceptive uptake, Post Abortion Care. Barriers to contraceptive use were as a result of; fear of side effect, inaccessibility, socio-economic factors, bad social prescripts and poor service delivery. The output, unintended pregnancies ended in induced abortions. The desire to delay, space and end childbirth are reasons giving for having an induced abortion suggesting high unmet need for FP.
Keywords: self-induced, spontaneous, abortion, post-abortion, contraceptive useZ
Copyright © 2016 Science and Education Publishing. All Rights Reserved.Cite this article:
- Agyei Helena, Dr. Easmon Otupiri, Dr. R. E. Larson-Reindorf. Preventing Repeat Abortions among Women in Kumasi, Ghana. American Journal of Public Health Research. Vol. 4, No. 1, 2016, pp 8-15. http://pubs.sciepub.com/ajphr/4/1/2
- Helena, Agyei, Dr. Easmon Otupiri, and Dr. R. E. Larson-Reindorf. "Preventing Repeat Abortions among Women in Kumasi, Ghana." American Journal of Public Health Research 4.1 (2016): 8-15.
- Helena, A. , Otupiri, D. E. , & Larson-Reindorf, D. R. E. (2016). Preventing Repeat Abortions among Women in Kumasi, Ghana. American Journal of Public Health Research, 4(1), 8-15.
- Helena, Agyei, Dr. Easmon Otupiri, and Dr. R. E. Larson-Reindorf. "Preventing Repeat Abortions among Women in Kumasi, Ghana." American Journal of Public Health Research 4, no. 1 (2016): 8-15.
| Import into BibTeX | Import into EndNote | Import into RefMan | Import into RefWorks |
At a glance: Figures
1. Introduction
Promoting post-abortion contraceptive uptake is a key intervention for improving the health of all women and children. Contraceptive uptake plays an important role in reducing fertility. Contraceptive use, however, is the consequence of contraceptive acceptance, method choice, continuation, switching and failure. The use of contraceptive methods to prevent unintended pregnancies is one of the most effective strategies to reducing induced abortion rates, maternal morbidity and mortality. Thus, the provision of post-abortion family planning services that include counselling with easy access to contraceptive methods are suitable to determine the acceptance and selection of contraceptive methods by women who have had induced abortion.
PAC services have historically sought to reduce maternal mortality by treating the symptoms of haemorrhage and sepsis rather than by treating women's unmet need for family planning thus overlooking the potential of Post-abortion care to interrupt the cycle of repeat unplanned pregnancy, abortion and complications leading to maternal death.
For many post-abortion patients, the lack of family planning counselling and services quickly leads to another induced abortion, because fertility returns within four to six weeks after miscarriage or induced abortion.
Induced abortion remains pervasive and damaging condition in the low-income and middle-income countries where mostly abortion is illegal. In Ghana unsafe abortion remains a major public health problem despite apparent liberalisation of the law on abortion over two decades. Though abortion is legal in Ghana, women still obtain unsafe abortions (The Alan Guttmacher Institute, 1999) due to lack of knowledge at the provider and population levels. Most women, especially in the developing world have misconception together with other factors that influence the use of contraception which makes post-abortion care deficient and calls for the need to be incorporated into practice for Ghana to attain the MDG 5.
Contraception is one of the major determinants of fertility levels. Its use has been increasing steadily since 1970 and is currently widespread throughout the world. However, progress has been uneven across geographical areas and great challenges remain in terms of both increasing the level of contraceptive use to satisfy existing needs in certain regions and in terms of making available an adequate variety of contraceptive methods to increase the ability of individuals wishing to use contraception to do so in a consistent and efficient manner. Post-abortion contraceptive uptake is proposed as a strategy to avert unintended pregnancy and the practice of self-induced abortion which dates back to ancient times.
Worldwide contraceptive prevalence, the percentage of women using contraception among women of reproductive age who are married or in a consensual union is estimated to have reached 61 per cent in 1998, the average date for the most recent data available in 160 countries. However, this global average masks important disparities across and within developmental groups, major areas and regions.
In Africa, low levels of contraceptive use have persisted since the early 1970s in the countries of Eastern, Middle and Western Africa. Significant increases did not start in those regions until the late 1980s or early 1990s; a development that explains why 87 per cent of the countries in Africa with data on trends still had contraceptive prevalence levels below 30 per cent in 2000.
Studies in Africa, Latin America and Russia have demonstrated an uptake of post abortion contraception of over 50% and as high as 87% among women who have received abortion care (whether for complications of spontaneous or induced abortions) and who are offered contraception prior to discharge from the health care facility, even when contraceptive use is relatively low across all women of reproductive age.
In Zimbabwe, a study showed that offering contraception to women at the time of post-abortion care prevented more unplanned pregnancies and repeat abortion in a one year period compared with women who did not receive contraceptive services at the same time or location of their treatment for abortion complications suggest there are sufficient service delivery points to provide decentralised abortion care, but that the full range of necessary abortion care services may not be provided at all these sites.
The 2008 Ghana Demographic and Health Survey (GDHS) showed an increase in contraceptive use among currently married women in Ghana, from 13.0 per cent in 1988 to 23.5 per cent in 2008. Similarly, an increase in the proportion of sexually active unmarried women using a contraceptive method was noted between 2003 and 2008, from 43.5 per cent to 50.4 percent. This increase in contraceptive use is encouraging; however, studies suggest that Ghana's contraceptive prevalence rate (CPR) is still too low to have solely led to the observed reduction in fertility levels from 1988 to 2008. Induced abortion, however, (taken together with contraceptive use) could explain this decrease in fertility.
The level of unmet demand says little about either overall demand or the level of contraceptive use. In both Botswana and Uganda, for example, unmet demand is estimated at 27%: but in Botswana the overall demand is 60% of which 33% is met, whereas in Uganda the overall demand is 32% of which only 5% is being met (DHS, 1994).
Ghana’s total fertility rate has declined steadily since 1990; 5.21993, 4.41998, 4.42003, 4.02008. Decreases in total fertility rates-TFR are expected to be matched by increases in contraception prevalence rates-CPR but this has not happened all the time in Ghana; 10%1993, 13%1998, 19%2003 and 17%2008 (modern methods) Source: GDHS 1993; GDHS 1998; GDHS 2003; GDHS 2008. Induced abortion is suspected for this mismatch since some women still use induced abortion as a means of birth control.
Barriers to contraceptive use exist across a wide variety of country settings but the specific barriers to use vary depending on the country as well as the life stage of different women within that country.
Contraception could avert unintended pregnancy and the practice of self-induced abortion whereas contraceptive non-use might lead to unintended pregnancy which would intend lead to self-induced abortion and later result in maternal mortality or morbidity.
It has been established that the prevalence and effectiveness of contraception is important in predicting unintended pregnancy and the abortion rate. Thus, use of effective contraceptive methods is essential in preventing unintended pregnancies that are later voluntarily terminated. However, recent data reveal that among women who experienced an induced abortion between 2002 and 2007, about 70 per cent failed to use a method prior to the terminated pregnancy. Twenty-eight per cent of women used a method but reported experiencing contraceptive failure.
Post-abortion contraceptive counselling is a critical point of intervention and service delivery and provides a powerful rationale for PAC services. In practice, however, treatment of complications is usually the sole focus and family planning is often neglected. It is essential to restore the family planning component to PAC services, not only to prevent repeat unintended pregnancy and abortion, but also because it is integral to achieving the Millennium Development Goals, other health objectives reducing maternal morbidity and mortality, mother-to-child transmission of HIV and new HIV infections.
Again, services could produce cost savings as well as rapid results, women and communities should demand quality PAC services that provide them with accessible, cost-effective post abortion family planning services that can assist them in reducing unplanned pregnancy and repeat abortion, reduce new HIV infections, improve the health of a woman's next child and ultimately improve the health of her family.
The whole of Africa needs research-based evidence and technical advice to the government in the development of its national health policies and programs. The results of the Navrongo experiment demonstrated that affordable and sustainable means of combining nurse services with volunteer community action can accelerate attainment of the United Nations Millennium Development Goals (MDGs).
There is still the need for the Government of Ghana to initiate programmes in the effort to reach its MDG5 goal by 2015, with particular focus on the reduction of maternal morbidity and mortality due to unsafe abortion by improving access to and the quality of contraceptive services.
A woman who has had induced abortion and has been counselled on contraceptive use will use contraceptive.
2. Methods
The data were analyzed using SPSS version 16. The Pearson Correlation Coefficient test was used to compare variables with level of significance set at p<0.05 and other data were then expressed in simple percentages.
Cross-sectional study design was used to assess factors influencing contraceptive uptake among women presenting at KATH. The study population comprised all women within the age range of 15-49 years presenting with abortion in KATH. The target population is all women with induced abortion.
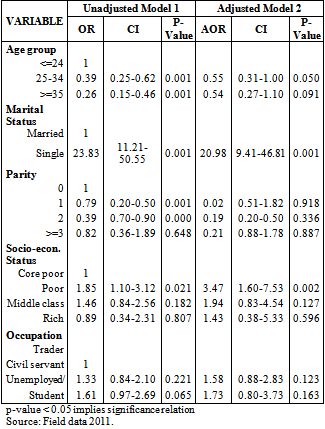
A multi-linear regression analysis model was used to determine the relationship between factors influencing contraceptive uptake among women with induced abortion. Logistic regression analysis will then be used to estimate odds ratios (ORs) with 95% confidence intervals (CIs) and significant (p< 0.05) the bivariable analysis for associations between the participants' characteristics at the time of the interview and their reported history of contraceptive uptake. The analysis was adjusted for primary sampling units and population weights.
3. Results
Most of the respondents from the ages of 20-24, had never used contraceptives or were on any contraceptives as at the time of the study thus 27 out of 127 from 20-24 years used contraceptives.
The study reported that less than a half (182 (43.3%)) of 420 interviewed were married and out of 252 who had induced abortion, only 26 were married in addition to 89 cohabiting with their partners. Majority 130 were single.
With regard to education, majority of the respondents 270 (64.3%) had primary education and 176 (41.9%) were traders whilst 95 (22.6%) were artisans, 58 (13.8%) were unemployed and 38 (9.0%) were students.
From the category of abortion considered in this study, “induced abortion” had the higher recording of 252 (60.0%) as against 168 (40%) representing “not induced abortion” (miscarriage) group.


)



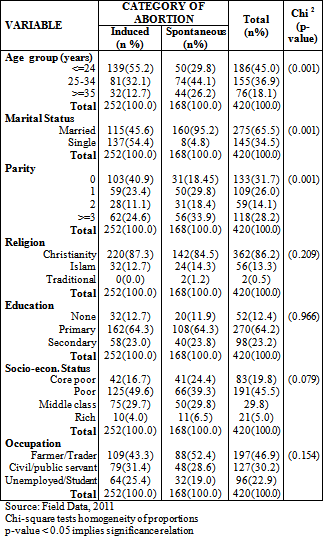

In terms of socio-economic status, 83 (19.8%) of the respondents were very or core poor in the society, 191 (45.5%) of the respondents were poor whilst 125 (29.8%) were middle class in the society. However, only 21 (5.0%) respondents were rich. In all, about 65.3% of the respondents did not have the financial power to seek somewhat safe abortion in the society.
Among the 420 respondents who were interviewed, majority 153 (36.5%) sought information from health workers. 111 (26.5%) and 35 (8.4)% of the respondents sought information from the media and relatives respectively. Only (2.9%) of the respondents sought information from books. On the contrary, 108 (25.8%) sought information from friends.
It was found that, 60.2% of the respondents did not plan the index pregnancy and never used any contraceptive. This is a reflection of the high rates of termination of unintended pregnancies due to non-use (unmet need) of contraceptive. On the contrary, only 39.8% of the respondents planned their index pregnancies.
Most of the respondent’s partners, 404 (96.2%) were not on contraceptive or did not use contraceptive before the index pregnancy and about 88.3% did not also allow their female partners to use contraceptives. Only a few respondents 140 (33.3%) had ever used modern contraceptives to prevent unwanted pregnancies. However, majority of the respondents 339 (80.7%) had the desire to be on contraceptive.
Out of the 420 respondents, 64.8% had no knowledge or were not aware of safe abortion services whereas only 35.2% had knowledge or were aware of safe abortion services. Three hundred and ninety-five (94.0%) decided to seek termination from the hospital whilst 25 (6.0%) of the respondents decided that they would seek termination elsewhere other than the hospital in case they became pregnant and were not ready to give birth.
Table 2. Follow-up assessment of post-abortion contraceptive non-use among women with induced abortion (n=252)

)

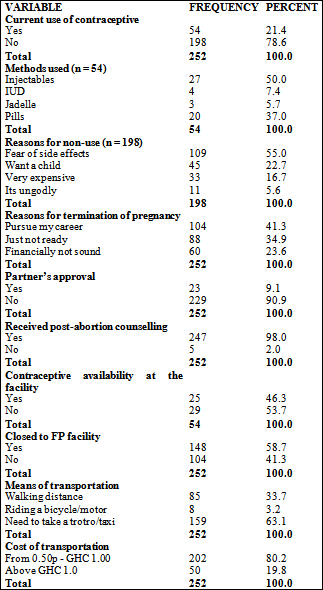

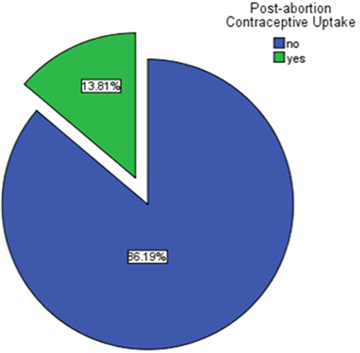
Among the 252 respondents who had induced abortion, only 54 (21.4%) took up contraceptives whilst the majority, 198 (78.6%) were still not using contraceptive even though they wanted to prevent unwanted pregnancies.
Table 3. Characteristics of women presenting with induced abortion verses those presenting with spontaneous abortion



 Download as
Download as
Moreover, over 50% of the respondents used short term contraceptive methods such as pills and injectables whereas 7.4% and 5.7% used IUD and Jadelle respectively. Reasons gathered from the respondents showed that 109 (54.8%) were afraid of side effects of contraceptive use. About 17.1% and 5.5% of the respondents claimed that the use of the contraceptive was expensive and ungodly respectively.
However, 22.6% of respondents wanted children so they did not use any contraceptives. Almost everybody, 98.0% was given counseling by the health provider before discharge home. Among the 54 respondents who were given contraceptives at the facility, 66.7% claimed they were methods of their choice whilst 33.3% claimed the methods were recommended to them. Majority, 208 (82.5%) of the respondents were somewhat close to a family planning facility and were either walking, riding a bicycle/motor or taking a trotro/taxi with 137 (80.6%) paying between 0.50p-GHC 1.00 and only 19.4% paying above GHC 1.00.
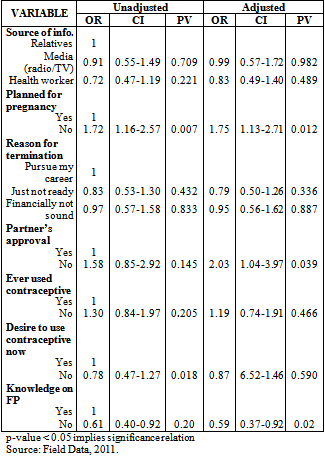
The method of contraceptive used by respondents (p= 0.000), the right of respondents to choice (p=0.000), their means of transportation (p= 0.015), the cost of transportation (p=0.009), partner’s approval to respondent’s use of contraceptive and the desire of respondents to use contraceptive (p=0.018) were significantly related to post-abortion contraceptive uptake.
However, reasons for non-use, partner’s use of contraceptives, counselling given by health worker, distance of clients to FP facility, availability of contraceptive at the facility and the right of respondents to choice did not have any significant influence; reasons for non-use (p=0.329), partner’s use of contraceptives (p=0.471), counselling given by health worker (p=0.238), distance of clients to FP facility (p=0.149) and availability of contraceptive at the facility (p=0.349) on post-abortion contraceptive uptake.



The plan of the index pregnancy (p= 0.000) and whether they intentionally induced the abortion (p= 0.000) were significantly related to the category of abortion. On the contrary, their sources of information about how to get rid of an unwanted pregnancy did not have any significant influence (p= 0.373) on the category of abortion, i.e. either induced or not induced.
A woman who has had induced abortion and has been counselled on contraceptive use will use contraceptive. Ideally those who induce abortion are supposed to be on contraceptives but the outcome was not so as hypothesised in this study.
Helping women to continue contraception safely and effectively is desirable both from an ethical and public health perspective because it reduces unintended pregnancies, self-induced abortion, maternal mortality and morbidity.
4. Discussion
Post-abortion contraceptive uptake could go a long way to reduce maternal mortality particularly, among women with unsafe abortion. Majority of the respondents irrespective of their ages were involved with self-induced abortion and contraceptive non-use. However, the age group 20-24 with the mean age of 22 had the highest recording of 100 out of 127 for contraceptive non-use and 45-49 age group had the least recording of 1 out of 4.
Also in sub-Saharan Africa, it was estimated that 14 million unwanted pregnancies occur every year with almost half occurring among women aged 15-24 years. The younger age groups were likely to be associated with single/cohabiting status, lower socio-economic status, low education level and high socio-cultural influence (partner’s influence) on contraceptive uptake which increased the likelihood to induced abortions. A Ghanaian woman may not be willing about carrying a pregnancy to full term because her partner denies responsibility, she is not ready to marry or her family perceives childbearing outside of marriage as unacceptable. For instance, Ghanaian cultural setting/society tends to disapprove of a mother's sexual behavior if both she and her daughter are nursing infants at the same time.
Of all the 420 respondents interviewed more than half had poor knowledge on reproductive health. Even though 111 had information from the media, some still resorted to induced abortion. That is 108sought information from friends and the rest from other places.
Hogerzeil has argued that a right informed application of the essential medicine concept would demand that particular vulnerable groups are considered. And indeed young people have not been given the necessary attention by policy makers and service providers as said by Sundby, 2006.
From this study it was found that poor quality of contraceptive services including lack of information was a reason for low contraceptive uptake leading to unintended pregnancies, some of which ended in abortion. As unmarried adolescents are not supposed to be sexually active on the basis of cultural norms/traditions, some of the respondents also used other abortifacient before coming to the hospital.
The cost of abortion extend well beyond those of the health system, societies bear the economic cost of lower productivity caused by long term disability and mortality.
It was found that, out of 252, only 26 were married in addition to 89 cohabiting with their partners who intentionally induced abortion were not on contraceptives due to the fact that the respondents were not ready or did not plan the index pregnancy.
Among those who planned the index pregnancy, some could not adequately use the contraceptives that were at their disposal. And as stipulated in literature, mere increases in prevalence of contraceptive use need not necessarily mean success in avoiding unwanted or mistimed pregnancies.
There were a large number of these women who wished to postpone pregnancy and also desired to delay childbearing for economic reasons. Yet contraceptive use as a means of spacing or limiting births remained very low.
With regards to socio-cultural issues, 404 respondents’ partners did not use contraceptives and those 16 who used contraceptives did not have any significant influence on the respondents’ contraceptive uptake. Barriers to contraceptive use are often a result of gender inequality that results in poor communication about family planning between partners, social prescripts which prohibit sexual behavior among a certain segment of the population, and poor service delivery. The output, unintended pregnancies, ended in induced abortions.
Majority, 339 of the respondents, had the desire to use contraceptives nevertheless, only 49 as against 371 were allowed by their partners to use contraceptives.
Also, inadequate availability of contraceptives and quality counselling at the facility did not enhance contraceptive uptake among respondents. Thus clients did not have the right to choice. The study also found that women were significantly more likely to accept a method if they had a range of contraceptive options to offer at sites to promote informed choice (Glasier, 2006). The availability of contraceptive counselling immediately after abortion was an important factor in women’s acceptance of a method.
If contraception were accessible, maternal mortality would decline by an estimated 25-35% (Bongaarts J and Westoff C.F, 2008). Thus, PAC would interrupt the cycle of repeat unplanned pregnancy, abortion and complications leading to maternal mortality.
Also, most successful contraceptive method is likely to be the one that the women or partner chooses rather than the one the clinician chooses for them.
The large numbers of unplanned and unwanted pregnancies in the world are not due solely to inadequate contraceptive methods. It is surely true that substandard health services, lack of public education, inadequate provider training, misunderstandings about risks and poor understanding of how people calculate risk, accessibility, and social, cultural, and religious influences on family planning behavior, all can play a role in whether contraception is used or not.
Among those who used contraceptives, over 50% of the respondents used outmoded or short term contraceptive methods such as pills and injectables whereas 7.4% and 5.7% used IUD and Jadelle respectively.
From literature, long term methods have a big impact on unintended pregnancy particularly among the adolescent since fertility returns four to six weeks after abortion and FP has a role to play before a woman becomes pregnant and after abortion or miscarriage.
Again, most of the respondents were not much closer to FP centers and would patronise taxi/trotro at prices from 0.50p and GHC 1. Since those involved were not economically sound and unmarried with virtually low education these ‘high’ prices deterred them from going to the FP centers for just contraceptives which they would pay at a fee. Quiet a number of them claimed they could walk to the FP centers whilst a few would take bicycles/motor bikes.
5. Conclusion
A major challenge to addressing unsafe abortion in Africa is the lack of commitment on the part of governments to promote, protect and respect women’s reproductive rights, including the right to access safe and legal abortion services. This lack of political will affect the availability, accessibility and quality of abortion-related care.
In order to reduce the incidence of induced abortion contributing to maternal mortality in Ghana, there is the need to: (1) educate the public about the major social and public health burdens of unintended pregnancy; and (2) stimulate a comprehensive set of activities at the national and local levels to reduce such pregnancies.
This requires a thoughtful and deliberate response, a pivotal part of which must be the increased, careful and consistent use of some form of contraception or for the highly motivated and the exercise of periodic abstinence. Thus, greater knowledge about reproductive health and in that context, contraception, is essential for providers, consumers and the public at large, if fully informed, free and appropriate choices are to be made about fertility regulation and sexuality.
The incidence of unsafe abortion generally reflects the magnitude of unwanted (unplanned) pregnancies in a particular community. Hence, one of the best ways of effectively minimizing unsafe abortion is to ensure women have easy access to safe, effective and acceptable contraceptive information and services, backed up by policies that promote social justice and equality, enhanced status of women, as well as legislation that decriminalises abortion.
From the data, very few of the respondents had ever used contraceptives. There were misconceptions about the use of modern contraceptives and sustained education must be mounted to reverse this. Data indicated that there waslow over all contraceptive use of 17% in Ghana (GDHS, 2008) with high unmet FP needs of 34%.
There were negative reactions from the partners and society towards pregnant adolescent women. Partners might have been unhappy, indifferent, or surprised about the pregnancies while others refused responsibility. Most parents also were said to be angry with their pregnant daughters these factors coupled with socioeconomic factors of the women, the partners and parents influenced the decision made in seeking abortion.
The women were found to have low level of sex education as well as poor knowledge of reproductive health issues. Sources of information on family planning particularly PAC appeared to be very muchlimited. The core components of PAC comprising: treatment of incomplete abortion, contraceptive counselling and services and community empowerment through community mobilization, were totally not rendered to post-abortion provided clients.
Moreover, the extent of male use of family planning and the nature of men's role in family planning must be examined carefully and critically for involving men actively in family planning. Policies that aim to increase male involvement must be sensitive to cultural values, apply to a decentralized government approach toward information and supplies, include adequate political will and consider the costs and benefits of changing values. A policy, compatible to traditional values should stress the value of male individuals contributing as much as possible for their own and others' welfare.
Community participation is considered important in order to create a feeling of mutual support. Therefore, a sizeable investment will be required for mass distribution of contraceptive information.
The evidence suggested that health service providers should intensify awareness about the use of contraception, highlight the dangers of induced and repetitive abortions, through health education. Thus high rates of unprotected sex would be a threat to achieving the proposed Millennium development goals. In view of this, the following recommendations are suggested:
Health system administrators and policy makers’ first need to learn about and acknowledge the magnitude of the problem of unsafe abortion in the country due to contraceptive non-use to enable them plan ahead to provide the care women need (WHO, 2007).
Public Health advocates can speak out about the need to provide post-abortion care, citing local statistics on women’s deaths and the cost to local hospitals.
Public Health nurses should organized health education programmes to offer family life education, sex education and contraceptive uptake to both men and women at market places, churches, mosque and schools. Schools are viewed as an ideal place for educating youth about the problems of high fertility and about use of family planning methods, such as the condom. Comic books on how to use condoms are suggested as a good source.
Religious organizations should be used to educate people about responsible parenthood and to minimize barriers to use of modern contraception.
Associations should be encouraged to invite health workers and family planning advisors to educate their members on the importance, durability and reliability of using contraceptive.
Mass media campaign can alert the public to the problems of unsafe abortion. Staff at the maternal and child Health should give talk on abortion and its complications in their clinics in local dialect to enlighten the women that abortion is not the best way for family.
Family Planning counselling services should be affordable to women treated for abortion. Women particularly, young people should be given the necessary attention on their reproductive rights by policymakers and service providers.
Men must also be involved actively in contraceptive use. Also they must be involved in health issues arising from pregnancy and delivery to have effective result that is preventing abortion. Contraceptive services must be made accessible and affordable for both men and women to patronise them.
Competing Interests
Financial competing interests• In the past five years have you received reimbursements, fees, funding, or salary from an organization that may in any way gain or lose financially from the publication of this manuscript, either now or in the future? NO
Is such an organization financing this manuscript (including the article-processing charge)? NO
If so, please specify.
• Do you hold any stocks or shares in an organization that may in any way gain or lose financially from the publication of this manuscript, either now or in the future? NO
If so, please specify.
• Do you hold or are you currently applying for any patents relating to the content of the manuscript? NO
Have you received reimbursements, fees, funding, or salary from an organization that holds or has applied for patents relating to the content of the manuscript? NO
If so, please specify.
• Do you have any other financial competing interests? NO
If so, please specify.
Non-financial competing interests• Are there any non-financial competing interests (political, personal, religious, ideological, academic, intellectual, commercial or any other) to declare in relation to this manuscript? NO
If so, please specify.
Authors' Contributions
HA is the principal investigator, she did the entire investigation, conducted the research and the write-up. REL has made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; EO has made substantive intellectual contributions to a published study. He has been involved in drafting the manuscript or revising it critically for important intellectual content and given final approval of the version to be published.
Acknowledgements
Once again, I wish to express my sincere thanks to the Almighty God through whose love, protection and directions have endowed me with all heavenly blessings to act and perform particularly, in this project.
My indebtedness goes to my project supervisors Dr. Peter Agyei-Baffour, Dr. Easmon Otupiri and Dr. R. E. Larsen-Reindorf. I will remain ever grateful to them for their help, guidance, patience and suggestions during the course of this study.
Also, I am grateful to my lovely family whose support, efforts, provisions and advice made this project a reality.
Moreover, I am particularly grateful to all my lecturers especially, Dr. Harry Tagbor and Mr. Emmanuel Nakua at the KNUST, Community Health Department for their reassurance, directions and dedication during my course. There is no funding for this study.
References
| [1] | Adebysoye, C.; Singh, P.M and Audam, S. (1997). Abortion in sub-Saharan Africa Family Planning Perspective. Vol.23. no.4. December 1997. | ||
 In article In article | |||
| [2] | Adewole, R.F., B.A. Oye Adeniran, N. Iwere, A. Oladokun and A. Gbadegesin, 2002. Contraceptive usage among abortion seekers in Nigeria. West Afr. J. Med., 21: 112-114. | ||
| In article | PubMed | ||
| [3] | Alan Guttmacher Institute. Uneven and unequal: Insurance coverage and reproductive health services. New York: Alan Guttmacher Institute, 1994. | ||
| In article | |||
| [4] | Amin R, Li Y, Ahmed AU. 1998. Women’s Credit Programme and Family Planning in Women’s Lives and rapid fertility decline: Some lessons fromBangladesh and Egypt. Population Research and Policy Review 21(4): 275-317. | ||
| In article | View Article | ||
| [5] | Bongaarts J and Westoff CF, The potential role of contraception in reducing abortion, Studies in Family Planning, 2000, 31(3): 193-202. | ||
| In article | View Article PubMed | ||
| [6] | Bongaarts J, Trends in unwanted childbearing in the developing world, New York: Population Council, 1997; and Westoff CF, Unwanted fertility in six developing countries, International Family Planning Perspectives, 1981, 7(2):43-51. | ||
| In article | |||
| [7] | Bongaarts,J. 1991. "The KAP-Gap and the Unmet Need for Contraception." Population and Development Review 17, 2: 293-313. | ||
| In article | View Article | ||
| [8] | Bongaarts, Johansson and Westoff CF. The potential role of contraception in reducing abortion. Studies in Family Planning 2000; 31: 193-202. | ||
| In article | View Article PubMed | ||
| [9] | Boonstra H, Duran V, Gamble VN, Blumenthal P, Dominguez L, Pies C. The “Boom and Bust Phenomenon”: The hopes, dreams, and broken promises of the contraceptive revolution. Contraception. 2000;61(1):9-25. [PubMed] | ||
| In article | View Article | ||
| [10] | Bromham, D.R. and Thompson. (1996) Knowledge and use of secondary contraception among patients requesting termination of pregnancy. British Medical Journal, 306: 556-57. | ||
| In article | View Article | ||
| [11] | Cleland J, Bernstein S, Ezeh A, Faundes A, Glasier A, Innis J. 2006. Family Planning:the 'perfect contraceptive' population, Science, 1977, 169(951):1177-1182. | ||
| In article | |||
| [12] | Cleland J, Kamal N, Sloggett A. 1996. Links between fertility regulation and the clinic for the first time. Sexually Transmitted Infection, 74: 433-34. | ||
| In article | |||
| [13] | Corbett, M.R. and K.L. Turner, 2003. Essential elements of post-abortion care: Origins, evolution and future directions. Int. Family Planning Perspectives, 29: 106-110. | ||
| In article | View Article PubMed | ||
| [14] | Definition of “Abortion". http://wikepedia/uncensored.html. Retrieved 2009. | ||
| In article | |||
| [15] | DHS Program, Women's lives and experience: a decade of research findings from the Demographic and Health Surveys Program, 1994. | ||
| In article | |||
| [16] | Ekanem, A.D., S.J. Etuk and E.J. Utoma, 2005. What proportion of abortion seekers in Calabar are really pregnant. Trop. J. Obstet Gynaecol., 22: 12-15. | ||
| In article | |||
| [17] | Emuveyan, E.F. and E.O. Agbogboroma, 1997. Trends in abortion related maternal mortality in lagos, Nigeria. Trop J. Obstet. Gynaecol., 14: 39-41. | ||
| In article | |||
| [18] | Frost JJ, Henshaw SK and Sonfield A, Contraceptive Needs and Services, National and State Data, 2008 Update, New York: Guttmacher Institute, 2010. | ||
| In article | |||
| [19] | Furuta M, Salway S. 2006. Women’s position Within the Household as a Determinant of Gallen et al. "Men: New focus on family planning programs," JHU/Population Information Program Series J, May/June, 1986. | ||
| In article | |||
| [20] | Ghana Statistical Service (GSS) and Macro International Inc. (MI). Ghana Demographic and Health Survey2003GDHS, Calverton, Maryland, U.S.A: Macro International Inc., 2004, 65-76. | ||
| In article | |||
| [21] | Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF Macro. Ghana Demographic andHealth Survey 2008. Accra, Ghana: GSS, GHS, and ICF Macro, 2009, 79-87. | ||
| In article | |||
| [22] | Gilda Sedgh et al., “Induced Abortion: Estimated Rates and Trends Worldwide, Guttmacher Institute and World Health Organization,” The Lancet, 370, no. 9595 (2007): 1338-45. | ||
| In article | View Article | ||
| [23] | Glasier AF, Cameron ST, Fine PM, et al. Ulipristal acetate versus levonorgestrel for emergency contraception: a randomised non inferiority trial and Meta analysis. Lancet.2010; 375: 555-62. | ||
| In article | View Article | ||
| [24] | Guttmacher Institute. Facts on induced abortion in the United States [fact sheet]. May 2011. Available at http://www.guttmacher.org/pubs/fb_induced_abortion.pdf.Accessed June 21, 2011. | ||
| In article | |||
| [25] | Guttmacher Institute. Improving contraceptive use in the United States. In Brief. 2008 Series, No. 1 April 2008. | ||
| In article | |||
| [26] | Hakim A, Salway S, Mumtaz Z. 2003. Women’s Autonomy and Uptake of Contraception. | ||
| In article | |||
| [27] | Hardon, A. Reproductive rights in practice: A comparative assessment of quality of care. In: Hardon, A. and Hayes, E. Reproductive Rights in Practice: A Feminist Report on Quality of Care. London, Zed Books, 1997. p. 193-222. | ||
| In article | |||
| [28] | Hardon, A. Reviewing quality of care policies. In: Hardon, A., Mutua, A., Kabir, S., and Engelkes, E., eds. Monitoring Family Planning and Reproductive Rights. London, Zed Books, 1997. p. 23-30 | ||
| In article | |||
| [29] | Hatcher RA, Trussel J, Nelson AL, et al. Contraceptive Technology. 19th revised ed. New York, NY: Ardent Media, 2005. | ||
| In article | |||
| [30] | Hatcher, R.A., Rinehart, W., Blackburn, R., Geller, J.S., and Shelton, J.D. The essentials of contraceptive technology. Baltimore, Johns Hopkins School of Public Health, Population Information Program, Jul. 1997. 340p. | ||
| In article | |||
| [31] | Hatcher, R.A., Trussell, J., Stewart, F., Cates, W., Stewart, G.K., Guest, F., and Kowal, D. Contraceptive technology. 17th ed. New York, Irvington Publishers, Inc., 1998. | ||
| In article | |||
| [32] | Heise, L. L. (1997). Beyond acceptability: Reorienting research on contraceptive choice. World Health Organisation, beyond acceptability: Users’ perspectives on contraception inputs (pp. 6–13). Geneva: WHO. | ||
| In article | |||
| [33] | Henshaw, S.K. AND katzive, L; et .al, (1998).The incidence of abortion in Nigeria. Family planning Perspective.Vol.24 No.4 Decenber,1998. | ||
| In article | View Article | ||
| [34] | Henshaw, S.K., S. Singh, B.A. Oye-Adeniran, I.F. Adewole, N. Iwere and Y.F. Cuca, 1998. The incidence of induced abortion in Nigeria. Int. Fam. Plan. Perspect., 20: 156-164. | ||
| In article | View Article | ||
| [35] | Hogerzeil, HV. Essential medicines and Human Rights: What can they learn from each other? Bull WHO 200, 84:371-5. | ||
| In article | View Article | ||
| [36] | ICPD/15 (1994) International Conference on population and Development. Africa Regional Review Report: 15 year Review of the Implementation of the ICPD in Africa. | ||
| In article | |||
| [37] | IPAS, 1991. Strategy for the Next Decade: Women s Health Initiatives. Ipas, Publ., Carrboro, NC, USAin Pakistan. Asia Pacific Population Journal 18(1): 63-82. | ||
| In article | |||
| [38] | JAIN, A. and BRUCE, J. 1989. A reproductive health approach to the objectives and assessment of family planning programs. Increase Contraceptive Practice In: Sen, G., Germain, A., and Chen, L.C. Population Policies Reconsidered: Health, Empowerment and Rights. Boston, Harvard University Press, Mar. 1989. p. 194-209. | ||
| In article | |||
| [39] | JAIN, A. Should eliminating unmet need for contraception continue to be a program priority? International Family Planning Perspectives 25 (Suppl.): S39-43, S49. Jan. 1999. Journal, 306: 556-57. | ||
| In article | |||
| [40] | Kenya National Bureau of Statistics (KNBS) and ICF Macro. 2010. Kenya Demographic and Health Survey 2008-09. Calverton, MD: KNBS and ICF Macro. | ||
| In article | |||
| [41] | Morhee R.A.S. and Morhee E.S.K. Overview of the law and availability of abortion services in Ghana. Ghana Medical Journal 2006; 40: 80-86. | ||
| In article | PubMed | ||
| [42] | Population Reference Bureau. Family Planning Worldwide 2008 Data Sheet. Washington, DC: Population Reference Bureau; 2008. | ||
| In article | |||
| [43] | Potter, Robert G. 1999. “Inadequacy of a One-Method Family Planning Program.” Studies in Family Planning, Vol. 2, No. 1 (January), 1-6. | ||
| In article | View Article | ||
| [44] | Westoff. 1991. The Contribution of Fulfilling the Unmet Need for Family Planning ( The Futures Group/PolicyProject, 1991). | ||
| In article | |||
| [45] | Sedgh, Gilda; et al (2007-10-13). "Induced Abortion: Estimated Rates and Trends Worldwide". The Lancet370 (9595): 1338-45. | ||
| In article | View Article | ||
| [46] | Singh S, Sedgh G and Hussain R, Unintended pregnancy: worldwide levels, trends and outcomes, Studies in Family Planning, 2010, 41(4):241-250. | ||
| In article | View Article PubMed | ||
| [47] | Singh S. (2006). Hospital admissions resulting from unsafe abortion, estimates from 13 developing countries. Lancet, 368 (9550), 1887-1892. | ||
| In article | View Article | ||
| [48] | Starrs, A., 1997. The safe motherhood action agenda: Priorities for the next decade. Report on the Safe Motherhood Technical Consultation, 18-23 October, Colombo, Sri Lanka. | ||
| In article | |||
| [49] | Snowden. 1985., Walsh, 1997. Advances in Contraception. The Official Journal of the Society cont.vol.13, Noso 2/3 pp 81-384, June/Sept 1997, kluwer Academic Publisher. | ||
| In article | |||
| [50] | Sundby J, Olsen A. Infertility, technology and the law. Patients’ and future doctors’ opinions. Acta Obstet Gynecol Scand. 1990; 69: 641-4. | ||
| In article | View Article PubMed | ||
| [51] | Sundby, J (2006). Young Peoples sexual and Reproductive Health Rights. Best Pract Res Clin Obstrct Gynaeco, 20(3), 355-368. | ||
| In article | View Article PubMed | ||
| [52] | Sundby J. Methodological considerations in the study of frequency, risk factors and outcome of reduced fertility. Scand J Soc Med. 1989;17(2):135-40. Review. | ||
| In article | PubMed | ||
| [53] | Sundby J. Sad Not to have Children. Happy to be Childless. A Personal and Professional Experience of Infertility. Reproductive Health Matters. 1999;13:13-9. | ||
| In article | View Article | ||
| [54] | The Alan Guttmacher Institute (AGI), 1999. Sharing Responsibility: Women, Society and Abortion Worldwide. AGI, New York. | ||
| In article | |||
| [55] | Thompson, S., Skinner, K. and Kirkman, R.J.E. (1996) Would you rather be seen by the nurse? British Journal of Family Planning, 22: 130-32. | ||
| In article | |||
| [56] | UN, 2008. The millennium development goals report 2008. New York. http://www.un.org/millenniumgoals/pdf/The%20Millennium%20Development%20Goals%20Report%202008.pdf. | ||
| In article | |||
| [57] | United Nations Population Division/DESA: Fertility and Family Planning Section. World Contraceptive Use 2009: Unmet Need for Family Planning. http://www.un.org/esa/population/publications/WCU2009/Metadata/UMN.htm. | ||
| In article | |||
| [58] | Westhoff C. Depot-medroxyprogesterone acetate injection (Depo-Provera®): a highly effective contraceptive option with proven long-term safety. Contraception. 2003; 68(2):75-87. | ||
| In article | View Article | ||
| [59] | Westoff CF, The unmet need for birth control in five Asian countries, International Family Planning Perspectives, 1978, 4(1): 9-18. | ||
| In article | |||
| [60] | Westoff, CF and Ochoa LH. 1991. Unmet Need and Demand for Family Planning. Demographic and Health Surveys Comparative Studies 5. Columbia, MD: Institute for Resource Development/Macro International Inc. | ||
| In article | |||
| [61] | World Health Organization. (2004b). Contraception: issues in adolescent health and development. In WHO Discussion Papers on Adolescence. Geneva WHO available at http://whql:bdoc.who.int/publications/2004/9241591447_eng.pdf.2010-09-20. | ||
| In article | |||
| [62] | World Health Organization (WHO), Maternal Mortality in 2005: Estimates Developed by WHO, UNICEF, UNFPA and the World Bank (Geneva: World Health Organization, 2007): 1.17-27. | ||
| In article | |||
| [63] | World Health Organisation, WHO (2010). Maternal Mortality, Media Center Fact Sheet No 348 available at http://www.who.int/mediacentre/factsheets/fs348en/index.html2011-03-27. | ||
| In article | |||
| [64] | World Health Organization (WHO), Unsafe Abortion and Post-abortion Care available at http://www.wpro.who.int/interrut/files/pub/360/141.pdf2011-08-02. | ||
| In article | |||
 CiteULike
CiteULike Delicious
Delicious



{kind=link}
{kind=link}